Gamma Knife Radiosurgery: An Adjuvant Therapy for Primary Sellar Paraganglioma
Madan Bajagain, Shingo Fujio, Mari Kirishima, Kazutaka Yatsushiro, Ryosuke Hanaya

TL;DR
Gamma Knife radiosurgery is an effective adjuvant therapy for primary sellar paraganglioma after partial surgical removal.
Contribution
This case study demonstrates the efficacy of Gamma Knife radiosurgery as an adjuvant treatment for primary sellar paraganglioma.
Findings
A TC-TS surgical approach allowed partial resection of a highly vascular sellar paraganglioma.
Gamma Knife radiosurgery stabilized residual tumor growth two years post-treatment.
SP should be considered in the differential diagnosis of pituitary diseases.
Abstract
Sellar paraganglioma (SP) is a rare benign tumor, usually treated by surgery. SPs are lobulated, firm, adherent, and highly vascular, allowing mostly partial resection. We present the case of a 52-year-old man diagnosed with primary SP, treated with a transcranial-transsphenoidal (TC-TS) surgical approach, followed by adjuvant Gamma Knife stereotactic radiosurgery (GKSR). The tumor has an extra-pituitary origin, with a sellar-suprasellar, right cavernous sinus extension that encroached the bilateral optic nerve and anterior cerebral artery. Histopathology confirmed SP with a Zellballen pattern. Despite postoperative tumor growth observed at four and 10 months, a stable residual tumor was noted at a follow-up two years after GKSR. SP is diagnosed mainly in middle age or in adolescent males. The TC-TS approach offers a bidirectional view that allows greater resection by minimizing blind…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
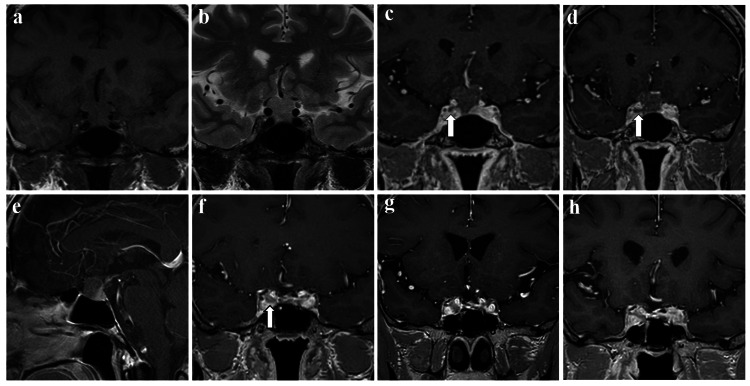 Figure 1
Figure 1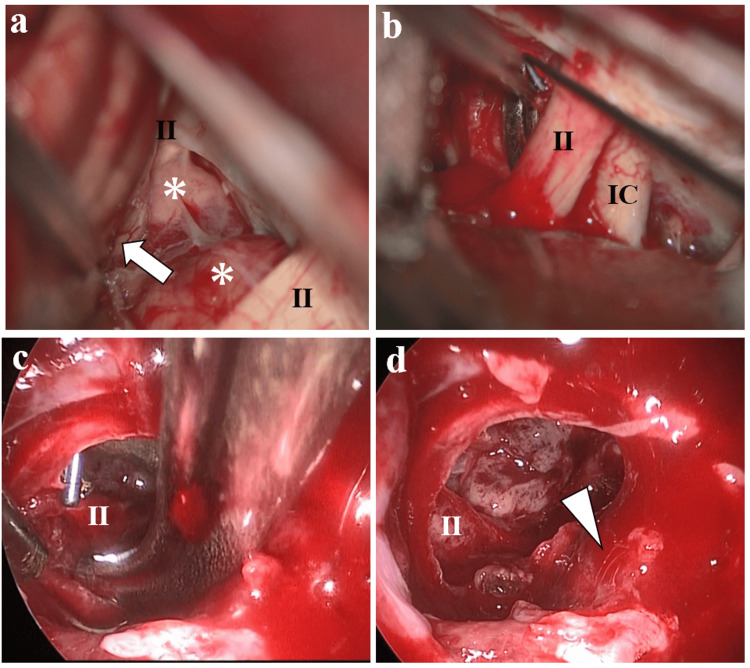 Figure 2
Figure 2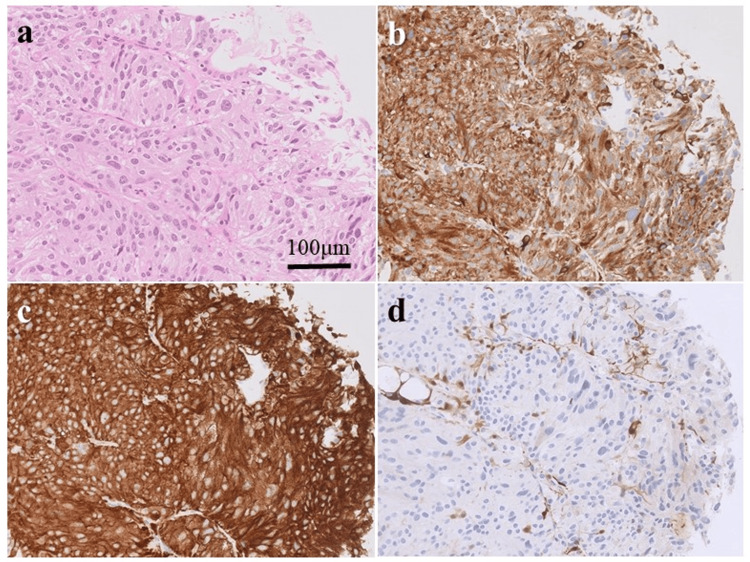 Figure 3
Figure 3| S.N. | First author and year of publication | Age/ Sex | Location | Surgical route/ Approach | STR/ GTR | Radiation therapy/ doses | |
| 1 | Chytil, 1967 [ | 46/M | Sellar / SPS | TS | STR | RT | CRT 40 Gy** |
| 2 | Bilbao et al., 1978 [ | 37/M | Sellar | TC | GTR | No RT | - |
| 3 | Ho et al., 1982 [ | 65/M | CS / semilunar ganglion | TC/ Rt. fronto temporal | STR | RT | CRT 52 Gy |
