Clinical and nutritional correlates of bacterial diarrhoea aetiology in young children: a secondary cross-sectional analysis of the ABCD trial
Sarah Somji, Per Ashorn, Karim Manji, Tahmeed Ahmed, Md Chisti, Usha Dhingra, Sunil Sazawal, Benson Singa, Judd L Walson, Patricia Pavlinac, Naor Bar-Zeev, Eric Houpt, Queen Dube, Karen Kotloff, Samba Sow, Mohammad Tahir Yousafzai, Farah Qamar, Rajiv Bahl, Ayesha De Costa

TL;DR
This study found that certain nutritional and clinical factors are linked to bacterial causes of severe diarrhea in young children, which could help identify those needing antibiotics.
Contribution
The study identifies specific clinical and nutritional correlates associated with bacterial diarrhea in young children.
Findings
Children with moderate acute malnutrition had higher odds of bacterial diarrhea.
Dehydration and high stool frequency were also linked to bacterial causes.
Fever and prolonged diarrhea were not associated with bacterial aetiology.
Abstract
The objective was to assess the association between nutritional and clinical characteristics and quantitative PCR (qPCR)-diagnosis of bacterial diarrhoea in a multicentre cohort of children under 2 years of age with moderate to severe diarrhoea (MSD). A secondary cross-sectional analysis of baseline data collected from the AntiBiotics for Children with Diarrhoea trial (NCT03130114). Children with MSD (defined as >3 loose stools within 24 hours and presenting with at least one of the following: some/severe dehydration, moderate acute malnutrition (MAM) or severe stunting) enrolled in the ABCD trial and collected stool sample. June 2017–July 2019. None. Likely bacterial aetiology of diarrhoea. Secondary outcomes included specific diarrhoea aetiology. A total of 6692 children with MSD had qPCR results available and 28% had likely bacterial diarrhoea aetiology. Compared with children…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
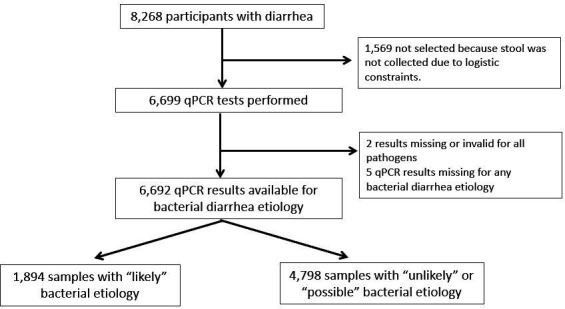 Figure 1
Figure 1| Baseline characteristics | Bangladesh | India | Pakistan | Kenya | Malawi | Mali | Tanzania | All sites |
| Age (months) | 11.2 (5.0)* | 11.9 (5.6)* | 12.5 (5.5)* | 11.0 (5.7)* | 12.0 (4.8)* | 12.0 (4.6)* | 11.0 (5.2)* | 11.6 (5.3)* |
| Males | 57.8% | 52.9% | 50.6% | 52.7% | 56.9% | 53.9% | 53.2% | 53.8% |
| Any rotavirus vaccination | 1.0% | 2.7% | 7.3% | 99.6% | 99.6% | 97.6% | 99.9% | 60% |
| Exclusively breastfed at time of enrolment | 1.7% | 6.9% | 9.2% | 17.9% | 4.1% | 5.4% | 14.4% | 8.7% |
| Maternal age, years | 24 (5) | 26 (4) | 27 (6) | 26 (6) | 25 (6) | 26 (6) | 27 (6) | 26 (6) |
| Maternal body mass index, kg/m2 | 22.3 (4.3) | 22.6 (4.3) | 23.2 (5.0) | 23.2 (3.8) | 23.1 (5.3) | 24.0 (4.9) | 24.5 (5.0) | 23.3 (4.7) |
| Maternal education, completed school years | 5.8 (4.0) | 4.8 (4.8) | 2.9 (4.0) | 9.0 (2.9) | 8.3 (2.8) | 4.3 (5.0) | 7.8 (2.7) | 6.0 (4.4) |
| Number of children <5 years of age in house | 1.2 (0.4) | 1.9 (0.9) | 2.0 (1.0) | 1.7 (0.8) | 1.4 (0.6) | 2.4 (1.8) | 1.3 (0.5) | 1.7 (1.1#) |
| Fever (defined as temperature >37.5°C) | 15.3% | 7.6% | 9.0% | 6.0% | 19.4% | 16.9% | 12.5% | 12.1% |
