Dexamethasone in Patients with Glioblastoma: A Systematic Review and Meta-Analysis
Pierre Scheffler, Christian Fung, Shahan Momjian, Dominik Koessinger, Levin Häni, Nicolas Neidert, Jakob Straehle, Florian Volz, Oliver Schnell, Jürgen Beck, Amir El Rahal

TL;DR
Dexamethasone, a steroid used to treat symptoms in glioblastoma patients, may reduce survival and should be used cautiously.
Contribution
This study provides the first meta-analysis showing that dexamethasone use correlates with worse survival in glioblastoma patients.
Findings
Higher dexamethasone doses are linked to reduced overall and progression-free survival in glioblastoma patients.
The negative effect on survival remains even after adjusting for clinical status.
Dexamethasone should be restricted to selected symptomatic patients due to its potential detrimental impact.
Abstract
Dexamethasone is frequently administered in brain tumor patients for symptomatic relief. However, an increasing number of publications suggests that dexamethasone may lead to worse outcome in patients with glioblastoma. Our study reviews all the published evidence and aggregates the available data in a meta-analysis. We found that dexamethasone indeed significantly reduces overall and progression-free survival in glioblastoma patients, even when accounting for clinical status. Given the potential detrimental association of dexamethasone use on overall survival, its administration to glioblastoma patients should be approached with caution. Objective: Glioblastomas are the most common primary central nervous system (CNS) tumors. Although modern management strategies have modestly improved overall survival, the prognosis remains dismal, with treatment side effects often impinging on the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
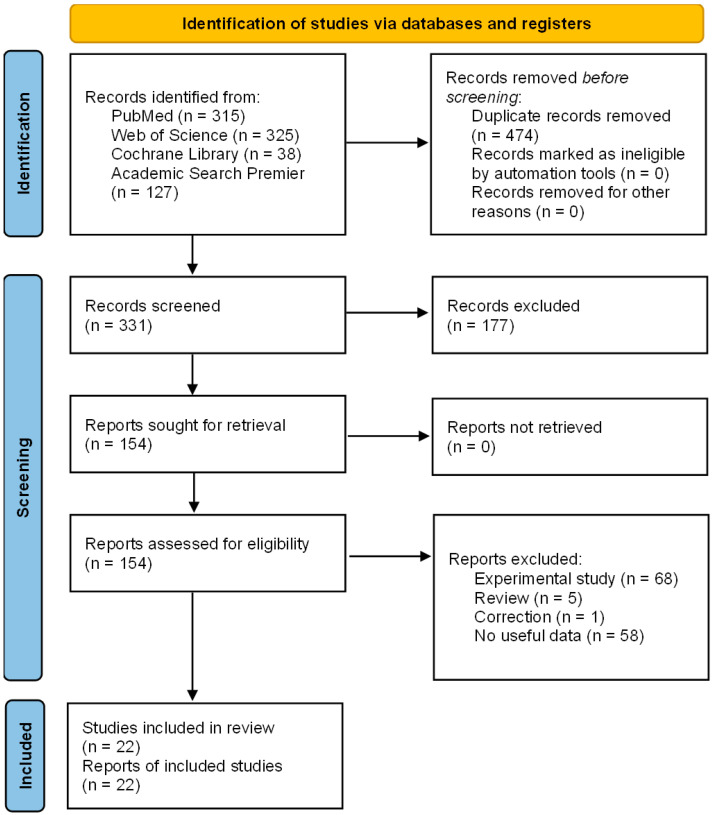 Figure 1
Figure 1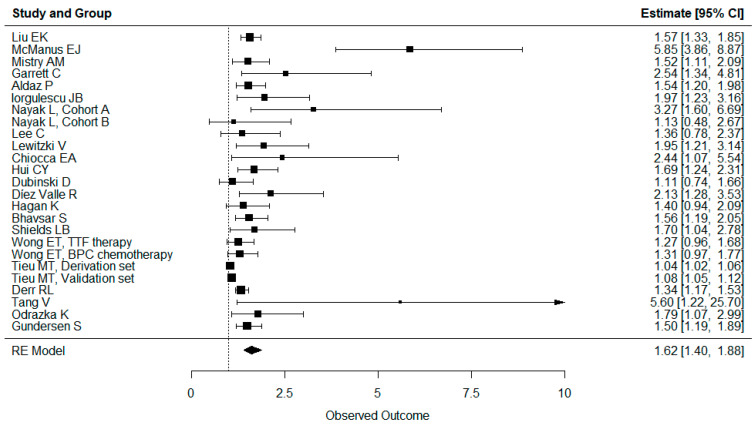 Figure 2
Figure 2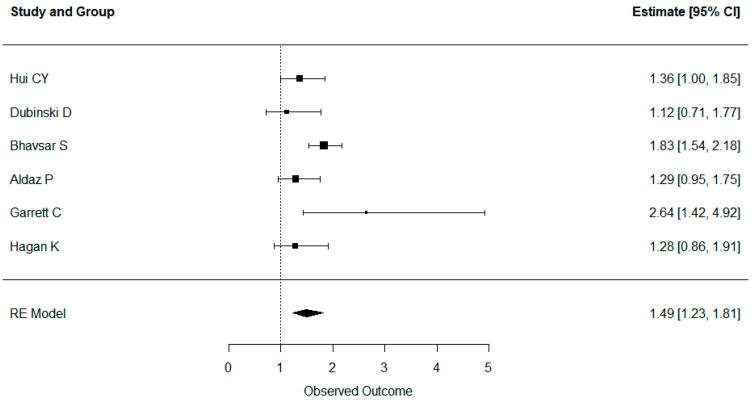 Figure 3
Figure 3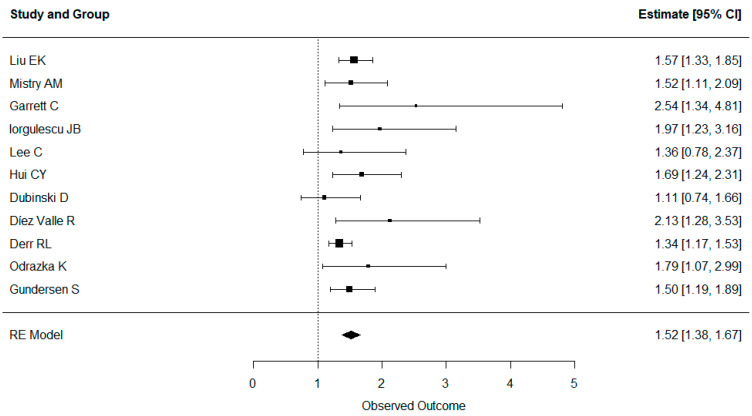 Figure 4
Figure 4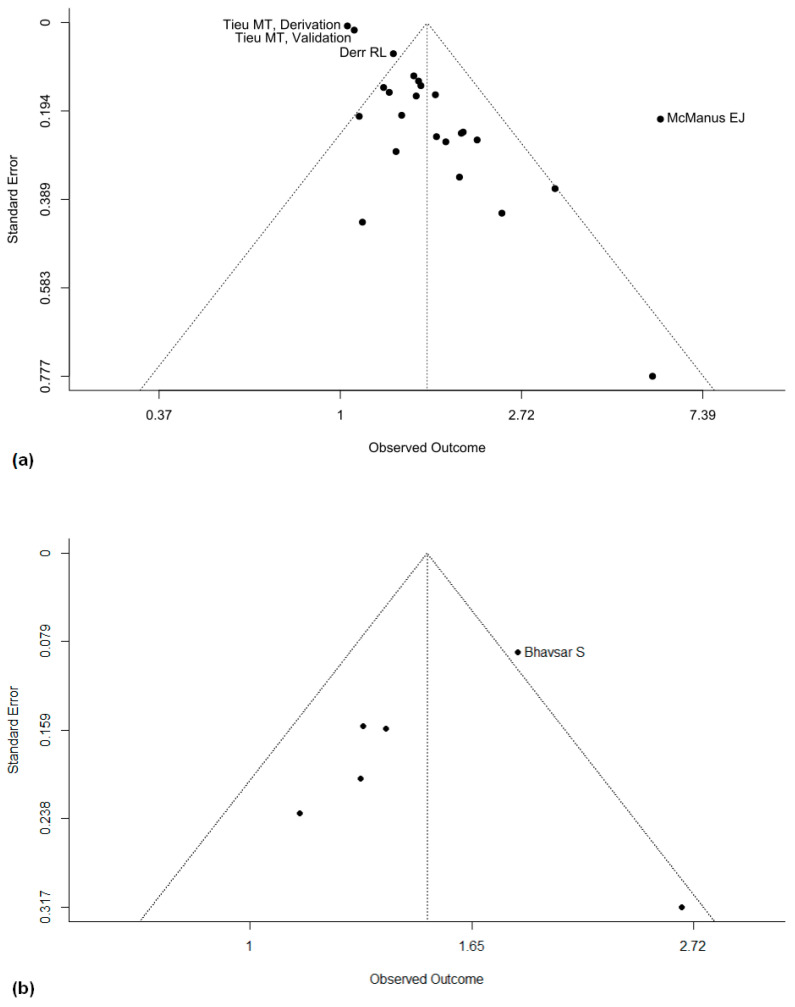 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLinguistics, Language Diversity, and Identity
1. Introduction
