Prevalence of risky sexual behavior and associated factors among Injibara University students, Northwest Ethiopia
Mekdes Abera Adal, Saron Abeje Abiy, Mebratu Mitiku Reta, Mezgebu Silamsaw Asres, Yaregal Animut

TL;DR
This study found that nearly 40% of university students in Ethiopia engaged in risky sexual behaviors, with factors like peer pressure and substance use playing a significant role.
Contribution
The study identifies specific behavioral and knowledge-related factors associated with risky sexual behavior among Ethiopian university students.
Findings
38% of students engaged in risky sexual behaviors.
Substance use and peer pressure were strongly associated with risky behavior.
Only 38% of students had basic HIV knowledge, which was linked to risky sexual behavior.
Abstract
Engaging in risky sexual behaviors can lead to HIV infection, sexually transmitted infections, and unintended pregnancy among youths. University students had greater sexual risks for many reasons. Therefore, this study aimed to assess the magnitude and associated factors of risky sexual behaviors among regular undergraduate students at Injibara University, Northwest Ethiopia. A cross-sectional study was conducted at Injibara University from 20 January to 30 2020. Multistage sampling was employed to select 770 students. Data were collected using a semistructured self-administered questionnaire. A binary logistic regression model was used to identify factors associated with risky sexual behavior. Adjusted odds ratios with 95% CIs were determined, and variables with P-values <0.05 were considered significant. A total of 770 students participated in the study, providing a response rate of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
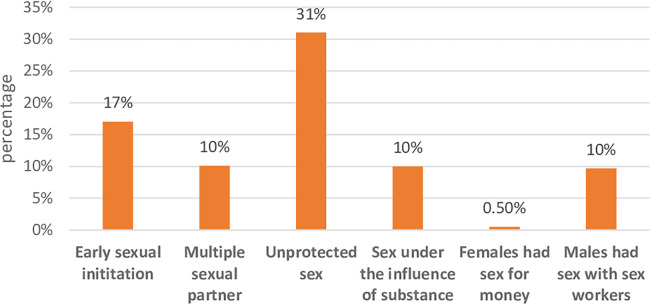 Figure 1
Figure 1| Variables | Categories | Frequency | Percent |
|---|---|---|---|
| Sex | Male | 397 | 51.6 |
| Female | 373 | 48.4 | |
| Age in years | 18–24 | 586 | 76.1 |
| ≥25 | 184 | 23.9 | |
| Marital status | Single | 745 | 96.75 |
| Married | 25 | 3.25 | |
| Religion | Orthodox | 599 | 77.8 |
| Muslim | 81 | 10.5 | |
| Protestant | 68 | 8.8 | |
| Others | 22 | 2.9 | |
| Mother educational level | Unable to read and write | 203 | 26.4 |
| Read and write only | 234 | 30.4 | |
| Primary school | 150 | 19.5 | |
| secondary school | 112 | 14.5 | |
| Collège and above | 71 | 9.5 | |
| Father educational level | Unable to read and write | 169 | 21.9 |
| Read and write only | 252 | 32.7 | |
| Primary school | 203 | 26.4 | |
| Secondary school | 68 | 8.8 | |
| Collège and above | 78 | 10.1 | |
| Year of study | Second year | 482 | 62.6 |
| Third year | 288 | 37.4 | |
| Monthly pocket money | ≤500ETB | 613 | 79.61 |
| >500ETB | 157 | 20.39 |
| Variables | Frequency | Percent |
|---|---|---|
| Alcohol drinking | ||
| Yes | 240 | 31.2 |
| No | 530 | 68.8 |
| Khat chewing | ||
| Yes | 68 | 8.8 |
| No | 702 | 91.2 |
| Cigarette smoking | ||
| Yes | 57 | 7.4 |
| No | 713 | 92.6 |
| Hashish use | ||
| Yes | 40 | 5.2 |
| No | 730 | 94.8 |
| Facebook use | ||
| Yes | 484 | 62.9 |
| No | 286 | 37.1 |
| Watch pornography | ||
| Yes | 246 | 31.9 |
| No | 524 | 68.1 |
| Variables | Categories | Frequency | Percent |
|---|---|---|---|
| Basic HIV transmission and prevention knowledge | Yes | 470 | 61 |
| No | 300 | 39 | |
| HIV risk perception | Yes | 489 | 63.5 |
| No | 281 | 36.5 | |
| Ever tested for HIV | Yes | 542 | 70.4 |
| No | 228 | 29.6 | |
| Peer pressure for sex | Yes | 367 | 47.7 |
| No | 403 | 52.3 | |
| Ever had sexual intercourse | Yes | 346 | 44.9 |
| No | 424 | 55.1 | |
| Age at first sexual intercourse ( | <18 years | 131 | 37.9 |
| ≥18 years | 215 | 62.1 | |
| Life time number of sexual partners ( | 1 | 246 | 71.1 |
| ≥2 | 100 | 28.9 | |
| Number of sexual partners in the last one year ( | none | 99 | 28.6 |
| 1 | 169 | 48.8 | |
| ≥2 | 78 | 22.5 | |
| History of sexual intercourse with FSW (for males) ( | Yes | 75 | 36.1 |
| No | 133 | 63.9 | |
| Sex while under the influence of substance ( | Yes | 77 | 22.3 |
| No | 269 | 77.7 | |
| Condom use ( | Inconsistent | 185 | 53.5 |
| Consistent | 107 | 30.9 | |
| Never used | 54 | 15.6 | |
| Condom use during the last sex ( | Yes | 153 | 44.2 |
| No | 193 | 57.8 |
| Variables | Categories | Risky sexual behaviours | COR (95% CI) | AOR (95% CI) | ||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| Marital status | Single | 290 | 455 | 3.35 (1.14, 9.85)* | 2.58 (0.84, 7.89) | 0.096 |
| Married | 4 | 21 | 1 | 1 | ||
| Study year | 2nd year | 195 | 287 | 1.30 (0.96, 1.76) | 1.41 (0.98, 1.97) | 0.15 |