| 4 | Prabhakar et al. 1984 [ | 7/F | PS, pre and retro sellar | TC/ Rt. fronto temporal | STR | RT | CRT 45 Gy |
| 5 | Steel et al., 1993 [ | 44/F | Sellar, PS, and CS | TS | STR | RT | CRT 45 Gy |
| 41/F | Sellar, PS, and CS | TC/ Lt. fronto temporal | STR | RT | CRT 50 Gy | ||
| 6 | Flint et al., 1993 [ | 17/M | Sellar, SS, CS, and Carotid Sinus | TC/ sub frontal** | Biopsy, STR | No RT | - |
| 7 | Scheithauer et al., 1996 [ | 14/M | Sellar/ SS | TS, 3 m later TC/ Rt. frontal | Biopsy, STR | RT | CRT 50.4 Gy |
| 8 | Noble et al., 1997 [ | 71/M | Sellar | TC/ Rt. fronto- temporo-parietal | STR | ND | - |
| 9 | Mokry et al., 1998 [ | 76/M | Sellar / SS | TS, later TC/ Rt. pterional | STR | No RT | - |
| 10 | Del Basso De Caro et al., 1998 [ | 84/M | Sellar / SS | TS | GTR | No RT | - |
| 11 | Sambaziotis et al., 1999 [ | 54/M | Sellar | TS | GTR | No RT | - |
| 12 | Salame et al., 2001 [ | 48/F | Sellar / SS | TS | STR | No RT | - |
| 13 | Laquis et al., 2001 [ | 15/F | SS, CS | TC/ skull base | STR | RT | ND |
| 14 | Hertel et al., 2003 [ | 51/F | Sellar/ SS/ Middle cranial fossa and clival | TC/ Lt. trans-sylvian** | STR ** | RT | fSRT |
| 15 | Arkha et al., 2003 [ | 58/F | Sellar/ PS | TC/ Lt. fronto- temporal | STR | No RT | - |
| 16 | Naggara et al., 2005 [ | 47/M | Sellar / SS | TC/ temporal | GTR | No RT | - |
| 17 | Zorlu et al., 2005 [ | 37/M | Sellar / PS | Multiple surgeries | GTR*** STR* | RT | CRT 50 Gy |
| 18 | Boari et al., 2006 [ | 52/M | Sellar | Sub-labial TS | STR | No RT | - |
| 19 | Voulgaris et al., 2006 [ | 48/M | Sellar / SS | TC/ fronto- temporal | STR | RT | ND |
| 20 | Peltier et al., 2007 [ | 51/F | PS | TC/ Lt. sub-frontal | STR | RT | CRT 45 Gy |
| 21 | Sinha et al., 2008 [ | 18/M | Sellar, SS and CS | TS | STR | No RT | - |
| 22 | Özüm et al., 2008 [ | 70/M | Sellar/ PS with B/L CS | TS | STR | RT | CRT 50 Gy |
| 23 | Haresh et al., 2009 [ | 17/M | Sellar/ PS | TS | STR | RT | fSRT 50 Gy 25f |
| 24 | Albert et al., 2011 [ | 63/M | Sellar/ PS with orbital extension | TC/ orbital osteotomy | STR, GTR | No RT | - |
| 25 | do Nascimento et al., 2012 [ | 33/F | Sellar | TS, 2 m later TC/ sub frontal | GTR | No RT | - |
| 26 | Li et al., 2017 [ | 40/F | Sellar / SS | TC/ sub-frontal | STR | RT | CRT 50 Gy |
