Cleft closure and other predictors of contemporary outcomes after atrioventricular canal repair in patients with parachute left atrioventricular valve
Patrick B McGeoghegan, Minmin Lu, Lynn A Sleeper, Sitaram M Emani, Christopher W Baird, Eric N Feins, Laura A Gellis, Kevin G Friedman

TL;DR
This study examines the outcomes of repairing heart defects involving a parachute-shaped left atrioventricular valve and identifies factors that increase the risk of poor results.
Contribution
The study identifies predictors of adverse outcomes after repairing parachute left atrioventricular valve in patients with atrioventricular septal defect.
Findings
Leaving the cleft completely open during repair is associated with higher risk of poor outcomes.
Right-dominant AVSDs are at higher risk for LAVV reintervention.
Sixteen patients (44%) met the composite outcome of death, reintervention, or LAVV dysfunction within 2 years.
Abstract
Parachute left atrioventricular valve (LAVV) complicates atrioventricular septal defect (AVSD) repair. We evaluate outcomes of AVSD patients with parachute LAVV and identify risk factors for adverse outcomes. We evaluated all patients undergoing repair of AVSD with parachute LAVV from 2012 to 2021. The primary outcome was a composite of time-to-death, LAVV reintervention and development of greater than or equal to moderate LAVV dysfunction (greater than or equal to moderate LAVV stenosis and/or LAVV regurgitation). Event-free survival for the composite outcome was estimated using Kaplan–Meier methodology and competing risks analysis. Cox proportional hazards regression was used to identify predictors of the primary outcome. A total of 36 patients were included with a median age at repair of 4 months (interquartile range 2.3–5.5 months). Over a median follow-up of 2.6 years…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
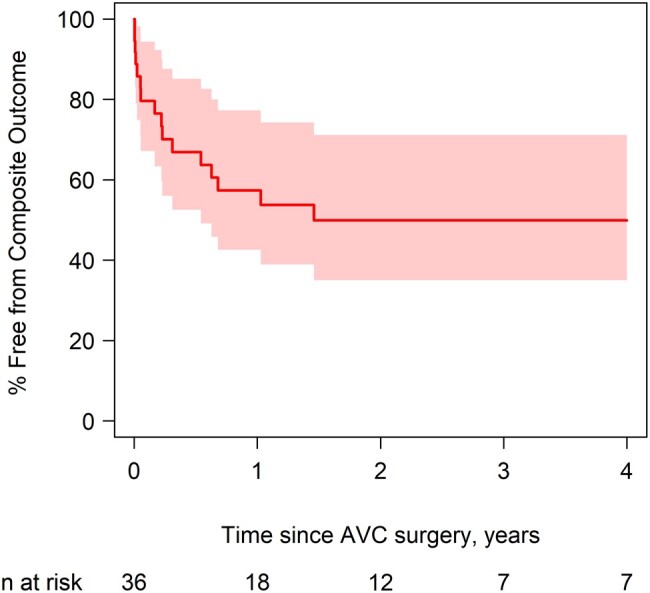 Figure 1
Figure 1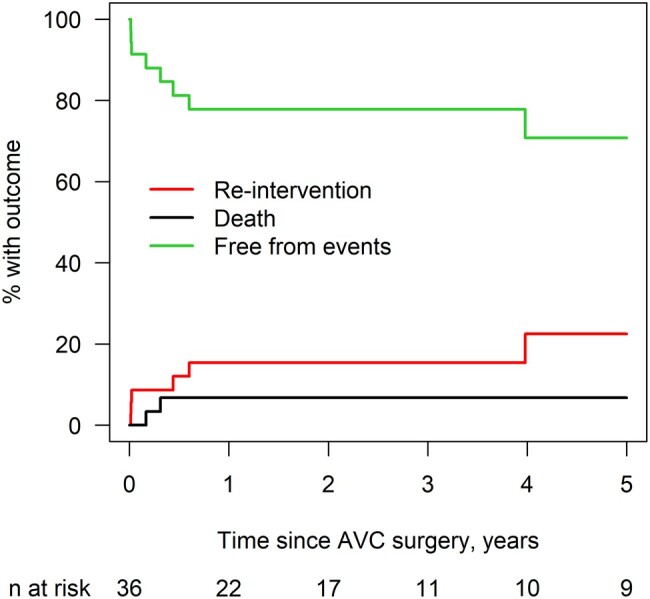 Figure 2
Figure 2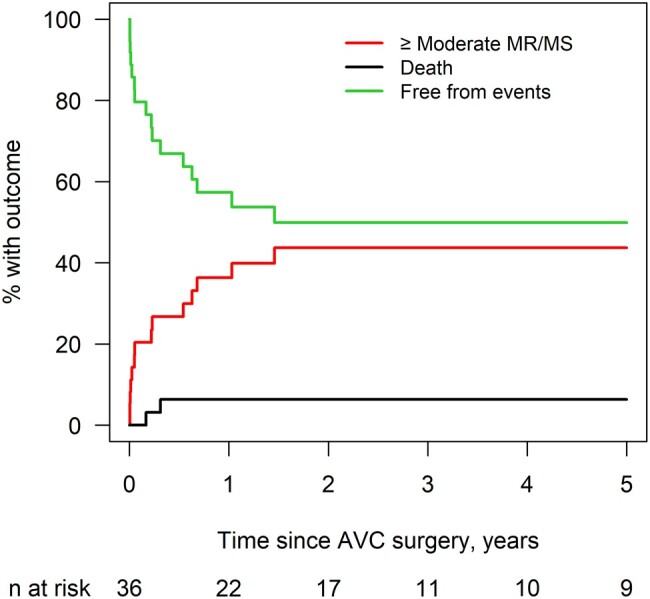 Figure 3
Figure 3| Composite outcome | |||||
|---|---|---|---|---|---|
| Variable | Overall ( | Yes ( | No ( | HR (95% CI) |
|
| Age at surgery (years) | 0.34 (0.19–0.46) | 0.31 (0.18–0.40) | 0.41 (0.20–1.02) | 0.25 (0.04–1.59) | 0.14 |
| Male | 7 (19.4%) | 3 (18.8%) | 4 (20.0%) | 1.55 (0.43, 5.55) | 0.50 |
| Weight at surgery (kg) | 4.60 (3.80–5.70) | 3.80 (3.36–5.22) | 4.65 (4.50–7.20) | 0.71 (0.48–1.05) | 0.09 |
| Known genetic disorder | 0.45 (0.16–1.25) | 0.13 | |||
| None | 18 (50.0%) | 10 (62.5%) | 8 (40.0%) | ||
| Trisomy 21 | 15 (41.7%) | 5 (31.3%) | 10 (50.0%) | ||
| Heterotaxy | 1 (2.8%) | 1 (6.3%) | 0 (0%) | ||
| Other | 2 (5.6%) | 0 (0%) | 2 (10.0%) | ||
| AV canal type | 0.13 | ||||
| Complete | 27 (75.0%) | 11 (68.8%) | 16 (80.0%) | 0.45 (0.16–1.25) | |
| Transitional | 9 (25.0%) | 5 (31.3%) | 4 (20.0%) | Ref | |
| Parachute type | 0.76 | ||||
| Complete parachute | 21 (58.3%) | 9 (56.3%) | 12 (60.0%) | 0.86 (0.32–2.31) | |
| | 15 (41.7%) | 7 (43.8%) | 8 (40.0%) | Ref | |
| AV canal balance | 0.26 | ||||
| Balanced | 11 (30.6%) | 3 (18.8%) | 8 (40.0%) | 0.49 (0.14–1.71) | |
| Right dominant | 25 (69.4%) | 13 (81.3%) | 12 (60.0%) | Ref | |
| Associated lesions | 35 (97.2%) | 16 (100%) | 19 (95.0%) | / | NA |
| Secundum ASD | 18 (50.0%) | 9 (56.3%) | 9 (45.0%) | 1.18 (0.44–3.19) | 0.74 |
| Additional VSD | 2 (5.6%) | 2 (12.5%) | 0 (0%) | – | NA |
| Coarctation of the aorta | 2 (5.6%) | 2 (12.5%) | 0 (0%) | – | NA |
| LVOT obstruction/concurrent subaortic stenosis/aortic stenosis | 4 (11.1%) | 2 (12.5%) | 2 (10.0%) | 0.87 (0.20–3.84) | 0.85 |
