Occult Breast Cancer Presenting as Sternum Pain
Dang Wu, Siyu Guo, Bicheng Zhang, Fengbo Huang, Wei Qian, Fuming Qiu, Qichun Wei, Ting Zhang

TL;DR
A 38-year-old woman with sternum pain was diagnosed with hidden breast cancer through imaging and lab tests, even without visible breast tumors.
Contribution
This case highlights the use of PET-CT and IHC staining to identify occult breast cancer in the absence of visible breast lesions.
Findings
A PET-CT scan showed increased FDG uptake in the sternum and internal mammary node.
Immunohistochemical staining confirmed the diagnosis of occult breast cancer.
Abstract
Bone metastasis has been reported in up to 70% of patients with advanced breast cancer. A total of 55.76% of skeletal metastases in women were derived from breast cancer. However, patients with bone metastasis from an occult primary breast cancer are a rare subset of patients. Here, we present the case of a 38-year-old woman who had sternum pain for 4 months. A whole-body PET-CT scan revealed that the FDG uptake of both the sternum and internal mammary node was significantly increased. The final diagnosis of occult breast cancer was established by immunohistochemical (IHC) staining, which is of great significance for identifying the origin of a metastatic tumor despite no visualized lesions of mammary glands.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
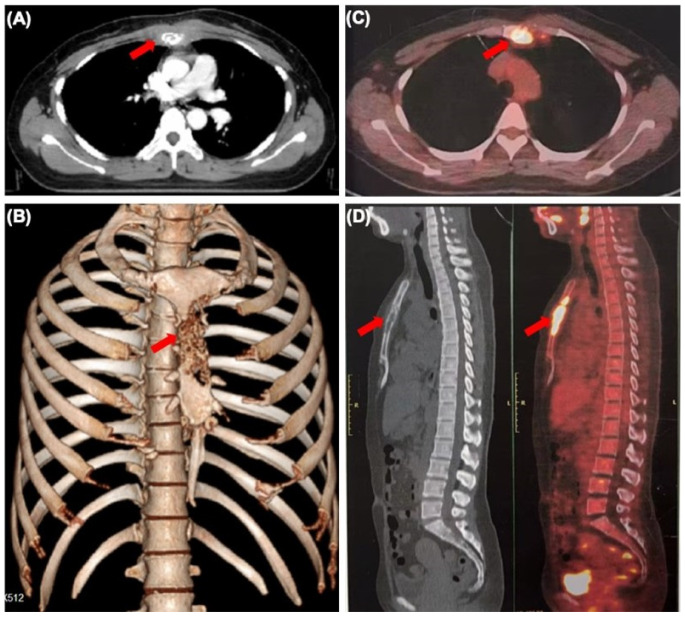 Figure 1
Figure 1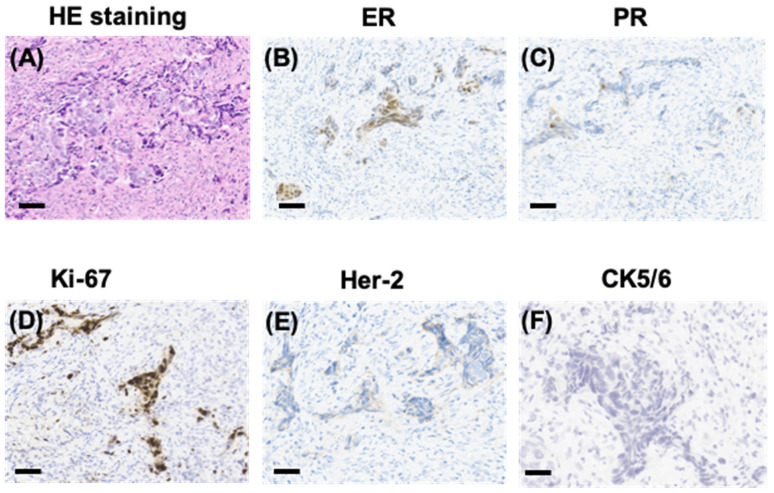 Figure 2
Figure 2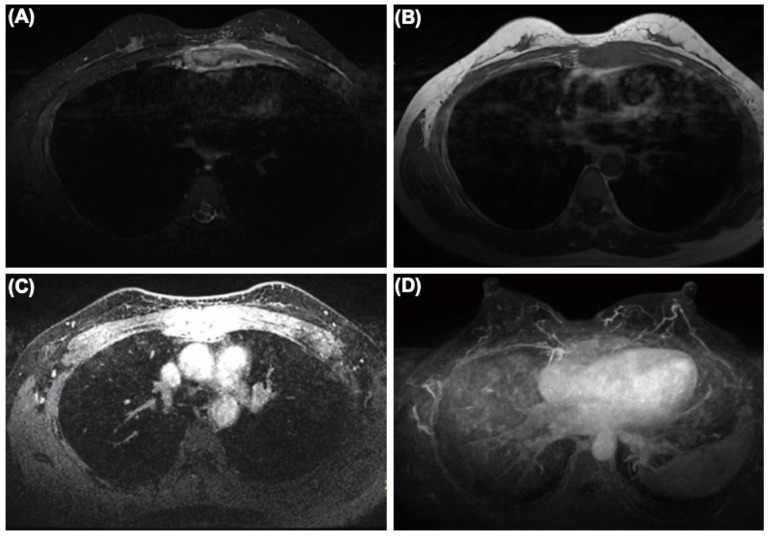 Figure 3
Figure 3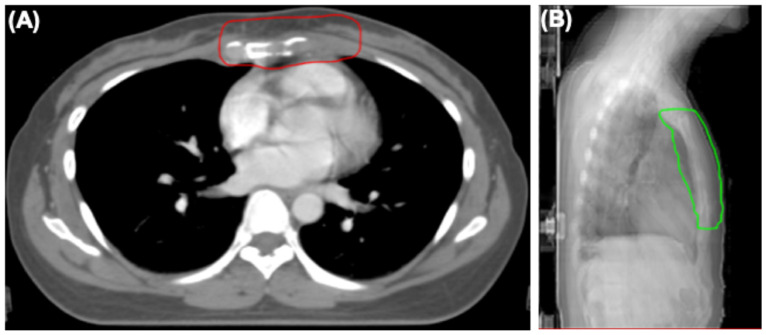 Figure 4
Figure 4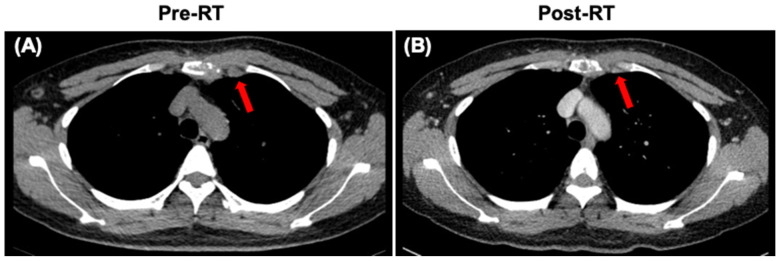 Figure 5
Figure 5- —National Natural Science Foundation of China
- —Immunoradiotherapy Research Fund of Chinese Society of Radiation Oncology