| Some/severe dehydration | 25.1% | 48.4% | 28.5% | 91.8% | 77.7% | 23.1% | 92.8% | 54.4% |
| Length for age z-score (LAZ) | −1.83 (1.15) | −2.12 (1.28) | −2.15 (1.28) | −0.81 (1.26) | −1.55 (1.47) | −1.16 (1.13) | −0.76 (1.14) | −1.48 (1.36) |
| Weight for length z-score (WLZ) | −1.69 (0.90) | −1.37 (1.01) | −1.45 (0.96) | −0.28 (1.19) | −0.62 (1.19) | −2.04 (0.74) | −0.39 (1.27) | −1.14 (1.23) |
| Severe stunting† | 19.5% | 27.6% | 27.5% | 5.6% | 16.5% | 6.5% | 2.2% | 15.0% |
| Moderate acute malnutrition‡ | 73.6% | 57.3% | 70.6% | 14.0% | 26.0% | 85.0% | 16.1% | 49.9% |
| Presence§ of any bacterial pathogen¶ in stool | 36.3% | 27.5% | 30.9% | 21.5% | 31.7% | 28.6% | 22.9% | 28.3% |
| Presence¶ of Shigella in stool | 12.8% | 16.0% | 18.2% | 7.0% | 11.3% | 13.5% | 9.2% | 12.6% |
| Presence¶ of ST-ETEC** in stool | 19.4% | 9.9% | 12.7% | 10.4% | 20.4% | 11.9% | 10.7% | 13.3% |
| Bacterial aetiology | |||
| Proportion n/N (%) | Adjusted* OR (95% CI) | P value | |
| Moderate to severe diarrhoea defining characteristics | |||
| 94/417 (22.5) | Ref. | – | |
| 764/2832 (27.0) | 1.67 (1.26 to 2.24) | <0.001 | |
| 675/2228 (30.3) | 1.57 (1.19 to 2.09) | 0.002 | |
| 209/626 (33.4) | 2.23 (1.62 to 3.08) | <0.001 | |
| 109/408 (26.7) | 1.13 (0.79 to 1.62) | 0.52 | |
| 22/95 (23.2) | 1.42 (0.79 to 2.49) | 0.23 | |
| 20/84 (23.8) | 0.80 (0.39 to 1.53) | 0.52 | |
| Fever | |||
| 1646/5884 (28.0) | Ref. | – | |
| 248/808 (30.7) | 1.11 (0.93 to 1.32) | 0.26 | |
| Duration of diarrhoea (excluding day of enrolment) | |||
| 1781/6328 (28.1) | Ref. | – | |
| 113/364 (31.0) | 1.22 (0.94 to 1.58) | 0.13 | |
| Frequency of diarrhoea in the past 24 hours | |||
| 912/3536 (25.8) | Ref. | – | |
| 982/3156 (31.1) | 1.20 (1.05 to 1.36) | 0.007 | |
| Proportion n/N (%) | Adjusted* OR (95% CI) | P value | Proportion n/N (%) | Adjusted* OR (95% CI) | P value | |
| Moderate to severe diarrhoea defining characteristics | ||||||
| 40/417 (9.6) | Ref. | – | 52/417 (12.5) | Ref. | – | |
| 378/2815 (13.4) | 1.74 (1.19, 2.62) | 0.006 | 305/2832 (10.8) | 1.18 (0.82 to 1.73) | 0.38 | |
| 319/2227 (14.3) | 1.69 (1.15 o to 2.53) | 0.009 | 320/2224 (14.4) | 1.29 (0.90 to 1.86) | 0.17 | |
| 81/623 (13.0) | 1.83 (1.18 to 2.89) | 0.008 | 90/626 (14.4) | 1.64 (1.09 to 2.50) | 0.02 | |
| 45/408 (11.0) | 1.04 (0.62 to 1.74) | 0.87 | 63/408 (15.4) | 1.08 (0.69 to 1.70) | 0.75 | |
| 14/95 (14.7) | 1.92 (0.92 to 3.82) | 0.07 | 5/95 (5.3) | 0.52 (0.17 to 1.27) | 0.19 | |
| 12/84 (14.3) | 1.19 (0.46 to 2.71) | 0.69 | 10/84 (11.9) | 0.68 (0.25, 1.58) | 0.41 | |
| Fever | ||||||
| 767/5865 (13.1) | Ref | – | 736/5883 (12.5) | Ref | – | |
| 122/806 (15.1) | 1.12 (0.89 to 1.40) | 0.31 | 109/808 (13.5) | 1.15 (0.90 to 1.46) | 0.26 | |
| Duration of diarrhoea (excluding day of enrolment) | ||||||
| 846/6308 (13.4) | Ref | – | 783/6327 (12.4) | Ref | – | |
| 43/363 (11.8) | 1.05 (0.72 to 1.50) | 0.79 | 62/364 (17.0) | 1.29 (0.92 to 1.78) | 0.13 | |
| Frequency of diarrhoea in the past 24 hours | ||||||
| 433/3521 (12.3) | Ref | – | 406/3535 (11.5) | Ref | – | |