| Left superior vena cava to coronary sinus | 6 (16.7%) | 3 (18.8%) | 3 (15.0%) | 1.01 (0.29–3.56) | 0.99 |
| Composite outcome | |||||
|---|---|---|---|---|---|
| Variable | Overall ( | Yes ( | No ( | HR (95% CI) |
|
| Left ventricular ejection fraction (%) | 56 (55–61) | 56.1 (50–60) | 56 (55–62) | 0.95 (0.88–1.02) | 0.17 |
| Qualitative LV function | 2.26 (0.78–6.55) | 0.13 | |||
| Normal | 30 (83.3%) | 11 (68.8%) | 19 (95.0%) | ||
| Mild | 5 (13.9%) | 4 (25.0%) | 1 (5.0%) | ||
| Mild–moderate | 0 | 0 | 0 | ||
| Moderate | 0 | 0 | 0 | ||
| Moderate–severe | 0 | 0 | 0 | ||
| Severe | 1 (2.8%) | 1 (6.3%) | 0 (0%) | ||
| AVVR degree | |||||
| None or trivial | 3 (8.3%) | 2 (12.5%) | 1 (5.0%) | ||
| Mild | 17 (47.2%) | 5 (31.3%) | 12 (60.0%) | ||
| Mild–moderate | 10 (27.8%) | 5 (31.3%) | 5 (25.0%) | ||
| Moderate | 1 (2.8%) | 1 (6.3%) | 0 (0%) | 1.89 (0.70–5.11) | 0.21 |
| Moderate–severe | 3 (8.3%) | 1 (6.3%) | 2 (10.0%) | ||
| Surgical history | 1.64 (0.59–4.54) | 0.34 | |||
| Coarctation repair | 4 (11.1%) | 2 (12.5%) | 2 (10.0%) | 1.15 (0.26–5.09) | 0.85 |
| Pulmonary artery band | 7 (19.4%) | 4 (25.0%) | 3 (15.0%) | 1.56 (0.50–4.86) | 0.44 |
| Patent ductus arteriosus ligation | 3 (8.3%) | 1 (6.3%) | 2 (10.0%) | 0.61 (0.08–4.61) | 0.63 |
| Stage I/bidirectional Glenn/hybrid | 3 (8.3%) | 2 (12.5%) | 1 (5.0%) | 2.78 (0.63–12.35) | 0.18 |
| Other | 5 (13.9%) | 2 (12.5%) | 3 (15.0%) | 0.83 (0.19–3.65) | 0.80 |
| Pre-op weight (kg) | 4.45 (3.70, 6.00) | 3.80 (3.47, 5.16) | 4.60 (4.20, 7.16) | 0.74 (0.52–1.05) | 0.09 |
| Pre-op height (cm) | 56.5 (52.8, 62.0) | 54.5 (52.0, 58.5) | 57.8 (53.4, 72.3) | 0.95 (0.90–1.01) | 0.11 |
| Pre-op BSA (m2) | 0.27 (0.24, 0.33) | 0.24 (0.23, 0.29) | 0.28 (0.25, 0.38) | 0.23 (0.00–34.85) | 0.57 |
| Repair strategy | |||||
| Single patch | 3 (8.3%) | 1 (6.3%) | 2 (10.0%) | 0.49 (0.06–3.74) | 0.49 |
| Double patch | 23 (63.9%) | 10 (62.5%) | 13 (65.0%) | 0.99 (0.36–2.74) | 0.99 |
| Modified single patch | 1 (2.8%) | 0 (0%) | 1 (5.0%) | – | NA |
| Primum ASD closure | 9 (25.0%) | 5 (31.3%) | 4 (20.0%) | 1.69 (0.59–4.88) | 0.33 |
| VSD closure | 8 (22.2%) | 4 (25.0%) | 4 (20.0%) | 1.26 (0.41–3.93) | 0.69 |
| Other | 0 | 0 | 0 | – | NA |
| Degree of cleft closure |
| ||||
| Full | 9 (25.7%) | 5 (31.3%) | 4 (21.1%) | Ref | |
| Partial | 23 (65.7%) | 8 (50.0%) | 15 (78.9%) | 0.54 (0.18–1.65) | |
| None | 3 (8.6%) | 3 (18.8%) | 0 (0%) | 4.09 (0.87–19.25) | |
| LAVV repair techniques | 27 (75.0%) | 11 (68.8%) | 16 (80.0%) | 0.76 (0.27–2.20) | 0.62 |
| Papillary muscle splitting/moving | 14 (38.9%) | 5 (31.3%) | 9 (45.0%) | 0.64 (0.22–1.84) | 0.41 |
| Chord division | 5 (13.9%) | 1 (6.3%) | 4 (20.0%) | 0.30 (0.04–2.27) | 0.24 |
| Annuloplasty | 3 (8.3%) | 1 (6.3%) | 2 (10.0%) | 1.15 (0.15–8.74) | 0.90 |
| Leaflet patch augmentation | 3 (8.3%) | 2 (12.5%) | 1 (5.0%) | 1.48 (0.33–6.55) | 0.61 |
| Chord placement | 1 (2.8%) | 1 (6.3%) | 0 (0%) | – | NA |
| Commissuroplasty | 0 | 0 | 0 | – | NA |
| Concurrent repairs | 35 (97.2%) | 16 (100%) | 19 (95.0%) | – | NA |
| PDA ligation | 12 (33.3%) | 5 (31.3%) | 7 (35.0%) | 0.89 (0.31–2.56) | 0.83 |
| Coarctation repair | 2 (5.6%) | 2 (12.5%) | 0 (0%) | – | NA |
| Tricuspid valve repair | 28 (77.8%) | 13 (81.3%) | 15 (75.0%) | 1.93 (0.55–6.83) | 0.31 |
| Fenestrated ASD closure | 12 (33.3%) | 7 (43.8%) | 5 (25.0%) | 1.40 (0.52–3.76) | 0.51 |
| LVOT intervention | 4 (11.1%) | 1 (6.3%) | 3 (15.0%) | 0.40 (0.05–3.07) | 0.38 |
| Damus–Kaye–Stansel/stage I/Glenn/Hybrid takedown | 2 (5.6%) | 1 (6.3%) | 1 (5.0%) | 1.39 (0.18–10.55) | 0.75 |
