Multiple Myeloma Presenting With Bronchopneumonia: A Case Report
Ashwin Karnan, Babaji Ghewade, Vivek D Alone, Anjana Ledwani

TL;DR
This case report highlights a rare presentation of multiple myeloma as bronchopneumonia, emphasizing the importance of recognizing unusual symptoms for timely diagnosis.
Contribution
The novelty lies in presenting a case of multiple myeloma with an atypical initial symptom of bronchopneumonia.
Findings
Multiple myeloma can present with bronchopneumonia, leading to delayed diagnosis.
Awareness of varied presentations is crucial for early detection and treatment.
Recent advances in treatment can achieve remission despite the disease being incurable.
Abstract
Multiple myeloma is a disease of the plasma cells of the bone marrow, resulting in the proliferation and release of the monoclonal protein, which further causes end-organ damage. We report an unusual presentation of multiple myeloma, thereby insisting on the need for the treating physician to be aware of the various presentations that can be encountered in regular practice. It is often difficult to diagnose, and the diagnosis is usually made at a late stage of the disease. Even though uncurable, with recent advances, a proper regimen, newer chemotherapeutic agents, and stem cell transplantation, the disease can be brought into remission.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1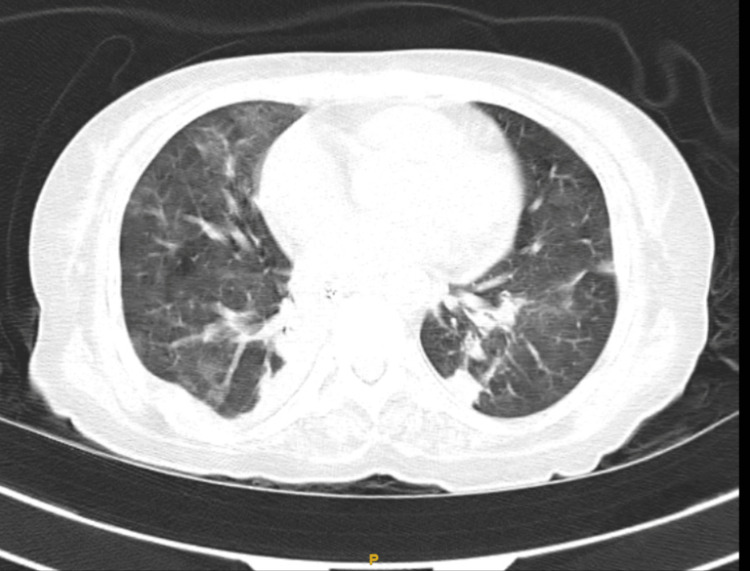 Figure 2
Figure 2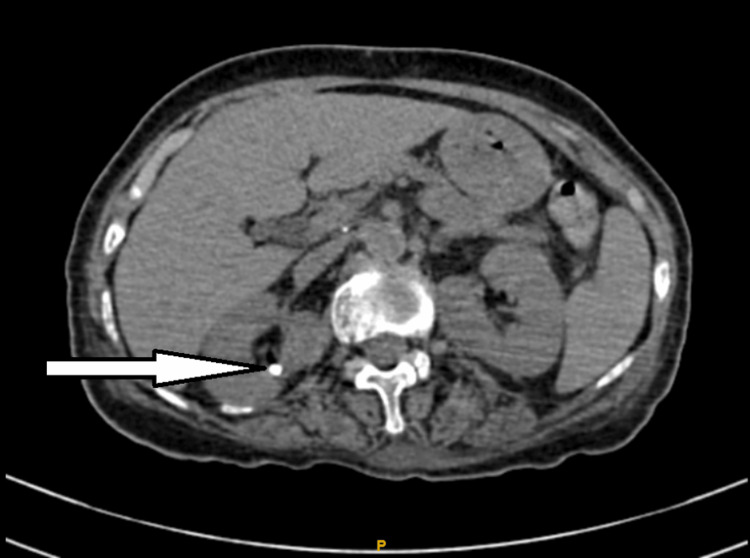 Figure 3
Figure 3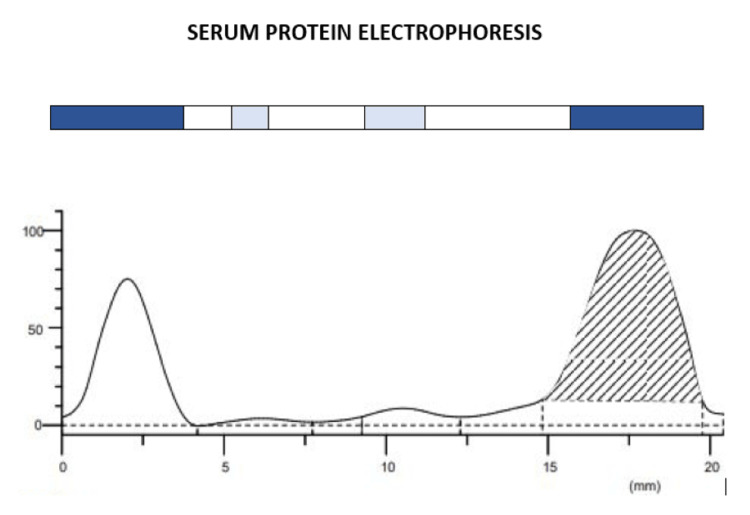 Figure 4
Figure 4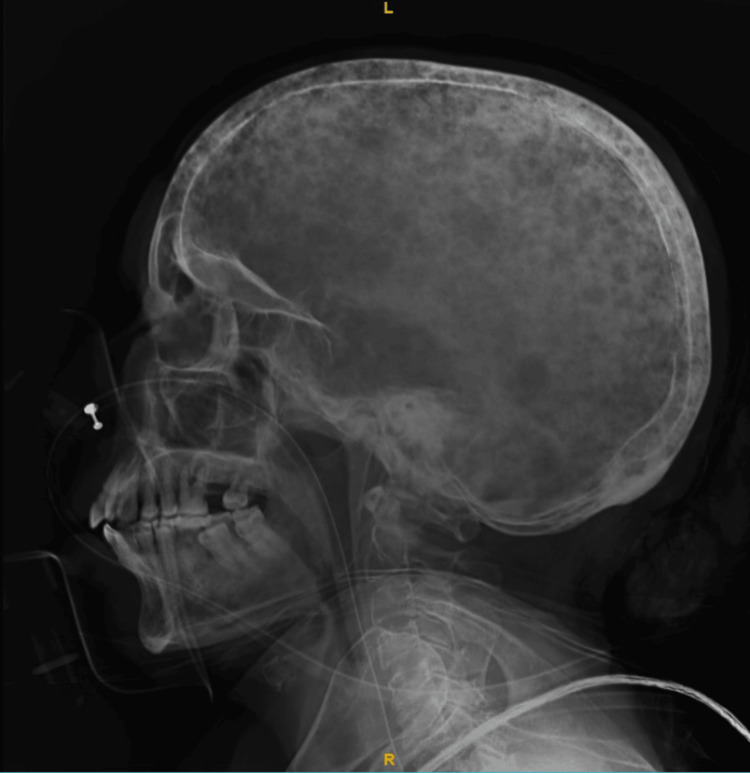 Figure 5
Figure 5| Investigations | Values | Reference range |
| Hb | 9.2 g/dL | 13-17 g/dL |
| MCHC | 33.5 g/dL | 30-35 g/dL |
| MCV | 85.6 fl | 80-100 fl |
| MCH | 28.7 Pico-gm | 27-32 Pico-gm |
| Total RBC count | 3.2 million/mm3 | 4.5-6 million/mm3 |
| Total WBC count | 13,400/mm3 | 4,000-11,000/mm3 |
| Total platelet count | 1.12 lacs/mm3 | 1.50-4.10 lacs/mm3 |
| HCT | 27.40% | Male: 41-50%; female: 36-44% |
| Investigations | Values | Reference range |
| ALP | 116 U/L | 38-126 U/L |
| ALT (SGPT) | 22 U/L | Male: <50 U/L; female: <35 U/L |
| AST (SGOT) | 54 U/L | 15-46 U/L |
| Total protein | 11.0 g/dL | 6.3-8.2 g/dL |
| Albumin | 3.0 g/dL | 3.5-5.0 g/dL |
| Globulin | 8.0 g/dL | 2.3-3.5 g/dL |
| Investigations | Values | Reference range |
| Urea | 90 mg/dL | Male: 9-20 mg/dL; female: 7-17 mg/dL |