Glioblastoma is the most common primary malignant tumor of the central nervous system (CNS), accounting for 48.6% of tumors, with an estimated incidence of 3.23 per 100,000 persons per year [1]. According to the current WHO classification, glioblastomas are among the most aggressive primary CNS tumors [2]. However, modern treatment strategies have improved the prognosis, with a clinical course often impinged by treatment side effects and cognitive decline. Standard treatment of glioblastomas consists of maximum safe resection followed by adjuvant chemotherapy and radiotherapy [3]. As a result, the survival rate for glioblastoma patients improved from 3.3 months to a median of 15 months in the past 30 years [4]. Most glioblastomas show rapid growth, with diffuse infiltration into healthy CNS tissue [5]. This growth is frequently associated with perifocal oedema. Although, due to necrosis, neurological function within the center of the tumor is usually irreversibly lost, neurological activity within the surrounding edematous tissue can be temporarily alleviated by reducing oedema.
Dexamethasone is a synthetic glucocorticoid that was first described in 1958 [6]. Dexamethasone is known for its high glucocorticoid potency, weak mineralocorticoid effects, and long biological half-life. The potent effects of dexamethasone administration on symptoms in brain tumor patients were first described by Galicich et al. [7,8]. Since then, dexamethasone has been widely used in patients with intracranial tumors. Steroids, like dexamethasone, are believed to mitigate the symptoms experienced by intracranial tumor patients owing to their anti-inflammatory properties. These properties facilitate the reduction of perifocal edema and potentially enhance the integrity of the blood–brain barrier. They achieve this through various mechanisms, including acting on the endothelium and exerting a direct influence on the astrocytes surrounding the vessels, consequently diminishing vasogenic perifocal edema. Administration of glucocorticoids may also improve general neurological function by reducing intracranial pressure [9]. Palombi et al. showed that administration of dexamethasone in glioblastoma patients leads to symptomatic improvements, such as a significant reduction in headaches, vomiting, seizures, and focal neurological deficits [10]. Villani et al. demonstrated a 20-point improvement in the Karnofsky Performance Score for 43.8% of patients with grade II–IV gliomas receiving dexamethasone [11].