| 27 | Karlekar et al., 2018 [ | 19/M | Sellar, PS with pontine extension | TC** | STR** | RT | ND |
| 28 | Lyne et al., 2019 [ | 73/F | Sellar / SS | TS | GTR | RT | ND |
| 29 | Vasoya et al., 2020 [ | 13/M | Sellar / SS | TC/ Left pterional | Biopsy | RT | CRT 50 Gy 25f |
| 20/M | Sellar / SS | TC/ Left pterional | Biopsy | RT | CRT 40 Gy 20f | ||
| 30 | Wang et al., 2023 [ | 70/F | Sellar / PS / SS | TC/ sub-frontal | STR | No RT | - |
| 31 | Current case | 52/M | Sellar/ PS | Combined TS-TC / Rt. pterional | STR | RT | GKSR 15 Gy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPituitary Gland Disorders and Treatments · Meningioma and schwannoma management · Adrenal and Paraganglionic Tumors
Introduction
Primary sellar paraganglioma (SP) is a rare benign pituitary disease derived from neural crest progenitor cells [1]. The usual modality of treatment for SP is surgical resection using a transcranial (TC) or transsphenoidal (TS) approach. However, in most previous cases, only partial resections or biopsies were achieved due to the firm consistency, adherence, and high vascularity of the tumor [2,3]. SP may also exhibit recurrence and usually requires adjuvant radiation therapy. Here, we present a case of a primary SP treated with adjuvant Gamma Knife stereotactic radiosurgery (GKSR) after a TC-TS surgery.
This article was previously presented as a meeting abstract at the 32nd Annual Meeting of the Japanese Society for Hypothalamic and Pituitary Tumors on February 18, 2022.
Case presentation
A 52-year-old man with occasional headaches underwent head computed tomography (CT) that revealed a sellar mass. Magnetic resonance imaging (MRI), performed following routine pituitary MRI protocol [4], showed a solid tumor extending into the sellar-suprasellar region with an isointense signal on T1- and T2-weighted imaging (Figure 1a, 1b). The tumor encroached on the A1 segment of the anterior cerebral artery on both sides, compressing the bilateral optic nerves. T1 contrast imaging suggested that the tumor had an extra-pituitary origin, with a normal pituitary gland located laterally and caudally (Figure 1c-1e). The contrast effect of the tumor was weak, and the dynamic study also showed minimal tumor contrast. Tumor invasion into the right cavernous sinus was suspected (Figure 1c, 1d).