| Creatinine | 2.0 mg/dL | Male: 0.66-1.25 mg/dL; female: 0.52-1.04 mg/dL |
| Calcium | 14.0 mg/dL | 8.1-10 mg/dL |
| Index | Band | Percentage | Concentration (g/dL) | Range (g/dL) |
| 1 | Albumin | 28.34% | 3.32 L | 3.50-5.00 |
| 2 | Alpha 1 | 1.45% | 0.17 | 0.10-0.40 |
| 3 | Alpha 2 | 0.73% | 0.08 L | 0.5-1.10 |
| 4 | Beta | 3.86% | 0.45 L | 0.60-1.30 |
| 5 | Gamma | 65.62% | 7.68 H | 0.60-1.60 |
| Total 11.70 | ||||
| 5M | Gamma | 49.06% | 5.74 H | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Peptidase Inhibition and Analysis · Protein Degradation and Inhibitors
Introduction
Multiple myeloma is a cancer of the plasma cells of the bone marrow, resulting in the proliferation and release of the myeloma protein, which further causes end-organ damage. It accounts for 1.8% of all cancer cases per year in the US, with an incidence of 5.8/1 lakh population accounting for 20,000 new cases per year and an incidence of 0.7/1 lakh population accounting for 7,000 new cases per year in India [1]. The average age at diagnosis is 70 years and is slightly more common in males, with a male-to-female ratio of 1.4:1. Symptoms include bone pain, generalized tiredness, recurrent infections, easy bruising and bleeding, weight loss, and headaches. The prognosis depends on the stage of the disease. Diagnosis is usually made at the late stage of the disease. The five-year survival rate is around 59.8% [2], and survival rates have improved with the introduction of newer chemotherapeutic drugs and stem cell transplantation. Almost all cases of multiple myeloma go into repeated remission and relapse. Supportive treatment aimed at the correction of hypercalcemia, anemia, and pain also plays an important role.
Case presentation
A 60-year-old female presented with complaints of breathing difficulty, dry cough, and chest pain for the preceding two days. The patient had been symptom-free until that point. The dry cough had an insidious onset and progressive nature, without positional variation. Breathlessness initially occurred on exertion, progressing to rest, and chest pain was diffuse and dull-aching with no radiation. The patient reported no similar past illnesses, no significant medical or family history, no history of addictions, and maintained a vegetarian diet.
