Treatment of hip instability after total hip replacement with pelvic osteotomy using a modified Stoppa approach
Deniz Akbulut, Mehmet Coşkun, Yakup Alpay, Javad Mirzazada

TL;DR
This paper presents a case study of a patient with recurrent hip dislocation after total hip replacement, successfully treated with pelvic osteotomy using a modified Stoppa approach without component revision.
Contribution
The novel use of pelvic osteotomy via a modified Stoppa approach to treat hip instability without revising implant components is highlighted.
Findings
Pelvic osteotomy successfully reduced acetabular inclination in a patient with recurrent hip dislocation.
The patient showed significant clinical improvement with no dislocation recurrence at two years.
Component revision was avoided, preserving bone stock and avoiding complications from cup extraction.
Abstract
Hip dislocation remains a significant complication following total hip arthroplasty, even though its incidence has decreased. While closed reduction is typically performed for early dislocations, delayed or chronic dislocations often necessitate acetabular or femoral component revision. This document describes the treatment of hip dislocation in a 56-year-old patient through pelvic osteotomy without component revision. An acetabular component malposition was identified, exhibiting an 80-degree inclination and 20-degree cup anteversion. Owing to limited bone stock, a modified Stoppa approach was used for pelvic osteotomy to reduce acetabular inclination. The patient displayed remarkable clinical improvement, achieving a Harris Hip Score of 85 at the two-year check-up with no signs of dislocation. Recurrent hip dislocation is difficult to manage. It frequently necessitates component…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2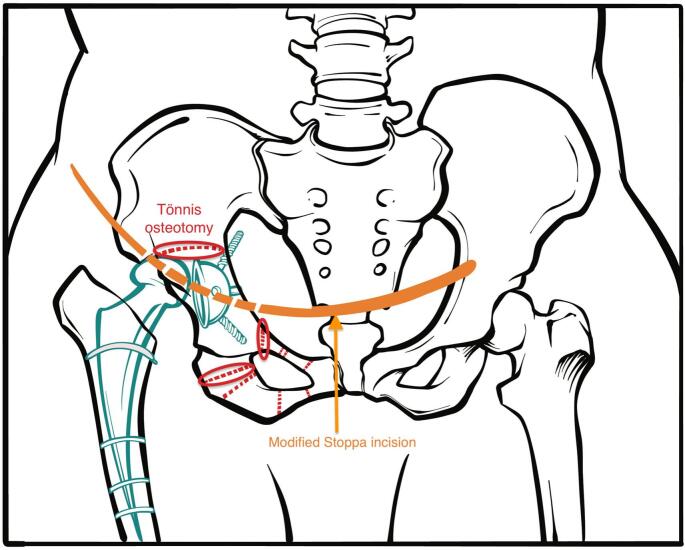 Figure 3
Figure 3 Figure 4
Figure 4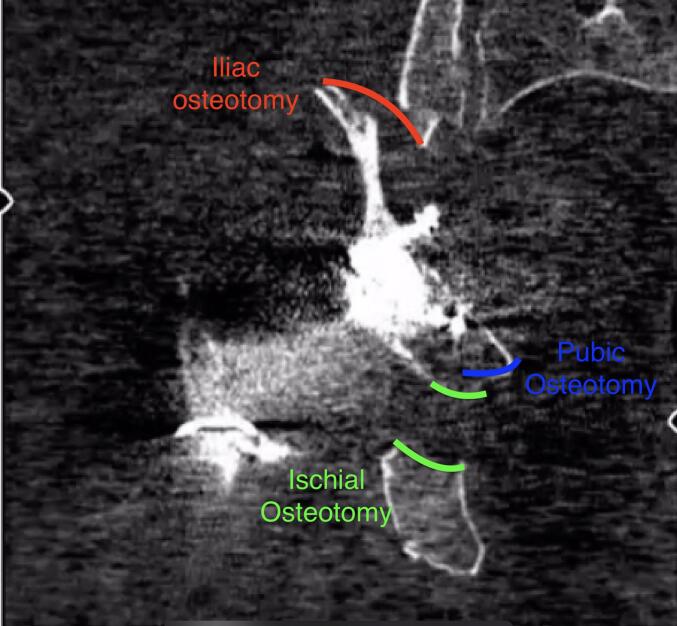 Figure 5
Figure 5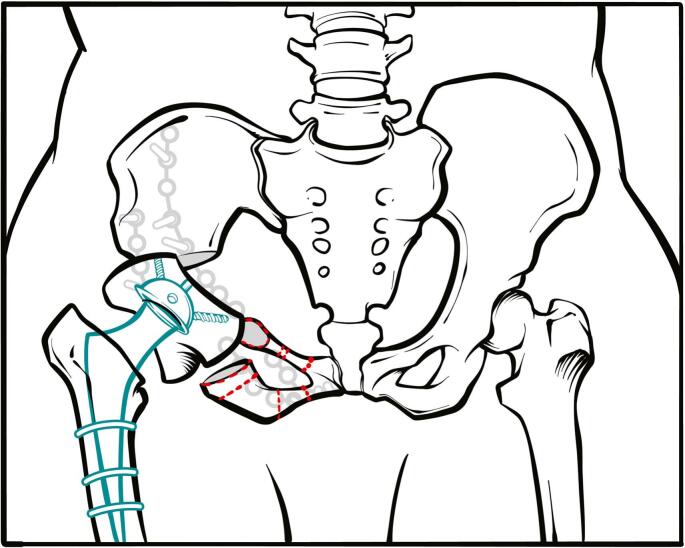 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes · Hip disorders and treatments
Introduction and background
1
Total hip arthroplasty (THA) is the most commonly used treatment for coxarthrosis in adults [1]. Various guidelines have been proposed to minimize complications related to THA, such as hip dislocation, inaccurate placement of components, discrepancies in limb length, deep vein thrombosis (DVT), and infections [2]. However, despite numerous technological advancements, hip dislocation remains a critical aftermath of THA [3]. Several suggestions have been offered in previous studies to mitigate the dislocation risk, including the use of a giant femoral head or an elevated liner [4]. Treatment for hip dislocation can involve closed reduction. If misplaced components are found to be the cause, options include revision of the acetabular/femoral component or a complete overhaul [5]. The most complex part of the surgical procedure involves the removal of the acetabular cup or femoral stem during component revision. This presents a major surgical challenge, requiring management of the ensuing bony defect post-cup extraction and treatment for any instability [[6], [7], [8]]. In this case study, we outline our approach to treating recurrent hip dislocation caused by component malposition. This involved a triple pelvic osteotomy using the modified Stoppa technique without needing to extract the cup.
Case presentation
2