Gradual changes on magnetic resonance imaging(a, b) At the initial visit, coronal images showed a solid tumor extending into the suprasellar region (a: T1-weighted, b: T2-weighted); (c, d, e) T1 contrast images showed an extra-pituitary origin of the tumor with the normal pituitary gland and the stalk situated caudally to the left (c, d: coronal, e: sagittal). The contrast effect of the tumor was weak. Tumor invasion into the right cavernous sinus was suspected (arrow in c and d); (f, g) Postoperative T1 contrast coronal images revealed a residual tumor in the right cavernous sinus (arrow in f), which increased in size (f: four months: maximum tumor size was 4 mm, g: 10 months: maximum tumor size was 7 mm); (h) Coronal T1 contrast images taken two years after Gamma Knife stereotactic radiosurgery showed no further tumor growth (The maximum tumor size was 6 mm).
The basal pituitary hormonal profile was normal. Further, an ophthalmological examination revealed no visual field defects. The first differential diagnosis was an ectopic pituitary adenoma. However, the tumor was less contrasted, which is atypical in pituitary adenomas. Rare tumors were also considered as differentials. Due to concerns about unusual postoperative bleeding and adhesion between the optic nerve and tumor, a combined TC and endoscopic TS surgery was performed.
The TC surgeon was positioned at the head of the operating table, whereas the TS surgeon was on the right side. The patient’s head was fixed in a Mayfield clamp and tilted 15° towards the left in a supine position. A high-definition endoscope (Karl Storz SE & Co. KG, Tuttlingen, Germany) was used to perform standard endoscopic endonasal TS surgery. After dissecting the bilateral nasal mucosa, the septal bone was harvested for sellar plasty. Next, the sella and dura were opened with a cruciate incision. The tumor center was soft, similar to a pituitary adenoma; however, the margins were fibrous and firm. The tumor border with the pituitary gland was easily detached; nonetheless, adhesion with the bilateral optic nerve, A1 segment of the anterior cerebral artery, and rectal gyrus was observed. The TC surgeon used the right pterional approach to dissect the tumor off the optic nerve, A1 segment of the anterior cerebral artery, and rectal gyrus, facilitating safer tumor resection and removal (Figure 2). Tumor invasion into the cavernous sinus was evident and excised as much as possible by the TS surgeon. The perioperative tumor bleeding was similar to that of a usual pituitary adenoma surgery. Adequate tumor removal with intact cavernous sinus was achieved.
Intraoperative views of the transcranial side (a, b) and transsphenoidal side (c, d)(a) The tumor was located between the optic chiasm and attached to the left and right optic nerves (asterisk) and rectal gyrus (arrow); (b, c) The tumor under the right optic nerve was dissected via the transcranial approach and removed via the transsphenoidal route; (d) Final view. No tumor invasion into the pituitary gland was observed (arrowhead).II: optic nerve, IC: internal carotid artery.
Histopathological examination revealed tumor cells with abundant cytoplasm, arranged in a nested Zellballen pattern (Figure 3a). Tumor cells were immunopositive for chromogranin A (Figure 3b) and synaptophysin (Figure 3c), whereas sustentacular cells surrounding the tumor were positive for S100 proteins (Figure 3d) and glial fibrillary acidic protein. Most tumor cells were negative for cytokeratin AE1/AE3 and anti-cytokeratin antibody 5.2, epithelial membrane antigen, vimentin, thyroid transcription factor-1, cluster of differentiation34, and signal transducer and activation of transcription6. The MIB-1 index was 2%; therefore, a diagnosis of SP was made.
Pathological findings(a) Hematoxylin-eosin staining shows cytoplasmic tumor cells with a Zellballen appearance with large polymorphic nuclei and multinucleated cells; (b–d) Immunostaining showing tumor cells positive for proteins (b: chromogranin A, c: synaptophysin, d: S-100).