Upon examination, the patient was conscious and oriented, with a height of 152 cm, a weight of 40 kg, and a BMI of 17.78 (underweight). The pulse rate was 120 beats/minute, the respiratory rate was 34 breaths/minute, and the blood pressure was 110/70 mm Hg (measured in the right upper arm in a sitting posture). Oxygen saturation was 75% at room air, improving to 96% with noninvasive ventilation (NIV) support (FiO2 100%, PEEP 5 cmH2O). In the respiratory system, bilateral crepitations were noted throughout the auscultation. The cardiovascular system exhibited audible S1 and S2 with no murmurs. There were no focal neurological deficits; abdominal pain and tenderness were absent, and lumbar region tenderness was noted.
Arterial blood gas suggested type I respiratory failure. The 12-lead ECG was within normal limits. The chest X-ray showed bilateral inhomogeneous shadows (Figure 1).
Chest X-ray showing bilateral bronchopneumonia
High-resolution computed tomography of the thorax showed bilateral patchy consolidation with cardiomegaly (Figure 2).
HRCT thorax showing bilateral patchy consolidation with cardiomegaly and bilateral diffuse ground glass opacity suggestive of pulmonary edemaHRCT, high-resolution computed tomography
A computed tomography of the abdomen and pelvis was performed, which showed hyperdense calculi in the right kidney (Figure 3).
CT scan showing degenerative changes in the spine and hyperdense calculi in the right kidneyCT, computed tomography
The complete blood count of the patient showed normocytic normochromic anemia (Table 1).
The liver function test of the patient showed elevated globulin levels with low serum albumin (Table 2).
The renal function test showed raised urea and creatinine with raised serum calcium (Table 3).
Serum protein electrophoresis showed a spike in the gamma M band, and a serum free light chain assay showed raised levels of free lambda light chain (Figure 4, Table 4).
Serum protein electrophoresis showing a spike in the gamma globulin region with an M band suggestive of multiple myeloma
An X-ray of the skull showed lytic lesions (Figure 5).
Lateral view of the skull showing multiple punched-out lytic lesions referred to as raindrop skull
The bone marrow aspirate showed normocytic normochromic anemia with Rouleaux formation and numerous immature plasma cells with irregular nuclei.
The patient was treated with intravenous antibiotics, intravenous fluids, non-NIV support, and chest physiotherapy. She was then shifted to the oncology department for chemotherapy.