Nonetheless, glucocorticoids are a class of drugs that affect various organ systems with unwanted side effects. Short-term glucocorticoid administration is generally deemed safe in most patients, even when given in substantial doses, such as in patients with acute worsening of multiple sclerosis [12]. However, long-term administration of high doses of glucocorticoids causes Cushing’s syndrome, which is associated with elevated cardiovascular risk, osteoporosis, and an elevated infection risk due to immunosuppression [13,14].
Although dexamethasone is widely used in patients with cerebral edema, it may not always be beneficial. Administration of dexamethasone was widespread in patients with traumatic brain injury until studies showed that its use was detrimental to outcomes [15]. More specifically, for glioblastoma patients, the use of dexamethasone has raised concerns. Recent findings suggest a potential negative impact on both PFS and OS, pointing towards a correlation with poorer long-term prognoses, making the routine use of this drug in this patient group a subject of careful consideration [16,17,18,19]. As a result, we decided to compile the currently available evidence on the impact of dexamethasone use in glioblastoma patients in a quantitative review.
2. Materials and Methods
2.1. Search Strategy
We performed a systematic review and meta-analysis according to the PRISMA-P guidelines. This review was not prospectively registered. In our meta-analysis, we included studies reporting on the objective outcomes of patients with glioblastomas taking dexamethasone, specifically their overall survival (OS) and progression-free survival (PFS). For our literature review, we searched the following databases: PubMed, Web of Science, Cochrane Library, and Academic Search Premier. All the results from all the databases were included up to 1 September 2023. We searched for all publications that included the keywords “dexamethasone” and “glioblastoma”.