| 456/3150 (14.5) | 1.10 (0.93 to 1.31) | 0.28 | 439/3156 (13.9) | 1.17 (0.98 to 1.40) | 0.08 | |
- —http://dx.doi.org/10.13039/100000865Bill and Melinda Gates Foundation
- —http://dx.doi.org/10.13039/100000002National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral gastroenteritis research and epidemiology · Child Nutrition and Water Access · Clinical Nutrition and Gastroenterology
Introduction
Diarrhoea causes over 400 000 deaths annually and strategies to reduce this burden are informed by studies of diarrhoea aetiology.1 Bacterial pathogens including enterotoxigenic Escherichia coli (ETEC) encoding heat stable toxin (ST-ETEC) and Shigella are commonly associated with childhood diarrhoea.2 3 The WHO recommends antibiotics for diarrhoea only if there is blood in stool or in suspected cases of cholera.4 Increasing evidence, however, suggests that acute watery diarrhoea can have bacterial (Shigella or enteroinvasive E. coli, EIEC) aetiology as seen in an age-stratified case–control Global Enteric Multicentre Study (GEMS). This study enrolled cases who had moderate to severe diarrhoea (MSD) in children under 5 and noted in their collected stool samples that 40.3% Shigella spp or EIEC diarrhoea attributed cases were non-dysenteric.3 Whether children with diarrhoea of bacterial aetiology can be identified, may have implications for antibiotic treatment recommendations.
While the relationship between nutritional status and incidence of diarrhoeal disease is well established, few studies have examined the relationship between child anthropometric and clinical characteristics with the specific aetiology of diarrhoea. Among Bangladeshi children aged 2–5 years with diarrhoea, those with malnutrition (defined as weight-for-age Z-score (WAZ)< −2) were more likely to present with specific parasitic and bacterial enteropathogens specifically ETEC.5 Another study in Kenya noted that malnourished children were more likely to have MSD due to enteroaggregative E. coli (EAEC) but in another study in Bangladesh in a similar cohort, similar children were likely to present with Shigella.6 7 While these studies suggest that acute malnutrition may be an important risk factor for bacterial causes of diarrhoea, they are notable for being performed at single sites, among children with either low-risk diarrhoea or in hospitalised children, or collected with traditional bacterial culture methods, and/or for a limited number of pathogens. We recently completed a large, multicentre clinical trial of antibiotics for MSD in children ages 2–23 months.8 9 This cohort provided an opportunity to better understand whether nutritional status and other clinical characteristics were associated with specific pathogens causing diarrhoea across several countries. Participants in the trial presented with MSD and were assessed using molecular detection tools for several types of enteropathogens. We hypothesised that among children with MSD, those with moderate acute malnutrition (MAM) would be more likely to have a bacterial aetiology.