Whole-body CT and meta-iodobenzylguanidine scintigraphy revealed no detectable lesions with normal levels of urine metanephrine and normetanephrine. Corticotropin-releasing hormone, luteinizing hormone-releasing hormone, and thyrotropin-releasing hormone tests were performed three months after surgery; nevertheless, no decrease in anterior pituitary function was observed. Postoperative MRI at four months showed a residual tumor confined in the right cavernous sinus (Figure 1f), which increased in size at 10 months (Figure 1g).
GKSR with a marginal dose of 15 Gy was chosen over a second surgery as tumor regrowth was limited to the cavernous sinus. Two years after GKSR, no additional tumor growth was observed (Figure 1h). The pituitary function was also preserved.
Discussion
Paragangliomas are benign neuroendocrine tumors that arise from paraganglionic tissue, constituting only 0.6% of all head and neck region tumors [5]. They are primarily located in the carotid body (60% to 70%), the jugular glomus, and along the vagus nerve [2]. SPs are relatively rare due to the absence of paraganglia in the sellar region, their origin and disease causation remain unknown. Meta-iodobenzylguanidine scintigraphy is a useful diagnostic tool for neuroendocrine tumors like paragangliomas [6]. However, this case exhibited no accumulation other than that in the pituitary gland, and the disease appeared to be primary.
A literature review on sellar region paraganglioma (excluding metastasis) yielded 30 reports, comprising 32 patients (Table 1).
Most patients with SP were diagnosed in middle age (40-59 years, 38.70%) or adolescence (10-19 years, 22.58%). SP is predominantly seen in males (65.63%), with a male-to-female ratio of 1.9:1, contrasting with the female-predominant carotid, vagal, tympanic, and laryngeal paragangliomas [34,35]. SP tumors are lobulated, firm, and highly vascular, with or without a capsule [1,33]. They are adherent to the carotid artery, cavernous sinus, and optic nerve, which extends to the extra sellar locations [2,3,33]. Although the exact origin of the SP is unknown, in the current case, the border between the tumor and the pituitary gland was clear, and the tumor extended into the cavernous sinus, suggesting that it may have originated from within the cavernous sinus. MRI of SP shows heterogeneous intensity on T2 with gadolinium enhancement, indicating high vascularity [12,32,33]. However, the findings were atypical for the present case, with a weak contrast effect and minimal enhancement in dynamic studies.
The primary treatment modality for SP is surgical resection via the TC or TS route. The preferred surgical approaches for TC were sub-frontal and trans-pterional. Preoperative endovascular embolization to devascularize the SP followed by TS resection is a plausible treatment option. In the late 20th-century case reports, SP patients were treated via both the TC [8-13] and TS [1, 7,11,14-16] routes equally (n=6 each). However, since 2000, more patients with SP have been treated via the TC route (13 patients, 65%) [3,18-22,24,28,30-33] rather than the TS route (seven patients, 35%) [2,17,23,25-27,29]. The primary treatment choices for SP are biopsy (12.5%), subtotal resection (65.6%), or gross total resection (21.9%). These facts show that reaching a consensus to follow a TC or TS route to achieve adequate tumor resection can be challenging. Recently, combined TC-TS surgeries have been employed for anterior skull-base tumors that include meningiomas, giant pituitary adenomas, and craniopharyngiomas [36]. The combined TC-TS approach allows bidirectional views for greater resection by minimizing blind spots and reducing residual tumor masses in the tumor bed. This prevents post-operative bleeding, particularly when the tumor extends beyond the capsule intracranially [36,37]. Surgical manipulation from two directions also facilitates precise dissection along the carotid artery and optic nerves [36,38]. The TS approach alone involves a high risk for postoperative hemorrhage, edema, and mass effects if radical resection is not achieved [37]. The tumor, in the current case, was without a capsule, encroached on the A1 segment of the anterior cerebral artery, and compressed the bilateral optic nerves, which guided our decision to pursue a combined TC-TS approach. Despite many previous reports achieving partial resections, we chose the combined technique for its potential to allow a gross safer resection despite the complex anatomical involvement.