| PA band takedown | 7 (19.4%) | 4 (25.0%) | 3 (15.0%) | 1.56 (0.50–4.86) | 0.44 |
| Secundum ASD closure | 15 (41.7%) | 7 (43.8%) | 8 (40.0%) | 0.96 (0.36–2.58) | 0.94 |
| Other | 17 (47.2%) | 8 (50.0%) | 9 (45.0%) | 0.765 | 0.48 |
| Multiple bypass runs during primary repair | 0.76 | ||||
| Yes | 4 (11.1%) | 2 (12.5%) | 2 (10.0%) | 1.26 (0.28–5.54) | |
| No | 32 (88.9%) | 14 (87.5%) | 18 (90.0%) | Ref | |
| Time since surgery | % Free from Composite Outcome (95% CI) |
|---|---|
| 0.5 years | 67 (48–80) |
| 1 year | 57 (39–72) |
| 1.5 years | 50 (31–66) |
| 5 years | 50 (31–66) |
|
| |
| Time since surgery | % Reintervention (95% CI) | % death (95% CI) |
|---|---|---|
| 3 months | 8.7 (2.2–21.0) | 3.4 (0.2–15.0) |
| 6 months | 12.0 (3.7–25.7) | 6.8 (1.1–19.7) |
| 9 months | 15.4 (5.5–30.1) | 6.8 (1.1–19.7) |
| 1 year | 15.4 (5.5–30.1) | 6.8 (1.1–19.7) |
| 3 years | 15.4 (5.5–30.1) | 6.8 (1.1–19.7) |
| 5 years | 22.5 (7.7–42.0) | 6.8 (1.1–19.7) |
|
| ||
| Reintervention | |||||
|---|---|---|---|---|---|
| Variable | Overall ( | Yes ( | No ( | HR (95% CI) |
|
| Age at surgery (years) | 0.34 (0.19–0.46) | 0.28 (0.10–0.44) | 0.34 (0.19–0.50) | 0.16 (0.01–4.40) | 0.28 |
| Male | 7 (19.4%) | 0 (0%) | 7 (23.3%) | / | NA |
| Weight at surgery (kg) | 4.6 (3.8–5.7) | 4.3 (3.4–5.4) | 4.6 (3.8–6.8) | 0.78 (0.48–1.26) | 0.31 |
| Known genetic disorder | 0.16 (0.02–1.49) | 0.11 | |||
| None | 18 (50.0%) | 5 (83.3%) | 13 (43.3%) | ||
| Trisomy 21 | 15 (41.7%) | 1 (16.7%) | 14 (46.7%) | ||
| Heterotaxy | 1 (2.8%) | 0 (0%) | 1 (3.3%) | ||
| AV canal type |
| ||||
| Complete parachute | 27 (75.0%) | 2 (33.3%) | 25 (83.3%) | Ref | |
| Transitional | 9 (25.0%) | 4 (66.7%) | 5 (16.7%) | 7.69 (1.56–33.33) | |
| Parachute type | 0.30 | ||||
| Complete | 21 (58.3%) | 5 (83.3%) | 16 (53.3%) | 3.15 (0.36–27.37) | |
| Forme fruste | 15 (41.7%) | 1 (16.7%) | 14 (46.7%) | Ref | |
| AV canal balance | NA | ||||
| Balanced | 11 (30.6%) | 0 (0%) | 11 (36.7%) | / | |
| Right dominant | 25 (69.4%) | 6 (100%) | 19 (63.3%) | / | |
| Associated lesions | 35 (97.2%) | 6 (100%) | 29 (96.7%) | / | NA |
| ASD | 18 (50.0%) | 4 (66.7%) | 14 (46.7%) | 2.01 (0.41–9.95) | 0.39 |
| VSD | 2 (5.6%) | 0 (0%) | 2 (6.7%) | – | NA |
| Coarctation of the aorta | 2 (5.6%) | 2 (33.3%) | 0 (0%) | – | NA |
| LVOT obstruction/concurrent subaortic stenosis/aortic stenosis | 4 (11.1%) | 0 (0%) | 4 (13.3%) | – | NA |
| Left superior vena cava to coronary sinus | 6 (16.7%) | 0 (0%) | 6 (20.0%) | – | NA |
| Reintervention | |||||
|---|---|---|---|---|---|
| Variable | Overall ( | Yes ( | No ( | HR (95% CI) |
|
| Left ventricular ejection fraction (%) | 56 (55–61) | 58.50 (46–65) | 56 (55–59.10) | 0.96 (0.84–1.09) | 0.51 |
| Qualitative LV function | 2.24 (0.40–12.46) | 0.36 | |||
| Normal | 30 (83.3%) | 4 (66.7%) | 26 (86.7%) | Ref | |
| Mild | 5 (13.9%) | 1 (16.7%) | 4 (13.3%) | ||
| Mild–moderate | 0 | 0 | 0 | ||
| Moderate | 0 | 0 | 0 | ||
| Moderate–severe | 0 | 0 | 0 | ||
| Severe | 1 (2.8%) | 1 (16.7%) | 0 (0%) | ||
| AVVR degree | |||||
| None or trivial | 3 (8.3%) | 0 (0%) | 3 (10.0%) | ||
| Mild | 17 (47.2%) | 1 (16.7%) | 16 (53.3%) | ||
| Mild–moderate | 10 (27.8%) | 3 (50.0%) | 7 (23.3%) | ||
| Moderate | 1 (2.8%) | 0 (0%) | 1 (3.3%) | 8.09 (1.35–48.56) |
|
| Moderate–severe | 3 (8.3%) | 1 (16.7%) | 2 (6.7%) | ||
| Surgical history | 11 (30.6%) | 3 (50.0%) | 8 (26.7%) | 2.30 (0.49–10.78) | 0.29 |
| Coarctation repair | 4 (11.1%) | 1 (16.7%) | 3 (10.0%) | 1.25 (0.22–7.28) | 0.80 |
| Pulmonary artery band | 7 (19.4%) | 1 (16.7%) | 6 (20.0%) | 0.73 (0.11–5.12) | 0.76 |