Methods
Participants
We studied a subsample of participants from the ABCD trial, a randomised, blinded, placebo-controlled, multicountry trial designed to evaluate whether azithromycin would reduce all-cause mortality in young children with undernutrition and MSD.8 9 The trial was implemented in Bangladesh, India, Kenya, Malawi, Mali, Pakistan and Tanzania between June 2017 and July 2019 in MSD children 2–23 months of age. For the purpose of this study, MSD was defined as a history of acute watery diarrhoea (caretaker report of >3 loose/watery stool in the past 24 hours) for <14 days with one of more of the following: the presence of some/severe dehydration per WHO standards10 MAM (defined as weight-for-length z-score <−2 and >−3 (or mid-upper arm circumference (MUAC) >115 mm and <125 mm for children over 6 months)); or severe stunting (length-for-age z-score <−3). Exclusion criteria included receipt of antibiotics currently/in previous 14 days; allergy/contraindication to azithromycin; had dysentery; severe acute malnutrition or clinical suspicion of Vibrio cholerae infection; previous/current enrolment of the child in this/any interventional trial; enrolment of a sibling or another child in the same household; or living at a distance from the enrolment centre that would prevent direct observation on days 2 and 3. After written informed consent was obtained, participants were randomised to receive either a 3-day course of azithromycin or placebo.9 The subsample was participants identified randomly, at baseline with equal numbers from all sites.
Exposure and confounding variables
MSD defining characteristics were the primary exposure of interest and included severe stunting, MAM, some/severe dehydration or a combination of either of the two or all three characteristics. All anthropometric measurements were performed by two independent trained assessors according to WHO guidelines.8 Weight was measured using an electronic scale to the closest±10 g, length was obtained using a length board to the nearest 0.1 cm and MUAC was obtained using a non-stretchable tape to the nearest 0.1 cm. Study physicians measured the temperature using a digital thermometer at screening. Fever was calculated as temperature >37.5°C. Diarrhoea duration and diarrhoea frequency in the past 24 hours was recorded from mothers recall. Numerous confounding variables were collected at baseline using standardised questionnaires across all sites (online supplemental figure 1). A wealth quintile variable was created using country-specific wealth distribution as reported in each country’s most recent Demographic and Health Survey.11
10.1136/bmjpo-2023-002448.supp1Supplementary data
Outcome variables
The primary outcome variable was likely bacterial diarrhoea aetiology assessed by quantitative PCR PCR (qPCR) on a baseline stool sample. Secondary outcomes included specific bacterial diarrhoea aetiology (likely ST-ETEC or Shigella). Stool or rectal swab samples were tested by qPCR with a customised 85-target TaqMan array card to determine a cycle threshold value and is detailed elsewhere.3 Pathogen-specific cut-offs were developed to assign likely diarrhoea aetiology based on the quantity of pathogen DNA/RNA in the stool sample (ie, pathogen burden). These cut-offs12 were obtained using adapted statistical models from two previously performed large multisite diarrhoea studies: the seven-site GEMS and the eight-site Malnutrition and the Consequences for Child Health and Development cohort study.3 13 Each cut-off was calculated by taking the median quantity-specific OR from site-specific models from previous studies. Then, the episode-specific attributable fraction (AFe) was calculated. Finally, an LOESS regression was fit and the highest Ct value with >0.5 Afe value was picked as the cut-off for each pathogen.14 15
For this analysis, Ct values lower than these cut-offs were considered as ‘likely’ bacterial diarrhoea associated aetiology. Specimens assessed as ‘likely’ were compared with the other category. Ascribing aetiology to ‘likely’ with these cut-offs has been previously performed.16 Bacteria assessed for aetiology and their Ct cut-off values included Campylobacter (16.3), typical Enteropathogenic Escherichia coli (EPEC) (18.1), ST-ETEC (25.4), Salmonella (31.9), Shigella (28.7) and V. cholerae (32.6). Shigella and ST-ETEC were chosen as the main specific aetiologies since they comprised about 84% of all bacterial enteropathogens. Due to logistical and budgetary constraints, stool/rectal swabs from approximately the first 1000 participants at each site were collected. Whole stool sample or flocked rectal swab were stored at −80°C until analysis.