Discussion
Multiple myeloma is characterized by the proliferation of cancerous plasma cells that grow out of control, produce an abnormal antibody called M protein, and cause end-organ damage. The plasma cells activate osteoclastic activity, causing bone destruction (pain, fracture, and immobility). It accounts for 1.8% of cancer cases in the US and 1.1% of all cancer deaths. Risk factors include advancing age, male sex, which is twice as common among African Americans, and people with a family history. Genetic alteration in the form of chromosomal deletion (del(17p)) and translocation (t(14;16), t(11;14), t(4;14)) is known to initiate disease and cause progression. These genetic alterations alter signaling pathways, which lead to plasma cell growth and proliferation. These plasma cells interact with the microenvironment of the bone marrow and induce osteoclastic activity [3]. Clinical manifestations include tiredness, excessive thirst, bone pain, easy bruising, recurrent infections, bleeding manifestations, and weight loss [4]. Diagnostic criteria include (1) clonal bone marrow plasma cells >10% or biopsy-proven extramedullary plasmacytoma, along with (2) evidence of end-organ damage due to plasma cell proliferative disorder such as hypercalcemia >11 mg/dL, renal failure creatinine >2 mg/dL, anemia (hemoglobin <10 g/dL), or one or more osteolytic lesions on skeletal radiography or clonal bone marrow >60% or uninvolved serum free light chain ratio >100 [5].
The five-year survival rate of multiple myeloma is around 57%, and the prognosis has increased due to therapeutic advances [6]. Multiple myeloma should be classified into high- or standard-risk groups, and proper treatment regimens should be initiated in such a way that future treatment is unaffected. If the patient is fit for transplant, the patient is treated with three to four cycles of monoclonal antibody/immunomodulator with a low-dose steroid; if a good response is noted, the patient can avoid maintenance therapy [7]. A trial involving bortezomib, dexamethasone, and lenalidomide showed a good response rate and survival rate, making it the initial therapy for newly diagnosed cases [1]. Along with chemotherapy, supportive treatment to correct hypercalcemia, anemia, and bone pain is important, which includes regular treatment with bisphosphonates [8]. Despite treatment options, multiple myeloma is known to have multiple remissions and relapses. While treating a case of relapse, time of relapse, aggressiveness, performance score, and response to earlier treatment are taken into account [9].
Conclusions
Multiple myeloma is a rare, aggressive neoplastic disease that is on the rise in developing countries. Although incidence has risen, survival rates have increased due to newer drugs and stem cell transplant options. Bronchopneumonia in an immunocompromised patient is a complex infection with high mortality and morbidity. It may be further complicated by sepsis, multidrug resistance, pneumothorax, drug side effects, and respiratory distress. Since multiple myeloma is a complex disease, patient education and counseling are very important. As there is multisystem involvement, a multidisciplinary approach and a lookout for unusual presentations should always be kept in mind. In addition to chemotherapy, pain management, physiotherapy, diet, and nutrition should be given equal importance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology, staging, and management of multiple myeloma Med Sci (Basel) Padala SA Barsouk A Barsouk A 3920213349835610.3390/medsci 9010003 PMC 7838784 · doi ↗ · pubmed ↗
- 2Cancer stat facts: myeloma 2 2024 https://seer.cancer.gov/statfacts/html/mulmy.html
- 3Multiple myeloma Stat Pearls [Internet] Albagoush SA Shumway C Azevedo AM Treasure Island (FL)Stat Pearls Publishing 2024 https://pubmed.ncbi.nlm.nih.gov/30521185/30521185 · pubmed ↗
- 4Multiple myeloma: clinical features and indications for therapy Best Pract Res Clin Haematol Dispenzieri A Kyle RA 5535681820051602673710.1016/j.beha.2005.01.008 · doi ↗ · pubmed ↗
- 5Multiple myeloma: 2022 update on diagnosis, risk stratification, and management Am J Hematol Rajkumar SV 108611079720223556006310.1002/ajh.26590 PMC 9387011 · doi ↗ · pubmed ↗
- 6Time trends in survival and causes of death in multiple myeloma: a population-based study from Germany BMC Cancer Eisfeld C Kajüter H Möller L Wellmann I Shumilov E Stang A 3172320233702481310.1186/s 12885-023-10787-5PMC 10080943 · doi ↗ · pubmed ↗
- 7Treatment of multiple myeloma: a comprehensive review Clin Lymphoma Myeloma Kyle RA Rajkumar SV 278288920091971737710.3816/CLM.2009.n.056PMC 3910142 · doi ↗ · pubmed ↗
- 8Multiple myeloma Clin J Am Soc Nephrol Singhal S Mehta J 13221330120061769936510.2215/CJN.03060906 · doi ↗ · pubmed ↗