| Patent ductus arteriosus ligation | 3 (8.3%) | 0 (0%) | 3 (10.0%) | / | NA |
| Stage I/bidirectional Glenn/Hybrid | 3 (8.3%) | 2 (33.3%) | 1 (3.3%) | 11.57 (1.92–69.62) |
|
| Other | 5 (13.9%) | 1 (16.7%) | 4 (13.3%) | 1.28 (0.13–12.35) | 0.83 |
| Pre-op weight (kg) | 4.45 (3.70, 6.00) | 3.75 (3.34, 5.40) | 4.55 (3.80, 6.80) | 0.74 (0.43–1.27) | 0.27 |
| Pre-op height (cm) | 56.5 (52.8, 62.0) | 53.5 (52.0, 58.5) | 57.3 (53.0, 64.0) | 0.94 (0.87–1.01) | 0.12 |
| Pre-op BSA (m2) | 0.27 (0.24, 0.33) | 0.24 (0.22, 0.33) | 0.27 (0.24, 0.32) | 1.20 (0.05–27.65) | 0.91 |
| Repair strategy | |||||
| Single patch | 3 (8.3%) | 0 (0%) | 3 (10.0%) | – | NA |
| Double patch | 23 (63.9%) | 2 (33.3%) | 21 (70.0%) | 0.25 (0.05–1.21) | 0.08 |
| Modified single patch | 1 (2.8%) | 0 (0%) | 1 (3.3%) | – | NA |
| Primum ASD closure | 9 (25.0%) | 4 (66.7%) | 5 (16.7%) | 7.68 (1.55–37.98) |
|
| VSD closure | 8 (22.2%) | 3 (50.0%) | 5 (16.7%) | 4.16 (0.89–19.53) | 0.07 |
| Degree of cleft closure | 0.67 | ||||
| Full | 9 (25.7%) | 2 (33.3%) | 7 (24.1%) | 0.75 (0.06–9.48) | |
| Partial | 23 (65.7%) | 3 (50.0%) | 20 (69.0%) | 0.39 (0.03–4.41) | |
| None | 3 (8.6%) | 1 (16.7%) | 2 (6.9%) | Ref | |
| LAVV repair techniques | 27 (75.0%) | 5 (83.3%) | 22 (73.3%) | 1.95 (0.24–16.06) | 0.54 |
| Papillary muscle splitting/moving | 14 (38.9%) | 1 (16.7%) | 13 (43.3%) | 0.29 (0.03–2.50) | 0.26 |
| Chord division | 5 (13.9%) | 1 (16.7%) | 4 (13.3%) | 0.92 (0.15–5.43) | 0.92 |
| Annuloplasty | 3 (8.3%) | 1 (16.7%) | 2 (6.7%) | 2.87 (0.30–27.30) | 0.36 |
| Leaflet patch augmentation | 3 (8.3%) | 1 (16.7%) | 2 (6.7%) | 2.19 (0.26–18.51) | 0.47 |
| Chord placement | 1 (2.8%) | 1 (16.7%) | 0 (0%) | – | NA |
| Concurrent repairs | 35 (97.2%) | 6 (100%) | 29 (96.7%) | – | NA |
| Coarctation repair | 2 (5.6%) | 2 (33.3%) | 0 (0%) | – | NA |
| Tricuspid valve repair | 28 (77.8%) | 5 (83.3%) | 23 (76.7%) | 2.14 (0.25–18.09) | 0.48 |
| Fenestrated ASD closure | 12 (33.3%) | 2 (33.3%) | 10 (33.3%) | 0.94 (0.17–5.16) | 0.94 |
| LVOT intervention | 4 (11.1%) | 0 (0%) | 4 (13.3%) | – | NA |
| Damus–Kaye–Stansel/stage 1/Glenn/Hybrid takedown | 2 (5.6%) | 1 (16.7%) | 1 (3.3%) | 4.71 (0.62–35.70) | 0.13 |
| PA band takedown | 7 (19.4%) | 1 (16.7%) | 6 (20.0%) | 0.73 (0.11–5.12) | 0.76 |
| Secundum ASD closure | 15 (41.7%) | 3 (50.0%) | 12 (40.0%) | 1.24 (0.27–5.80) | 0.78 |
| Other | 17 (47.2%) | 3 (50.0%) | 14 (46.7%) | 1.36 (0.29–6.51) | 0.70 |
| Multiple bypass runs | 0.72 | ||||
| Yes | 4 (11.1%) | 1 (16.7%) | 3 (10.0%) | 1.54 (0.15–16.27) | |
| No | 32 (88.9%) | 5 (83.3%) | 27 (90.0%) | Ref | |
| Time since surgery | % Moderate MR/MS (95% CI) | % death (95% CI) |
|---|---|---|
| 3 months | 26.8 (13.1–42.6) | 3.2 (0.2–14.3) |
| 6 months | 26.8 (13.1–42.6) | 6.4 (1.1–18.7) |
| 9 months | 36.3 (20.1–52.7) | 6.4 (1.1–18.7) |
| 1 year | 36.3 (20.1–52.7) | 6.4 (1.1–18.7) |
| 3 years | 43.7 (25.7–60.4) | 6.4 (1.1–18.7) |
| 5 years | 43.7 (25.7–60.4) | 6.4 (1.1–18.7) |
|
| ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac Valve Diseases and Treatments · Congenital Heart Disease Studies
INTRODUCTION