Statistical analysis
We conducted a cross-sectional analysis of baseline data from the ABCD trial. Logistic regressions were used to examine the association of clinical and anthropometric characteristics, including MSD defining characteristics: fever, diarrhoea duration and stool frequency, with likely bacterial diarrhoea aetiology. For the variable MSD defining characteristic, the presence of severe stunting alone was used as the reference category since participants with severe stunting had the lowest prevalence of likely bacterial diarrhoea. Some previous studies also suggest that stunting is not associated with presence of specific pathogens in stools of children with diarrhoea.7 17
Diarrhoea duration at enrolment was categorised as 0–6 days of diarrhoea versus prolonged diarrhoea of 7–14 days, and diarrhoea frequency in the past 24 hours was categorised as low frequency (3–6 stools) versus high frequency (>6 stools). Bivariate (unadjusted) and multivariable analyses were conducted. Multivariable models included covariates for potential confounding factors that may be associated with both child nutritional status and diarrhoea aetiology based on a literature review. All statistical analyses were performed by using R V.4.0.2 Software (R Foundation for Statistical Computing).
Results
The parent ABCD trial enrolled 8268 participants who presented with MSD. In total, 6699 had stool/rectal samples collected at baseline and qPCR testing done. Of those, two had missing/invalid qPCR results and five had no bacterial diarrhoea aetiology. On recalculation of anthropometric indexes, seven participants were deemed to have been erroneously enrolled, as they did not meet all enrolment criteria. The deviations from anthropometric enrolment cut-offs were, however, minor and these seven children were retained in the sample. Therefore, 6692 participants across the study sites were included in this analysis (figure 1) and 28% overall had diarrhoea of likely bacterial aetiology (table 1).
Flow chart of children aged 2–23 months presenting with moderate to severe diarrhoea. ‘Likely’ diarrhoea associated aetiology was determined by Ct value cut-offs for specific enteropathogens. Ct values greater than these cut-offs but <35 were considered ‘possible’ aetiologies while Ct value >35 was considered ‘unlikely’ aetiology. qPCR, quantitative PCR.
We first examined the association of MSD-defining characteristics with likely bacterial aetiology. Compared with children with severe stunting and adjusting for multiple clinical and demographic factors, children presenting with some/severe dehydration only (adjusted OR (aOR) 1.67 (95% CI (1.26 to 2.24)), MAM (aOR 1.57 (95% CI 1.19 to 2.09)), and both MAM and dehydration (aOR 2.23 (95% CI 1.62 to 3.08)) were significantly at higher odds of a likely bacterial infection (table 2). A similar trend was noted for ST-ETEC aetiology where children presenting with dehydration (aOR 1.74 (95% CI 1.19 to 2.62)), MAM (aOR 1.69 (95% CI 1.15 to 2.53)), and MAM and dehydration (aOR 1.83 (95% CI 1.19 to 2.89)) compared with those severely stunted, were at higher odds of a likely ST-ETEC aetiology (table 3). For Shigella, only children presenting with MAM and dehydration were found to have higher odds (aOR 1.64 (95% CI 1.09 to 2.50)) compared with those severely stunted (table 3). In bivariate associations of likely bacterial aetiology, MAM and dehydration increased odd of likely bacterial aetiology (OR 1.70 (95% CI 1.28 to 2.27)) and MAM increased the odds of likely ST-ETEC aetiology (OR 1.58 (95% CI 1.13 to 2.26)) versus severe stunting (online supplemental table 1).
10.1136/bmjpo-2023-002448.supp2Supplementary data
Fever and duration of diarrhoea were not associated with bacterial aetiology or Shigella or ST-ETEC aetiology ([tables 2 and 3](#T2 T3)). However, children with high stool frequency (>6 stools) had increased odds of likely bacterial aetiology (aOR 1.20 (95% CI 1.05 to 1.36)) compared with those with lower stool frequency.
