Generalize the use of the kidney failure risk equation (KFRE) for better vascular access planning
Bernardo Marques da Silva, Joana Gameiro

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
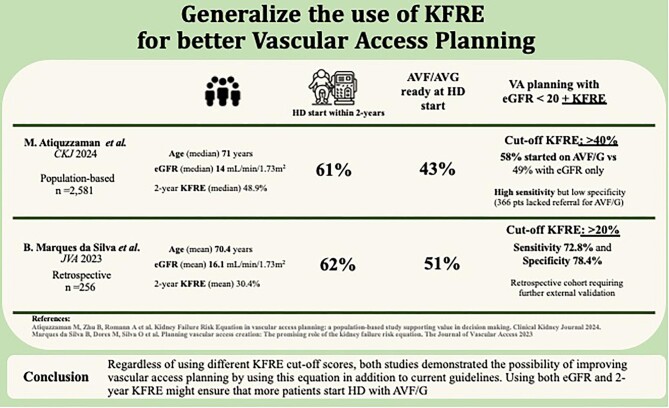 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Organ Donation and Transplantation · Acute Kidney Injury Research
To the Editor,
We were pleased to read the work by Atiquzzaman et al. concerning vascular access (VA) planning and the possibility of improvement by using the kidney failure risk equation (KFRE) [1]. Given the rising prevalence of chronic kidney disease (CKD) and the increasing number of patients requiring hemodialysis (HD), an effective VA [arteriovenous fistula or graft (AVF/G)] at the start of HD is crucial in ensuring optimal patient outcomes and quality of life [2]. Ideally, patients should be referred not only for VA creation in a timely manner, but also to prevent creation in patients who will not require HD. Referral criteria for AVF/G creation are still insufficient and rely on the nephrologist's perception of when HD will be required [3]. Therefore, developing tools to improve VA planning and timely creation is of utter importance.
In this recently published population-based study of 2581 participants with median age of 71 years, median eGFR at index 14.0 mL/min/1.73 m^2^, and 2-year KFRE of 48.9%, 61% of patients started HD within 2 years. Among those, 43% had AVF/G at HD start and had a significantly higher KFRE score (60 vs 29%, *P *< 0.001). More importantly, the authors demonstrated that using a KFRE cut-off >40% in addition to eGFR <20 mL/min/1.73 m^2^ significantly improved the adequateness of VA creation. Indeed, the proportion of patients who started HD on AVF/G within 2 years was 49% for eGFR threshold-based referral and of 58% when an adjunct KFRE of >40% was used. Despite the high sensitivity of this cut-off, the low specificity resulted in the lack of referral for AVF/G creation in 366 patients who started HD within 2 years.
Our retrospective study of 256 patients had a similar age and eGFR at referral for VA creation, and the mean 2-year KFRE score was 30.4% [4]. In a 2-year follow-up, 62.1% started HD. In this population, the optimal KFRE cut-off for VA referral was ⩾20%, which had a sensitivity of 72.8% and specificity of 78.4%. Eighty-four percent of patients with a KFRE ⩾20% started HD within 2 years. However, this was a retrospective cohort and would require external validation for a generalized use.
Regardless of using different KFRE cut-off scores, both studies demonstrated the possibility of improving VA planning by using this equation in addition to current guidelines, as described in Fig. 1. Using both eGFR and 2-year KFRE might ensure that more patients start HD with AVF/G and decrease unnecessary VA procedures. In an area so crucial for CKD patients, more studies should be undertaken to further improve and validate this additional tool in different population cohorts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atiquzzaman M, Zhu B, Romann A et al. Kidney failure risk equation in vascular access planning: a population-based study supporting value in decision making. Clin Kidney J 2024;10.1093/ckj/sfae 008PMC 1084762938327282 · doi ↗ · pubmed ↗
- 2Woo K, Lok CE. New insights into dialysis vascular access: What is the optimal vascular access type and timing of access creation in CKD and dialysis patients? Clin J Am Soc Nephrol 2016;11:1487–94. 10.2215/CJN.02190216.27401524 PMC 4974877 · doi ↗ · pubmed ↗
- 3Chapter 5: Referral to specialists and models of care. Kidney Int Suppl 2013;3:112–9. 10.1038/kisup.2012.68.PMC 428444225599001 · doi ↗ · pubmed ↗
- 4Marques da Silva B, Dores M, Silva O et al. Planning vascular access creation: the promising role of the kidney failure risk equation. J Vasc Access 2023;17. 10.1177/11297298231186373.37475542 · doi ↗ · pubmed ↗