Repair of atrioventricular septal defects (AVSDs) is now routinely performed in infancy with good surgical outcomes and a low risk of reoperation [1–3]. In several large cohort studies, freedom from reoperation following AVSD repair is ∼85% at 10–20 years [1, 2, 4]. Left atrioventricular valve regurgitation (LAVVR) is the most common indication for repeat surgery [4–6], and anomalies of the left atrioventricular valve (LAVV) can complicate repair [6, 7]. Patients with AVSD and LAVV leaflets supported by a single papillary muscle (parachute LAVV) or 2 closely spaced papillary muscles and maldistribution of chordae (forme fruste parachute) are at higher risk for postoperative left atrioventricular valve stenosis (LAVVS), LAVVR and future need for LAVV repair or replacement [8, 9]. In the setting of a parachute LAVV, closure of the cleft can result in stenosis, while leaving the cleft open can predispose to LAVVR [8–10]. A single-centre study evaluating patients with complete AVSD and parachute LAVV undergoing repair between 2001 and 2012 found a high burden of reoperation (28% at 4 years) [9]. These patients may require a series of LAVV interventions to address residual LAVV disease [11, 12]. Faced with a parachute-type LAVV in AVSD, some institutions choose to abandon biventricular repair due to concerns about valve function and opt for single-ventricle palliation [9, 13]. Given the challenges in single-ventricle palliation [14–16], it is important to provide contemporary surgical outcomes of biventricular repair for patients with AVSD and parachute LAVV. Further, anatomic, echocardiographic and surgical predictors of adverse cardiac outcomes are scarce and may benefit clinical management of this patient population. Hence, the aims of the current study were to: (i) to describe contemporary medium-term postoperative outcomes following AVSD repair in patients with parachute LAVV, and (ii) identify factors associated with these adverse outcomes after repair.
METHODS
Ethics statement
This study was approved by the Boston Children’s Hospital Institutional Review Board (IRB-P00041642) on 3 March 2022. Patient written informed consent was waived by our Institutional Review Board, and this study complies with the ethical principles of the Declaration of Helsinki.
Patient population
We included patients with AVSD and either parachute or forme fruste parachute LAVV who underwent full biventricular repair at Boston Children’s Hospital between 1 January 2012 and 1 January 2021. This included patients who underwent full repair of balanced or unbalanced AVSD and complete, transitional or partial defects. In this cohort, however, there were no patients with partial AVSD. Exclusion criteria included AVSD septation as part of staged left ventricular recruitment, double-orifice LAVV or clinically significant pulmonary vein stenosis. The primary outcome was a composite of death, LAVV reintervention (repair or replacement) and development of greater than or equal to moderate LAVV dysfunction (defined as mean LAVV inflow gradient ≥8 mmHg and/or greater than or equal to moderate qualitative grade of LAVVR). Secondary outcomes included LAVV reintervention and greater than or equal to moderate LAVV dysfunction (either LAVVR or LAVVS).
Definitions
Parachute LAVV was defined as a single left ventricular papillary muscle and no mural leaflet; forme fruste parachute LAVV was defined as 2 closely spaced papillary muscles and a diminutive mural leaflet. Transitional AVSD was defined by a small, restrictive ventricular septal defect, a primum atrial septal defect (ASD) and a common atrioventricular (AV) valve. Associated cardiac lesions involved assessment for additional ASDs or ventricular septal defects, coarctation of the aorta, double outlet right ventricle, left ventricular outflow tract obstruction, subaortic stenosis, aortic stenosis, persistent left superior vena cava to coronary sinus, sub-pulmonary/pulmonary stenosis, transposition of the great arteries and tetralogy of Fallot.