Since the qPCR analysis often detected more than one type of enteropathogen, we performed sensitivity analyses to evaluate the association between clinical and anthropometric characteristics with likely bacterial diarrhoea aetiology in children where only the enteropathogen of interest was found. The proportion of children who had only a single likely diarrhoea bacterial aetiology was 1110/6648 (16.7%). No statistically significant associations were observed between anthropometrics and specific likely bacterial pathogens in these sensitivity analyses. High stool frequency, however, was associated with higher odds of likely bacterial diarrhoea aetiology (aOR 1.23 (95% CI 1.05 to 1.45)), and Shigella aetiology (aOR 1.32 (95% CI 1.04 to 1.68)) after adjusting for multiple factors (online supplemental tables 2 and 3).
10.1136/bmjpo-2023-002448.supp3Supplementary data
10.1136/bmjpo-2023-002448.supp4Supplementary data
Discussion
In this analysis of 6692 children with MSD whose aetiology was assessed by qPCR methods, we found that several anthropometric and clinical factors were associated with likely bacterial diarrhoea aetiology. Children presenting with either MAM, dehydration or a combination of both, had higher odds of a likely bacterial and ST-ETEC diarrhoea aetiology compared with severely stunted children. Children with MAM and dehydration were also more likely to have Shigella diarrhoea aetiology compared with severely stunted children. Children with high stool frequency had higher odds of likely bacterial diarrhoea aetiology, a finding confirmed on sensitivity analysis evaluating children with only a single pathogen identified.
Our findings of association between MAM and a likely bacterial and ST-ETEC diarrhoea aetiology are consistent with some earlier studies.7 18 Tickell et al studied 1363 Kenyan children aged 6–59 months who presented with acute diarrhoea. The study noted that children with acute diarrhoea and wasting (defined as MUAC<12.5 cm) were 1.8 times more likely to have EAEC diarrhoea aetiology compared with those not wasted. Although the definition of acute malnutrition was different from our definition, they used similar PCR-based automated bacterial pathogen detection methods. A case–control study among children aged 6–23 months in Bangladesh18 noted that bacterial enteropathogens such as Shigella and EAEC were more common among children who were underweight (defined as WAZ<−2), a finding similar to ours. This study, however, enrolled children with malnutrition and only ~5% of those enrolled had diarrhoea at baseline, whereas in our study all children had MSD. Similarly, a recent cross-sectional study carried out in Ethiopia noted that being wasted was associated with Salmonella infection.19
Children with some/severe dehydration, with/without MAM, had greater odds of likely bacterial or ST-ETEC diarrhoea aetiology compared with children with severe stunting. Some/severe dehydration is known to be a risk factor for severe diarrhoea (and even death) in children but not usually associated with bacterial diarrhoea.20 21 In a study carried out in chidren <5 years presenting to a health clinic in Rwanda, Shigella was not associated with severe dehydration.22 Moreover, in a retrospective study carried out in Lao PDR to evaluate clinical and aetiology associated with severity of acute diarrhoea, among hospitalised children, 48.4% presented with dehydration and prevalence of dehydration was higher in those with rotavirus aetiology versus rotavirus negative children. This association of dehydration was not noted in children with Shigella or Salmonella aetiology, although the low numbers of samples positive for Salmonella (n=4) and Shigella (n=1) vs rotavirus (n=10) is noteworthy.23 Neither of the studies noted the association of dehydration in any bacterial diarrhoea in contrast with our findings.
A reanalysis of the ABCD trial including molecular diagnostics was conducted to understand the effect of azithromycin in the outcomes in children with and without bacterial diarrhoea aetiology.16 It was noted that among those with likely and possible bacterial aetiology, those in the azithromycin arm had lower risk of diarrhoea at 3 days after randomisation in comparison to those in the placebo arm. Additionally, within the 90-day follow-up period, azithromycin use was associated with lower risk of deaths/hospitalisations in children with likely and possible bacterial diarrhoea. As noted in Pavlinac et al’s results 12 and previous studies, bacterial diarrhoea may not always present with clinical signs and symptoms of dysentery13 24 and, therefore, limiting antibiotics to those with clinically apparent dysentery may limit treatment of bacterial diarrhoea. The findings from our analysis outlines clinical and nutritional risk factors to potentially identify such high+risk children who may benefit from antibiotics before culture results are known.