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Management of metastatic bone disease · Oral and Maxillofacial Pathology
Occult breast cancer (OBC) is defined as an undetectable primary breast tumor presenting with clinically recognizable metastatic cancer [1]. It accounts for 0.3–1% of all breast cancers [2], and axillary and cervical lymph node metastasis is the common first clinical presentation [3]. Bone metastasis has been reported in up to 70% of patients with advanced breast cancer [4]. However, patients with bone metastasis from an occult primary breast cancer are a rare subset of patients, especially those with sternum metastasis [5]. Here, we present the case of a 38-year-old woman who had sternum pain for 4 months.
The patient also had an occasional cough. Physical examination revealed normal vital signs and tenderness in the sternum. A plain CT of her chest showed bone destruction at the level of sternal notches 2–4, with soft tissue mass (Figure 1A,B). A subsequent whole-body PET-CT scan revealed that the FDG uptake of the sternum and internal mammary node was significantly increased and other lesions with abnormal FDG uptake were not found (Figure 1C,D). To rule out multiple myeloma, serum-free light chain analysis displayed that serum-free light chain kappa was slightly increased (concentration 23.3 mg/L). Urine protein electrophoresis demonstrated a slight increase in urine protein (0.16 g/24 h). The other results of serum and urine protein electrophoresis and immunofixation, serum β2 microglobulin and serum concentration of common tumor markers were normal. In order to further determine the characteristics of her sternum lesions, sternum biopsy was performed. The histopathology showed that the tumor cells were infiltrated in the form of nests and cords in the bone tissue and skeletal muscle.