Data collection
Patient medical records were used to extract demographics, anatomy, surgical characteristics and echocardiographic data. Echocardiographic data (including degree of LAVVS and LAVVR) were taken from preoperative transthoracic echocardiograms (TTE) and immediate postoperative transoesophageal echocardiograms. LAVVS was measured using mean LAVV inflow gradient on continuous-wave Doppler (mmHg) in the apical 4-chamber view with sample volume placed at the LAVV leaflet tips, and measurements were averaged over 3 beats. Left ventricle (LV) systolic dysfunction was defined as ejection fraction <55%. Exploratory TTE variables were assessed by a cardiologist blinded to outcomes and were used to quantify level of unbalance and leaflet pathology. All exploratory TTE variables were indexed to body surface area (BSA) either through calculating z-scores [17, 18] or (variable) BSA ratios. These variables include LV end-diastolic volume (LVEDV) z-score, atrioventricular valve index [19, 20], RV/LV inflow angle [19, 20], left AV area (subcostal short axis)/BSA, LAVV diameter/BSA, LAVV inflow diameter/BSA, left AV inflow diameter/total diameter [20] and right AV area (subcostal short axis)/BSA.
LAVV repair strategies were not uniform and were at the discretion of the operating surgeon. Primary repair strategies involved either single-patch, double-patch or modified single-patch for complete AVSDs, and primum ASD closure with or without ventricular septal defect closure for transitional canals. LAVV interventions included no, partial or complete cleft closure, papillary muscle splitting or mobilization, chordal division or placement, annuloplasty, leaflet patch augmentation and commissuroplasty. Concurrent repairs at the time of primary AV canal surgery were also recorded and included coarctation repair, fenestrated ASD closure, left ventricular outflow tract surgery and single-ventricle takedown. The need for multiple cardiopulmonary bypass runs was also recorded.
Statistical analysis
Comparisons between presence and absence of an outcome were assessed using Student’s t-test or Wilcoxon rank sum test. For comparisons of categorical variables, a Fisher’s exact test was performed. Competing risks cumulative incidence functions were estimated to describe time-to-event for LAVV reintervention, death and greater than or equal to moderate LAVV dysfunction. Kaplan–Meier methodology was used to estimate freedom from the composite outcome. Predictor variables included those shown in Tables 1 and 2. Univariate associations between predictors and the component outcomes were assessed by subdistribution Cox proportional hazards regression in the competing risks framework [21] and Cox regression (for the composite outcome). For multivariable model construction for the composite outcome, stepwise selection was used, with a criterion for entry into the model of P < 0.15 and the criterion for remaining in the model was P < 0.05. A P-value < 0.05 was considered statistically significant. Analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC) and R version 4.1.2.
RESULTS
Demographics
From 2012 to 2021, 36 AVSD patients with parachute LAVV underwent repair with baseline characteristics in Table 1. Overall, 21 (58%) had parachute LAVV and 15 (42%) had forme fruste parachute. Most patients had a complete AVSD (n = 27, 75%), while 9 (25%) had a transitional AVSD. The majority (n = 25, 69%) had right-dominant AVSD (7 with transitional AVSD and 18 with complete AVSD), while 11 had balanced AVSD (2 with transitional AVSD and 9 with complete AVSD). The median LVEDV z-score was 0.25 (interquartile range –1.63 to 0.58) and among those with right-dominant AV canals, 6 (24%) had a LVEDV z-score < –2.
Median age at primary AVSD repair was 4.1 months (interquartile range 2.3–5.5 months). Most patients (75%) had mild or mild-to-moderate AV valve regurgitation (AVVR) before primary repair. Surgical repair strategies are outlined in Table 2. In patients with complete AVSD, 23 had two-patch repair, 3 had single-patch and 1 modified single-patch (Australian) repair. The cleft was partially closed in 23 patients (64%), completely closed in 9 patients (25%) and left open in 3 patients (8%). Fourteen patients had splitting of a papillary muscle (39%) and 5 (14%) underwent division of LAVV chordae.
Outcomes
Among those who survived, median follow-up was 2.6 years (interquartile range 1.0–5.6 years). Sixteen (44%) patients met the composite outcome with 3 deaths, 6 LAVV reinterventions and 14 patients who developed greater than or equal to moderate LAVVR or a LAVVS gradient ≥8 mmHg. Freedom from the composite outcome (Fig. 1) declined rapidly over the 1st year following AVSD repair with 67% at 6 months and 50% at 1.5 years. All patients who experienced the composite outcome did so within 2 years of primary AVSD repair. Degree of cleft closure was the only statistically significant predictor of the composite in multivariate analysis. No cleft closure was associated with increased risk of experiencing the composite outcome when compared to partial or complete cleft closure in both univariate [hazard ratio (HR) 4.09, P = 0.02] and multivariate analysis (HR 7.62, P = 0.02) (Table 2, Supplementary Material, Table S1).
Estimated Kaplan–Meier freedom from composite outcome with pointwise 95% confidence bands. No events after 2 years.Kaplan-Meier Freedom from Composite Outcome.
**: **
Among the 3 patients who had no cleft closure, 2 had complete AVSD (1 balanced, 1 right-dominant) and 1 had transitional, right-dominant AVSD. Two patients had mild–moderate AVVR prior to surgery and 1 had severe AVVR requiring hospitalization with inotropes prior to surgery. One patient underwent papillary muscle splitting during primary repair, and another required posterior annuloplasty to better approximate the mural leaflet to the inferior bridging leaflet.
All 3 repairs only required 1 bypass run, and there was no initial attempt at cleft closure (as it was felt that the valve orifice in all 3 patients precluded closure). One patient died, 1 developed LAVVR alone and 1 developed LAVVR requiring 2 sequential LAVV repairs on postop days 5 and 6 to correct it. The repairs 1st involved suture cleft closure and annuloplasty followed by patch cleft closure and placement of artificial chordae.