Our secondary analysis has some limitations. First, the observational, cross-sectional nature of the analysis limits the ability to make causal inferences. Second, we may not have had adequate power to detect more moderate magnitudes of association between nutritional status and diarrhoea aetiology. Third, our study included children with MSD which may limit the generalisability of our findings. We note that lack of a non-malnourished group (or severely malnourished group such as SAM) adds to the limited of generalisability. Finally, the use of enteropathogens cut-offs is complicated in settings where asymptomatic carriage of enteropathogens is high. It is noteworthy that these cut-offs were derived from previous case–control studies, thus may be subject to further refinement. It is also noted that there were a small number of children with individual pathogens which limited the power to detect differences between groups. Strengths of the study include the multicountry setting, the prospective nature of the data collection, the inclusion of numerous possible confounding variables, standardised measures of anthropometric data and the use of novel enteropathogen detection tools. We also note that additional covariates that could influence the associations such as preterm birth, bloody diarrhoea, severe wasting were not included since some were not measured and others were exclusion criteria.
In summary, in this large cohort of children with MSD, we note that MAM and dehydration as well as high frequency of stools were associated with an increased odd of likely bacterial aetiology, compared with those with severe stunting. These findings suggest that these characteristics could be helpful criteria for children presenting with MSD who might benefit from antibiotics during an acute diarrhoeal episode. Future studies could examine other, more specific risk factors for diarrhoea aetiology, including micronutrient status,25 26 exposure to food and water sources,27–29 vaccine status30 and others. Additional trials of the utility of targeted antibiotic therapy also seem warranted.
Supplementary Material
Reviewer comments
Author's manuscript
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Troeger C, Blacker BF, Khalil IA, et al. Estimates of the global, regional, and national morbidity, mortality, and Aetiologies of diarrhoea in 195 countries: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis 2018;18:1211–28. 10.1016/S 1473-3099(18)30362-130243583 PMC 6202444 · doi ↗ · pubmed ↗
- 2Nuzhat S, Shahunja KM, Shahid ASMSB, et al. Diarrhoeal children with concurrent severe wasting and Stunting compared to severe wasting or severe Stunting. Trop Med Int Health 2020;25:928–35. 10.1111/tmi.1344632446268 · doi ↗ · pubmed ↗
- 3Liu J, Platts-Mills JA, Juma J, et al. Use of quantitative molecular diagnostic methods to identify causes of diarrhoea in children: a Reanalysis of the GEMS case-control study. The Lancet 2016;388:1291–301. 10.1016/S 0140-6736(16)31529-XPMC 547184527673470 · doi ↗ · pubmed ↗
- 4World Health Organization, Department of Child and Adolescent Health and Development. The Treatment of Diarrhoea: A Manual for Physicians and Other Senior Health Workers. Geneva: World Health Organization, Department of Child and Adolescent Health and Development, 2005.
- 5Mondal D, Haque R, Sack RB, et al. Attribution of malnutrition to cause-specific Diarrheal illness: evidence from a prospective study of preschool children in Mirpur, Dhaka, Bangladesh. Am J Trop Med Hyg 2009;80:824–6.19407131 PMC 3410540 · pubmed ↗
- 6Ahmed S, Latham JR, Das SK, et al. Severity of diarrhea and malnutrition among under five-year-old children in rural Bangladesh. Am J Trop Med Hyg 2013;89:223–8. 10.4269/ajtmh.12-074323817334 PMC 3741240 · doi ↗ · pubmed ↗
- 7Tickell KD, Pavlinac PB, John-Stewart GC, et al. Impact of childhood nutritional status on pathogen prevalence and severity of acute diarrhea. Am J Trop Med Hyg 2017;97:1337–44. 10.4269/ajtmh.17-013929140236 PMC 5817755 · doi ↗ · pubmed ↗
- 8The ABCD study team. A double-blind placebo-controlled trial of azithromycin to reduce mortality and improve growth in high-risk young children with non-bloody diarrhoea in low resource settings: the antibiotics for children with diarrhoea (ABCD) trial protocol. Trials 2020;21. 10.1186/s 13063-019-3829-y PMC 695647831931848 · doi ↗ · pubmed ↗