2.2. Screening
Two independent reviewers (PS and AER) screened all the abstracts. For the qualitative discussion of the current evidence, we filtered all the publications that reported on the effects of dexamethasone in glioblastoma patients, in glioblastoma animal models, or on glioblastoma cells. For the quantitative part of the review, we selected all the publications that reported on the overall or progression-free survival in patient groups with higher and lower dexamethasone intake and those that provided data that could be used to extract hazard ratios. For studies reporting on the same patient population, the most informative study (either the most recent or the one with the largest population) was selected.
2.3. Data Collection
Data were collected from published reports by one reviewer (PS) and subsequently confirmed by a second reviewer (AER). Data on OS and PFS were extracted for all available studies. Data from the multivariable analysis were extracted from studies that provided both univariable and multivariable analyses. We also extracted all the variables that were part of the multivariable analysis. For Hagan et al. [20], we extracted the data from the model adjusted for preoperative blood glucose. The bias of individual studies was assessed using ROBINS-I [21] by two independent reviewers (PS and AER).
2.4. Analysis
We analyzed the OS and PFS based on the reported hazard ratios (HR) and confidence intervals (CI). Most of the publications reported the effect sizes and variances of the OS and PFS as hazard ratios with a corresponding confidence interval. In one case, the confidence interval was calculated based on a reported standard error. If the publications only reported Kaplan Meier plots, the HR and CI were calculated based on data extracted using Engauge Digitizer. Statistical analysis was performed using the R programming language and its metafor package. A random effects model was used to calculate the average effect size across studies. Separate meta-analyses were performed for all studies reporting OS, all studies reporting PFS, and all studies reporting OS that adjusted for clinical status (by group matching or considering the Karnofsky performance score or ECOG performance status in their multivariable analysis), respectively. Reporting bias was assessed using funnel plots. Plots were created using the funnel function from R’s metafor package. Certainty was assessed according to the GRADE working group’s criteria [22].
3. Results
3.1. Study Selection
Our literature search initially revealed 318 studies quantifying overall and progression-free survival. After screening all the abstracts, 153 studies were retrieved for full review. After the exclusion of ineligible studies, 22 studies were identified for the quantitative review [17,18,20,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] (Figure 1).
3.2. Study Characteristics
All the studies selected for quantitative review were retrospective analyses of glioblastoma patients receiving different doses of dexamethasone. The characteristics and the quality assessment of these studies are shown in Table 1.
3.3. Risk of Bias in Studies
The risk of bias was determined to be either moderate or serious for all the included studies Table 1. This is mainly because all the included studies were retrospective, with only about half of them adjusting the clinical performance via multivariable analyses or matching despite clinical status being considered a significant confounder for OS and PFS.
3.4. Results for Individual Studies
The hazard ratios and confidence intervals for all the studies are reported in Figure 2 and Figure 3. All the studies reported either no effect or a significantly negative effect of dexamethasone intake on both overall and progression-free survival. No studies showed a positive effect of dexamethasone intake on OS or PFS. Mistry et al. also reported that higher doses of dexamethasone had a worse effect than medium or low doses [36].
3.5. Results of Syntheses
The results for aggregate OS and PFS are shown in Figure 2 and Figure 3. Administration of dexamethasone had a possible significant negative impact on both OS (hazard ratio 1.62, confidence interval 1.40–1.88) and PFS (HR 1.49, CI 1.23–1.81) in glioblastoma patients. In addition, overall survival remained significantly worse, even when the studies corrected for clinical status.
As we aimed to interrogate whether clinical status is a major confounder for survival in glioblastoma patients receiving dexamethasone, we also performed an aggregate analysis for overall survival, including only studies accounting for either the Karnofsky performance score or ECOG through matching or multivariable analysis. The results are shown in Figure 4. Even after accounting for clinical performance, dexamethasone intake had a negative impact on overall survival (HR 1.52, CI 1.38–1.67).
3.6. Reporting Biases
To assess the risk of bias in our study selection, we compared the study results using a funnel plot for OS and PFS (Figure 5a,b). Despite the funnel plots showing some outliers, no systematic bias could be visually perceived in the plots.