Figure 2 displays the competing risk cumulative incidence of death and LAVV reintervention over 5 years post AVSD repair. Six patients (18%) underwent LAVV reintervention (5 surgical and 1 catheter balloon dilation), resulting in LAVV reintervention incidence of 15% at 1 and 3 years. All 6 patients had greater than or equal to moderate LAVV dysfunction (3 with greater than or equal to moderate LAVVR, 2 with greater than or equal to moderate LAVVS and 1 with both greater than or equal to moderate LAVVR and LAVVS) prior to reintervention. All 6 patients who underwent LAVV reintervention had right-dominant AVSD.
Cumulative incidence of LAVV reintervention (6 events) and death (2 events). No events occurred after 5 years. LAVV: left atrioventricular valve.Cumulative incidence.
**: **
Of the 6 LAVV reinterventions, 3 occurred within 2 weeks of primary AVSD repair, while 5 occurred within 8 months. Of these patients, 4 underwent more than 1 reintervention and 3 ultimately had a LAVV replacement. Two of these patients underwent an initial surgical LAVV repair followed by replacement. One patient underwent 3 LAVV reinterventions prior to replacement. Significant comorbidities were associated with replacement, with 1 death, 2 pacemaker placements and 1 patient with subsequent Melody valve balloon dilation and need for additional valve replacement surgery.
During follow-up, there were 3 deaths, 2 of which occurred within 3 months of primary AVSD repair and without postoperative LAVV dysfunction or reintervention. One death occurred after LAVV reintervention and subsequent replacement.
Factors associated with LAVV reintervention in univariate analysis were transitional AVSD (vs complete AVSD) (HR 7.69, P = 0.01), a history of initial single-ventricle palliation prior to full AVSD repair (HR 11.57, P = 0.007) and greater than or equal to moderate AVVR on preoperative TTE (HR 8.09, P = 0.02) (Tables 3 and 4). All 6 patients who underwent LAVV reintervention had right-dominant AVSD. LAVV function on immediate postoperative transoesophageal echocardiogram was analysed by qualitative degree of LAVVR and LAVVS mean gradient. These values were not predictive of LAVV reintervention.
Competing risk curves in Fig. 3 show that by 1 year, the risk for development of greater than or equal to moderate LAVV dysfunction (LAVVS and/or LAVVR) is 36% and 44% by 3 years. Overall, 14 (39%) patients developed greater than or equal to moderate LAVV dysfunction (5 with greater than or equal to moderate LAVVR, 5 with greater than or equal to moderate LAVVS and 4 with both greater than or equal to moderate LAVVS and LAVVR). Univariate risk factors for greater than or equal to moderate LAVVS and/or LAVVR were younger age at surgery (HR 0.20; CI 0.05–0.82; P = 0.025), lower weight at surgery (HR 0.67; CI 0.47–0.96, P = 0.030) and preoperative LV dysfunction (HR 2.97; CI 1.22–7.27; P = 0.017).
Cumulative Incidence of at least moderate LAVVR/LAVVS (14 events), and death (2 events). No events occurred after 5 years. LAVVR: left atrioventricular valve regurgitation; LAVVS: left atrioventricular valve stenosis.Cumulative incidence.
**: **
Of the exploratory TTE variables collected, none were predictive of the outcomes (Supplementary Material, Tables S2 and S3).
DISCUSSION
In this study, we describe contemporary, medium-term outcomes after full repair of AVSD with parachute LAVV. This remains a high-risk population with 44% of patients having greater than or equal to moderate valve dysfunction, LAVV reintervention or death within 18 months of surgery. We also found that the majority of LAVV reinterventions were performed within 8 months of primary repair, and all LAVV reinterventions were performed in patients with a right-dominant AVSD. Leaving the cleft open was independently associated with increased risk of the composite of death, LAVV dysfunction and reintervention.
Despite continued evolution and improvement in surgical techniques, we found a high burden of LAVV reintervention and dysfunction over follow-up. Myers et al. from Boston Children’s Hospital previously analysed our institutional experience with biventricular repair in patients with complete AVSDs and parachute LAVV from 2001 to 2012. Our cohort had a similar freedom from LAVV reintervention 1 year post AVSD repair but a higher freedom from LAVV reintervention at 3 years. Both of our cohorts were skewed towards high-risk patients as evidenced by the high prevalence of unbalanced, right-dominant AVSD patients (69% of included patients in this study vs 67% in Myers study). Overall, this suggests a modest incremental improvement in reoperation rates between surgical eras. Furthermore, all LAVV reinterventions in the present study occurred in patients with unbalanced, right-dominant canal defects, which is concordant with Myers et al. who showed that an indexed LVEDV <20 ml/m^2^ resulted in statistically significant lower survival and increased proportion of LAVV reintervention.
The alternative management strategy for right-dominant AVSD patients is single-ventricle palliation. Although the LAVV reintervention rate in our cohort is relatively high, medium-term survival was >90%. These mortality and reintervention rates compare favourably to single-ventricle palliation outcomes, with prior publications showing high mortality (40%) and reintervention (60%) in unbalanced AVSD patients undergoing single-ventricle palliation [15]. These outcome data support the concept of primary biventricular repair or biventricular conversion as compared with single-ventricle palliation in this patient group when the LV is adequate in size but also emphasizes that there is significant risk of LAVV reintervention [10, 15, 22–24, 25].