IHC staining showed that tumor cells were diffuse positive for cytokeratin and breast-specific markers GATA3 and GCDFP-15. The tumor cells expressed estrogen receptor (ER) at 60% (Figure 2B), progesterone receptor (PR) at 5% (Figure 2C), and androgen receptor (AR) at 80%, a Her-2/neu score of 1+ (Figure 2E) and negative for CK5/6 (Figure 2F). The proliferation index of Ki-67 was up to 80% (Figure 2D). However, the tumor cells were negative for Vimintin, TTF1, PAX8, P40, and CgA. Therefore, the histopathological and IHC evaluation of sternum lesions was consistent with metastatic breast carcinoma, luminal type B, despite no significant abnormality being observed in the breast MRI (Figure 3).
After diagnosis, the patient received systemic therapy with endocrine therapy and a CDK4/6 inhibitor, and local radiotherapy (RT) to sternum and internal mammary node lesions (Figure 4A,B). After local RT, a CT scan was performed to evaluate their therapeutic effect. The sternum and internal mammary node lesions were significantly receded after RT (Figure 5A,B).
Recently, ER+/HER2+ patients have been reported as more likely to have metastases to bone compared to ER−/HER2+ patients in a nationwide autopsy study using artificial intelligence [6]. In this case, the patient was diagnosed as luminal type B of occult breast carcinoma. According to the above study, the molecular type of this patient has a higher possibility of bone metastasis, which might support the finding of the sternum as the first metastatic site. However, another recent study demonstrated that the majority of distant metastases in advanced breast cancer putatively arise from occult regional nodal disease [7]. An interesting feature in this case was that the internal mammary node was also involved in soft tissue mass around sternum lesions, while the FDG uptake of axillary and supraclavicular lymph nodes, with a higher possibility of metastasis, was normal. Therefore, it was difficult to determine whether the sternum was the first metastatic site to invade the internal mammary lymph nodes or vice versa.
Occult breast cancer presenting as sternum pain is an uncommon condition. Any non-specific symptoms, such as bone pain as in the present case, should require high vigilance for occult breast cancer. The role of whole-body PET-CT in assessing possible systemic involvement and the potential primary tumor site is important. IHC is of great significance to identify the origin of a metastatic tumor despite no positive signs in mammary glands.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Halsted W.S. The Results of Radical Operations for the Cure of Carcinoma of the Breast Ann. Surg.19074611910.1097/00000658-190707000-0000117861990 PMC 1414357 · doi ↗ · pubmed ↗
- 2Walker G.V. Smith G.L. Perkins G.H. Oh J.L. Woodward W. Yu T.K. Hunt K.K. Hoffman K. Strom E.A. Buchholz T.A. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis Cancer 20101164000400610.1002/cncr.2519720564117 PMC 4329781 · doi ↗ · pubmed ↗
- 3Toss A. Moscetti L. Cascinu S. Occult breast cancer: The uncommon presentation of a common disease Chin. Clin. Oncol.20198 S 1010.21037/cco.2019.01.0630823842 · doi ↗ · pubmed ↗
- 4Buijs J.T. van der Pluijm G. Osteotropic cancers: From primary tumor to bone Cancer Lett.200927317719310.1016/j.canlet.2008.05.04418632203 · doi ↗ · pubmed ↗
- 5Carsote M. Terzea D. Vasilescu F. Cucu A.P. Ciuche A. Nistor C. Sternum Metastases: From Case-Identifying Strategy to Multidisciplinary Management Diagnostics 202313269810.3390/diagnostics 1316269837627957 PMC 10453928 · doi ↗ · pubmed ↗
- 6Kazemzadeh F. Snoek J.A.A. Voorham Q.J. van Oijen M.G.H. Hugen N. Nagtegaal I.D. Association of metastatic pattern in breast cancer with tumor and patient-specific factors: A nationwide autopsy study using artificial intelligence Breast Cancer 20243126327110.1007/s 12282-023-01534-638133738 · doi ↗ · pubmed ↗
- 7Bitencourt A. Rossi Saccarelli C. Morris E.A. Flynn J. Zhang Z. Khan A. Gillespie E. Cahlon O. Mueller B. Cuaron J.J. Regional Lymph Node Involvement Among Patients With De Novo Metastatic Breast Cancer JAMA Netw. Open 20203 e 201879010.1001/jamanetworkopen.2020.1879033034638 PMC 7547365 · doi ↗ · pubmed ↗