A literature review on post-surgical adjuvant radiation therapy yielded 18 patients: four lacked relevant data [2,3,18,31], two received fractionated stereotactic radiation therapy [19,27], and the rest received conventional radiation therapy [1,7,9-11,22,24,26,30,32]. Most patients who underwent biopsy and subtotal resection (75% and 66.5%, respectively) received radiation therapy as an adjuvant. GKSR is effective for pituitary adenomas, metastatic tumors, meningiomas, schwannomas, and other benign tumors [39]. Additionally, GKSR is effective in treating paragangliomas found at other sites. A literature review of patients treated with GKSR for glomus jugulare tumors showed that 90.5% had tumor control [40]. Similarly, another study of 55 patients with a mean follow-up of 86.4 months had 94.8% of tumor control for jugulotympanic paragangliomas [41]. However, GKSR has neither been previously utilized nor reported in the literature for the treatment of SP recurrence. GKSR plays a crucial role in stabilizing tumor growth and preserving surrounding structures, especially in surgically inaccessible locations, such as the right cavernous sinus in this case. Follow-up MRI two years after the GKSR showed a stable tumor. This case provided an opportunity to investigate the effectiveness of GKSR in stabilizing SP recurrence. Further studies are warranted to elucidate the potential of GKSR as a novel therapeutic modality in this context.
Conclusions
SP is a rare disease that should be considered in pituitary pathology, particularly in adolescent and middle-aged men. Complete surgical removal of a tumor is generally unattainable via the TC or TS approach alone. Hence, a combined simultaneous TC-TS surgical approach can enable a near-complete and safer resection. GKSR plays a crucial role in treating SP growth in surgically inaccessible locations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intrasellar paraganglioma: report of a case in a sibship of von Hippel-Lindau disease Neurosurgery Scheithauer BW Parameswaran A Burdick B 395399381996886907110.1097/00006123-199602000-00034 · doi ↗ · pubmed ↗
- 2Primary sellar paraganglioma: case report with literature review and immunohistochemistry resource World Neurosurg Lyne SB Polster SP Fidai S Pytel P Yamini B 323612520193070359210.1016/j.wneu.2019.01.094 · doi ↗ · pubmed ↗
- 3Suprasellar and intrasellar paragangliomas Clin Neuropathol Voulgaris SG Partheni M Tzortzidis F Ravazoula P Pessach IS Papadakis N Polyzoidis KS 221226252006 https://pubmed.ncbi.nlm.nih.gov/17007444/17007444 · pubmed ↗
- 4Consistency of pituitary adenoma: prediction by pharmacokinetic dynamic contrast-enhanced MRI and comparison with histologic collagen content Cancers (Basel) Kamimura K Nakajo M Bohara M 39141320213435981410.3390/cancers 13153914 PMC 8345382 · doi ↗ · pubmed ↗
- 5National Cancer Data Base report on malignant paragangliomas of the head and neck Cancer Lee JH Barich F Karnell LH Robinson RA Zhen WK Gantz BJ Hoffman HT 7307379420021185730610.1002/cncr.10252 · doi ↗ · pubmed ↗
- 6Usefulness of 123I-MIBG scintigraphy in the evaluation of patients with known or suspected primary or metastatic pheochromocytoma or paraganglioma: results from a prospective multicenter trial J Nucl Med Wiseman GA Pacak K O'Dorisio MS 144814545020091969002810.2967/jnumed.108.058701 PMC 4722807 · doi ↗ · pubmed ↗
- 7A case of nonchromaffin paraganglioma originating in the suprasellar region and invading the nose through the sphenoid sinus [Article in Czech]Cesk Otolaryngol Chytil S 115119161967 https://pubmed.ncbi.nlm.nih.gov/4292615/4292615 · pubmed ↗
- 8Intrasellar paraganglioma associated with hypopituitarism Arch Pathol Lab Med Bilbao JM Horvath E Kovacs K Singer W Hudson AR 95981021978 https://pubmed.ncbi.nlm.nih.gov/341846/341846 · pubmed ↗