Our subject is a 56-year-old female patient who had hip surgery a year prior. Her first dislocation occurred two months after the surgery. She has since had to undergo closed reduction three times due to further dislocations. She came to us after experiencing a fourth dislocation a month before her visit (Fig. 1). An assessment of her hip X-ray images showed a malpositioned acetabular component, with an inclination of 80 degrees and a cup anteversion of 20 degrees, along with a posterior hip dislocation. To treat this, we performed a pelvic osteotomy using a modified Stoppa approach to correct the acetabular inclination (Fig. 2). After two years, she showed no signs of dislocation. At the most recent follow-up, her Harris Hip Score was 85. The patient and her family were informed that her case data would be published, to which they gave their consent.Fig. 1. Excessively vertical inclination and neutral anteversion of the acetabular cup caused multiple dislocations.Fig. 1. Fig. 2Joint stability was attained following periacetabular osteotomy by restoring acetabular cup inclination and anteversion.Fig. 2
Surgical procedure
3
First, an incision was made over the symphysis pubis, cutting through the skin and underlying tissue (Fig. 3). The rectus abdominis muscle was then longitudinally divided, and the distal L-shaped portion was detached from the symphysis pubis. This revealed the pubic arches and quadrilateral surface. Following this, the corona mortis was tied off, and the obturator neurovascular bundle, which crossed the quadrilateral surface, was left untouched. Next, an ischial osteotomy was performed on the pubic arch, followed by an iliac osteotomy using Schanz screws in the iliac wing. Subsequently, the osteotomized acetabulum was flipped over, and its inclination was reduced (Fig. 4, Fig. 5). The successful concentric reduction of the hip was confirmed using fluoroscopic imaging. As the patient displayed signs of osteoporosis, fixative measures included using a reconstruction plate, which started from the iliac wing and extended to the opposite side of the symphysis pubis. For added stability, a second plate was used to reinforce the joined area between the iliac bone and the acetabulum (Fig. 6). The work has been reported in line with the SCARE criteria [9].Fig. 3. The illustration demonstrates the intended approach where the dotted lines show the osteotomy options. We preferred Tönnis osteotomy which is marked with red ring.Fig. 3. Fig. 4Iliac osteotomy marked in the sagittal CT section.Fig. 4. Fig. 5Iliac, pubic and ischial osteotomies marked in the frontal CT section.Fig. 5. Fig. 6The illustration demonstrates the completed and fixated osteotomy with the attained joint stability.Fig. 6
Clinical discussion
4
Hip dislocation is a notable complication post-THA. It could be addressed through closed reduction or by revising acetabular or femoral components. The treatment of recurrent hip dislocation is challenging as it often necessitates component revision, complicated by difficulties extracting the cup and insufficient bone stock [10]. Utmost importance is to be emphasized on the mechanism of the dislocation for a proper management because the dislocation tends to recur [11] as it did in our case.
THA revision is frequently required due to hip instability, aseptic loosening, or infection. Unidentified preoperative component loosening may lead to bone stock loss during cup extraction, which can potentially result in pelvic insufficiency. The Paprosky classification helps in determining treatment options based on bone stock levels [12]. However, our patient could not be classified using this system due to excellent cup osteointegration and the inability to estimate remaining bone stock after cup removal [13].