3.7. Certainty of Evidence
Due to the retrospective observational nature and limited patient population of all the included studies, the overall certainty of evidence for the effect of dexamethasone on OS and PFS in patients with glioblastomas according to the GRADE criteria is low.
4. Discussion
Studies have shown that dexamethasone reduces perifocal edema in glioblastoma patients [7] and dexamethasone significantly reduces symptoms in glioblastoma patients [10,11]. Despite the widespread use of dexamethasone in glioblastoma patients, the association of dexamethasone with overall and progression-free survival is overwhelmingly negative. There are several potential explanations for this effect. First and foremost, glucocorticoids may interfere with any immunomodulatory treatments [31,41], as well as radiation and chemotherapy [18,23,29,32,42]. In addition, dexamethasone and other glucocorticoids are immunosuppressors. As a result, the administration of dexamethasone can lead to increased infectious complications [14,43].
Glucocorticoids also lead to impaired glucose tolerance. Hyperglycemia has been shown to be an independent risk factor for overall and progression-free survival in glioblastoma patients [17,25]. Although the exact mechanisms still remain to be elucidated, one possible explanation is the Warburg effect, which proposes that tumors meet their energy needs mainly through anaerobic glycolysis [44]. In vitro, unlike human astrocytes, glioblastoma cells were shown to undergo apoptosis upon glucose withdrawal [45]. Other detrimental effects of hyperglycemia, such as an increased risk of infection, may also contribute to its negative impact on survival [46].
Preclinical studies have investigated possible mechanisms through which dexamethasone might impair survival in glioblastoma patients. Experimental models have shown that dexamethasone increases invasiveness, tumor proliferation, and angiogenesis [47]. Dexamethasone also reduces temozolomide-mediated apoptosis in human glioblastoma cells [48,49,50], possibly through O6-methylguanine-DNA methyltransferase (MGMT) upregulation, which results in an increased temozolomide resistance [51,52]. Interestingly, some preclinical studies have found that dexamethasone can also reduce glioblastoma invasiveness through various mechanisms [53,54,55,56,57].
While evidence is limited, studies indicate that the overall dose of dexamethasone applied matters. Mistry et al. showed that the higher the dose of dexamethasone received, the worse the survival, with a continuously increasing hazard ratio at cumulative doses between 30 and 512 mg within the first 3 postoperative weeks after glioblastoma resection. Patients with a cumulative postoperative dose below 75 mg had a median survival of 441 days, whereas patients who received more than 300 mg had a median survival of 183 days [36]. This dose-dependent effect may also explain the outliers we see in the funnel plots of our meta-analysis. The included studies use various cutoffs between groups with high and low dexamethasone dosing, resulting in a variety of hazard ratios even in studies with a large patient population. We aimed to account for this by using a random effects model for our analysis. Our model accounts for the large variations in dexamethasone dosing that occur in everyday clinical practice. Therefore, the aggregate hazard ratio is harder to interpret but still supports the conclusion that the administration of dexamethasone might reduce survival.
Our findings may also be affected by several different types of bias. The negative effect of dexamethasone that we show could be exacerbated by publication bias. Although the funnel plot analysis shows no significant skew, its interpretability is reduced due to the significant differences between individual study protocols. Therefore, the contribution of publication bias to our results cannot be definitely excluded. Our analysis may also be affected by confounding variables. One possible explanation for the detrimental effect of dexamethasone is that patients with worse clinical statuses and more advanced diseases with worse outcomes will receive higher doses of dexamethasone. Most guidelines suggest only administering dexamethasone in symptomatic patients and adjusting the dose according to the patient’s symptoms, and a stable or increasing corticosteroid dose is necessary for defining progressive disease in gliomas according to RANO criteria in many cases [58]. Ideally, a prospective randomized trial could determine the effect of dexamethasone on survival in glioblastoma patients. One such review has already been launched and should be completed by 2026 under the “Restrictive Use of Dexamethasone in Glioblastoma (RESDEX)” project. However, retrospective studies have already tried to account for symptom differences through multivariable analyses. Our aggregate analysis of these studies showed that dexamethasone still negatively impacts survival, independent of patient’s symptoms. Mistry et al. also used matched control groups for the Karnofsky performance score and other potential confounders such as tumor size [36]. Despite matched groups, the administration of dexamethasone still significantly decreased OS and PFS.