Management of the cleft in AVSD patients, particularly in those with parachute-type LAVV, remains a challenge. Complete, and, in some cases, partial cleft closure is not feasible in patients with parachute LAVV as this would result in minimal inflow orifice and significant stenosis, while leaving the cleft completely open has been identified as a risk factor for development of postoperative LAVVR in prior studies [8–10]. Over the last 30–40 years, there has been a gradual evolution towards closing the cleft whenever possible, even in the setting of an abnormal LAVV. Data from the Mayo Clinic analysed long-term outcomes of surgical repair of 28 AVSD patients with parachute LAVV from 1977 to 2010 [7]. In this earlier era, the cleft was typically left open, and LAVVR was common and frequently led to reoperation. In the cohort from 2001 to 2012 at our institution in which the cleft was generally closed as much as deemed possible, Myers et al. described results like ours with indications for LAVV reintervention in their cohort distributed among LAVVR (60%), LAVVS (20%) or mixed valve disease (20%). The increase in proportion of patients undergoing LAVV reintervention for LAVVS or mixed LAVV disease in both our study and Myers et al. is likely related to the trend towards more aggressive cleft closure in the contemporary management of this patient population.
In our study, leaving the cleft completely open was independently associated with the composite outcome of death, reintervention and LAVVS and/or LAVVR. In this small cohort, it is difficult to determine if this finding is related to severity and complexity of valvar disease and LAVV hypoplasia versus surgical technique.
Therefore, larger, multicentre studies with central review of imaging data are needed to further explore how surgical management of the cleft influences medium and long-term outcomes in this patient population.
When managing a cleft deemed ineligible for suture closure, our institutional practice over the study duration was to close the cleft as fully as possible based on surgeon’s judgement and to utilize several strategies at both the base of the cleft and the papillary muscle. Decreasing annular dimension at the base of the cleft can reduce tension and decrease the chance of regurgitation. Furthermore, gently inverting or folding the superior and inferior bridging leaflets down into the ventricle can create more coaptation height at the cleft base. The papillary muscle is generally split to improve LAVV inflow, but this can come at the cost of splaying of the leaflets along the cleft and subsequent LAVVR. There is no specific rule for the degree of PM splitting, but one must balance opening up the inflow without predisposing to LAVVR.
Existing data on echocardiographic predictors of clinical outcomes for AVSD patients with parachute LAVV are scant. We found that greater than or equal to moderate AVVR prior to repair was associated with increased risk of LAVV reintervention. We evaluated a number exploratory preoperative TTE variables but found no significant associations with LAVV dysfunction or reintervention.
Limitations
This study is limited by its single-centre, retrospective design. Because of the small sample and small number of primary outcome events, as well as patient heterogeneity, our study is underpowered to detect some associations that may be clinically significant. For this reason, future studies with analysis of echocardiographic predictors in a larger cohort of patients may be of interest. Additionally, follow-up times are short, there is no universal indication for LAVV reintervention following AV canal repair, and there is a lack of consensus in surgical management of the LAVV (particularly management of the LAVV cleft).Finally, surgical techniques have evolved over the study period and differ by surgeon.
CONCLUSIONS
Repair of AVSD with parachute LAVV remains a clinical challenge with a high rate of LAVV reintervention and valvar dysfunction in medium-term follow-up. All LAVV reinterventions in patients with right-dominant AVSDs, but low postoperative mortality when compared to single-ventricle palliation supports biventricular repair whenever possible. Leaving the LAVV cleft open during primary AVSD repair might be an independent predictor of poorer overall outcomes and should be avoided when permitted by valvar anatomy. Multicentre cohort studies and registries are needed to determine independent predictive variables associated with outcomes in this patient group.
Supplementary Material
ivae048_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atz AM , Hawkin JA, Lu M, Cohen MS, Colan SD, Jaggers J et al; Pediatric Heart Network Investigators. Surgical management of complete atrioventricular septal defect: associations with surgical technique, age, and trisomy 21. J Thorac Cardiovasc Surg 2011;141:1371–9.21163497 10.1016/j.jtcvs.2010.08.093PMC 3098918 · doi ↗ · pubmed ↗
- 2Xie O , Brizard CP, d’Udekem Y, Galati JC, Kelly A, Yong MS et al Outcomes of repair of complete atrioventricular septal defect in the current era. Eur J Cardiothorac Surg 2014;45:610–7.24057432 10.1093/ejcts/ezt 444 · doi ↗ · pubmed ↗
- 3Minich LL , Atz AM, Colan SD, Sleeper LA, Mital S, Jaggers J et al; Pediatric Heart Network Investigators. Partial and transitional atrioventricular septal defect outcomes. Ann Thorac Surg 2010;89:530–6.20103337 10.1016/j.athoracsur.2009.10.047PMC 2900854 · doi ↗ · pubmed ↗
- 4Ginde S , Lam J, Hill GD, Cohen S, Woods RK, Mitchell ME et al Long-term outcomes after surgical repair of complete atrioventricular septal defect. J Thorac Cardiovasc Surg 2015;150:369–74.26048271 10.1016/j.jtcvs.2015.05.011 · doi ↗ · pubmed ↗
- 5Birim O , van Gameren M, de Jong PL, Witsenburg M, van Osch-Gevers L, Bogers AJ. Outcome after reoperation for atrioventricular septal defect repair. Interact Cardio Vasc Thorac Surg 2009;9:83–7.19372100 10.1510/icvts.2008.195180 · doi ↗ · pubmed ↗
- 6Stulak JM , Burkhart HM, Dearani JA. Reoperations after repair of partial and complete atrioventricular septal defect. World J Pediatr Congenit Heart Surg 2010;1:97–104.23804729 10.1177/2150135110362453 · doi ↗ · pubmed ↗
- 7Tishler B , Gauvreau K, Colan SD, Del Nido P, Nathan M. Technical performance score predicts partial/transitional atrioventricular septal defect outcomes. Ann Thorac Surg 2018;105:1461–8.29269131 10.1016/j.athoracsur.2017.11.043 · doi ↗ · pubmed ↗
- 8Sharma V , Burkhart HM, Schaff HV, Cetta F, Cabalka A, Dearani JA. Management of zone of apposition in parachute left atrioventricular valve in atrioventricular septal defect. Ann Thorac Surg 2013;95:1665–9.23523190 10.1016/j.athoracsur.2013.01.051 · doi ↗ · pubmed ↗