Despite all the efforts to develop the biomechanical factors and design, THA revision rate continues to grow along with the primary THA and prospects demonstrate accordingly [14]. The most contemporary techniques demand the acetabular revision as a part of the procedure to restore the biomechanical integrity of the design [15]. In fact, in some cases there is such a sturdy osteointegration that it's almost impossible to extract the component without harming the periacetabular bone. Our technique emerges as an alternative in patients with either ample or scarce bone stock where the acetabular revision is deemed unnecessary.
This technique also carries a financial benefit as it perishes the necessity for new set of THA equipment. Meanwhile lesser the use of the metal, lesser the risk of periprosthetic infections which is one of the most devastating complications in this area.
Alongside the advantages there is still a need for a superior skill in pelvic, particularly in acetabular surgery to perform this technique. Nevertheless, we believe an arthroplasty surgeon with skills to handle pelvis would easily overcome the challenge in short learning curve.
We diagnosed our patient with insufficient medial and superior walls and evaluated the need for ring and cage reconstruction post-cup extraction. However, there's no universally accepted treatment for pelvic discontinuity and extensive bone loss and further investigation on the long-term outcomes of these pelvic reconstructions is needed to judge their surgical effectiveness.
In this case, given the excellent cup osteointegration, we conducted a triple pelvic osteotomy. This procedure reduced the cup inclination from 80 to 45 degrees. An anteversion of 10 degrees was detected, which increased to 15 degrees following posterior hip dislocation.
Conclusion
5
Pelvic osteotomy effectively restores normal biomechanics in patients with component misalignment without causing loosening.
Informed consent
A detailed informed consent is presented and signed by the family prior to this presented study.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethics clearance was not necessary in our institution.
Funding
Non to declare.
Author contribution
Mehmet Coskun and Deniz Akbulut elaborated study concept/design, Yakup Alpay collected, analyzed, and interpreted the data, and Javad Mirzazada accomplished writing the paper.
Guarantor
Mehmet Coskun is the author who accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Research registration number
-
Name of the registry: clinicaltrials.gov.
-
Unique identifying number or registration ID: NCT06209255.
-
Hyperlink to your specific registration (must be publicly accessible and will be checked): https://register.clinicaltrials.gov/prs/app/action/SelectProtocol?sid=S000DXUB&selectaction=Edit&uid=U00079FU&ts=2&cx=-8e1324.
Conflict of interest statement
Non to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kocabiyik A.Changes in hip, knee, and ankle coronal alignments after total hip arthroplasty with transverse femoral shortening osteotomy for unilateral Crowe type IV developmental dysplasia of the hip J. Arthroplasty 3211 Nov. 20173449345610.1016/j.arth.2017.05.04428641973 · doi ↗ · pubmed ↗
- 2Guo L.Risk factors for dislocation after revision total hip arthroplasty: a systematic review and meta-analysis Int. J. Surg.38Feb. 201712312910.1016/j.ijsu.2016.12.12228043927 · doi ↗ · pubmed ↗
- 3Yetkin C.Yildirim T.Alpay Y.Tas S.K.Buyukkuscu M.O.Dırvar F.Evaluation of dislocation risk factors with total hip arthroplasty in developmental hip dysplasia patients: a multivariate analysis J. Arthroplasty 362Feb. 202163664010.1016/j.arth.2020.08.04332943316 · doi ↗ · pubmed ↗
- 4Alberton G.M.High W.A.Morrey B.F.Dislocation after revision total hip arthroplasty: an analysis of risk factors and treatment options J. Bone Joint Surg. Am.8410 Oct. 20021788179212377909 · pubmed ↗
- 5Sadhu A.Nam D.Coobs B.R.Barrack T.N.Nunley R.M.Barrack R.L.Acetabular component position and the risk of dislocation following primary and revision total hip arthroplasty: a matched cohort analysis J. Arthroplasty 323Mar. 201798799110.1016/j.arth.2016.08.00827633947 · doi ↗ · pubmed ↗
- 6Ballester Alfaro J.J.Sueiro Fernández J.Trabecular metal buttress augment and the trabecular metal cup-cage construct in revision hip arthroplasty for severe acetabular bone loss and pelvic discontinuity Hip Int.20Suppl. 72010 S 119S 12710.1177/11207000100200 s 72020512783 · doi ↗ · pubmed ↗
- 7Dennis D.A.Management of massive acetabular defects in revision total hip arthroplasty J. Arthroplasty 183 Suppl 1Apr. 200312112510.1054/arth.2003.5010512730946 · doi ↗ · pubmed ↗
- 8De Boer D.K.Christie M.J.Brinson M.F.Morrison J.C.Revision total hip arthroplasty for pelvic discontinuity J. Bone Joint Surg. Am.894Apr. 200783584010.2106/JBJS.F.0031317403808 · doi ↗ · pubmed ↗