Given the potential detrimental association of dexamethasone use on survival, careful consideration must be given before administering dexamethasone to glioblastoma patients. As the only proven benefit of dexamethasone is the reduction of symptoms, we believe that dexamethasone should not be administered in asymptomatic patients or with a restrictive regimen. Even in symptomatic patients, alternative specific treatments may be similarly effective without affecting survival. Headaches and nausea may be treated with analgesics and antiemetics. Several non-steroidal drugs and drug combinations are also being investigated as possible edema-reducing, glucocorticoid-sparing agents, such as bevacizumab [59] and a combination of spironolactone, ecallantide, and clotrimazole [60]. However, one should consider that the use of drugs like bevacizumab is constrained due to potential complications related to wound healing. Specifically, its administration must be discontinued at least 28 days pre- and post-surgery, which can limit its daily use [61,62]. As for the postoperative period, the current high costs associated with bevacizumab may render it limited for routine use in managing symptomatic patients. However, this might change in the future.
5. Limitations
As a meta-analysis, our study is limited by the quality of the underlying studies. All the included studies were retrospective. As a result, there was a significant potential for selection bias, confounding variables, and other sources of bias that may have affected the validity of the results. Additionally, the studies included in the analysis showed considerable heterogeneity in their methods used for measuring dexamethasone exposure and their cutoffs for defining high and low dexamethasone doses, which reduces the interpretability of our results and the effect sizes in our analysis. Despite these limitations, until the publication of prospective trials, a systematic review of these publications represents the highest quality of evidence currently available concerning the use of dexamethasone in glioblastoma patients.
6. Conclusions
Given the potential detrimental association of dexamethasone use on overall survival, its administration to glioblastoma patients should be approached with caution. As the only proven benefit of dexamethasone is the reduction of symptoms, we believe that dexamethasone should not be administered in asymptomatic patients or with a restrictive regimen and only after carefully weighing the expected symptomatic improvement against the worsened prognosis. Nevertheless, this recommendation may be subject to change as future prospective studies emerge.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ostrom Q.T. Cioffi G. Gittleman H. Patil N. Waite K. Kruchko C. Barnholtz-Sloan J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012–2016 Neuro-Oncology 201921(Suppl. 5)v 1v 10010.1093/neuonc/noz 15031675094 PMC 6823730 · doi ↗ · pubmed ↗
- 2Louis D.N. Perry A. Wesseling P. Brat D.J. Cree I.A. Figarella-Branger D. Hawkins C. Ng H.K. Pfister S.M. Reifenberger G. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary Neuro-Oncology 2021231231125110.1093/neuonc/noab 10634185076 PMC 8328013 · doi ↗ · pubmed ↗
- 3Stupp R. Mason W.P. van den Bent M.J. Weller M. Fisher B. Taphoorn M.J.B. Belanger K. Brandes A.A. Marosi C. Bogdahn U. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma N. Engl. J. Med.200535298799610.1056/NEJ Moa 04333015758009 · doi ↗ · pubmed ↗
- 4Delgado-López P.D. Corrales-García E.M. Survival in glioblastoma: A review on the impact of treatment modalities Clin. Transl. Oncol.2016181062107110.1007/s 12094-016-1497-x 26960561 · doi ↗ · pubmed ↗
- 5Xie Q. Mittal S. Berens M.E. Targeting adaptive glioblastoma: An overview of proliferation and invasion Neuro-Oncology 2014161575158410.1093/neuonc/nou 14725082799 PMC 4232088 · doi ↗ · pubmed ↗
- 6Glen A.E. Johnston D.B.R. Fried J. Spooncer W.W. Hoff D.R. Sarett L.H. 16-Methylated Steroids. I. 16α-Methylated Analogs of Cortisone, a New Group of Anti-Inflammatory Steroids J. Am. Chem. Soc.19588031603161
- 7Galicich J.H. French L.A. Melby J.C. Use of dexamethasone in treatment of cerebral edema associated with brain tumors J. Lancet 196181465313703072 · pubmed ↗
- 8Mc Clelland S.3rd Long D.M. Genesis of the Use of Corticosteroids in the Treatment and Prevention of Brain Edema Neurosurgery 200862965967965–967; discussion 67–6810.1227/01.neu.0000318183.25783.7718496203 · doi ↗ · pubmed ↗