| 3rd year | 99 | 189 | 1 | 1 | ||
| HIV tested | Yes | 189 | 353 | 1 | 1 | |
| No | 105 | 123 | 1.59 (1.16, 2.18)* | |||
| Basic HIV knowledge | Yes | 148 | 322 | 1 | 1 |
|
| No | 146 | 154 | 2.06 (1.53 (2.78)** | |||
| Contraceptive knowledge | Yes | 213 | 286 | 1.75 (1.28, 2.39)* | 1.48 (0.98,2.11) | 0.26 |
| No | 81 | 190 | 1 | 1 | ||
| Substance use | Yes | 64 | 29 | 4.29 (2.69, 6.84)** | ||
| No | 230 | 447 | 1 | 1 |
| |
| Peer pressure | Yes | 170 | 197 | 1.94 (1.45, 2.61)** | ||
| No | 124 | 279 | 1 | 1 |
| |
| Watch pornography | Yes | 127 | 119 | 2.28 (1.67, 3.11)** | ||
| No | 167 | 357 | 1 |
| 1 | |
| Alcohol drinking | Yes | 112 | 128 | 1.67 (1.23, 2.28) | 1.01 (0.70, 1.45) | 0.97 |
| No | 182 | 348 | 1 | 1 | ||
| HIV risk perception | Yes | 177 | 312 | 1 | 1 |
|
| No | 117 | 164 | 1.26 (0.93, 1.70) | |||
- —University of Gondar10.13039/501100007861
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFlowering Plant Growth and Cultivation · Plant Physiology and Cultivation Studies · Postharvest Quality and Shelf Life Management
Introduction
Risky sexual behavior is defined as any sexual activity that increases the risk of contracting sexually transmitted infections (STIs) and unintended pregnancy, which includes having sex with multiple sexual partners, early initiation of sexual intercourse under the age of 18 years, and unprotected sex (1, 2).
Sexual and reproductive health problems are among the main causes of death, disability, and disease among young people worldwide. According to the Centers for Disease Control and Prevention (CDC) report, 20% of all new HIV diagnoses and more than half of the nearly 20 million new STIs were among young people (aged 15–24 years) in 2020, and more than 145,000 infants were born to adolescent females in 2021 (1). HIV/AIDS is the second leading cause of death globally and the leading cause of death in Africa among young people (2). Globally, approximately 14,000 new HIV infections occur daily due to risky sexual behavior, with more than 95% of them in developing countries. Particularly, in sub-Saharan Africa, HIV/AIDS and unintended pregnancies continue to be major causes of mortality and morbidity among adolescents (3–5). According to the Ethiopian Demographic and Health Survey (EDHS) report, the percentage of first sexual intercourse among young people in Ethiopia aged between 18 and 24 who have had sex before age 18 has increased from 35% in 2016 to 40% in 2019 among women and from 9% to 12% among men (6, 7).
The transition from high school to university on its own has been identified as a major life stressor for many young people (8). During this period, many students live away from their homes for the first time, which may result in a great decrease in contact and support from family and friends (9). In addition, in this period, students have to deal with greater autonomy, enhanced academic demands and new social relationships. Furthermore, most university youths take risks due to a lack of knowledge, or they think that they are invulnerable (10). During the process of dealing with these university life challenges, students may engage in risky sexual behaviors that cause poor health outcomes both physically and mentally (11).
In Ethiopia, sexual matters are very sensitive and less likely to be discussed openly. Little attention is given to sexual and reproductive services for youths (12). Although youths are assets of society and change agents in filling the gap in the past and on whom the future generation is based, most HIV-related interventions target the general public; as a result, they do not directly respond to higher education students' needs, making actual coverage of behavioral and biomedical interventions for youths extremely low (13). Neglecting their sexual and reproductive health can lead to high social and economic costs, both immediately and in the years ahead (13). Understanding the determinants of university youth's risky sexual behaviors is an essential step toward curtailing the spread of STIs/HIV/AIDS and unintended pregnancies. Therefore, this study aimed to assess the magnitude and factors associated with risky sexual behavior among undergraduate regular students at Injibara University.
Methods
Study design and period
An institution-based cross-sectional study was conducted among regular students at Injibara University from January 20 to 30, 2020 G.C.
Study area and setting
The study was conducted at Injibara University located in the Awi zone of the Amhara region, 114 km from Bahir-Dar and 447 km from Addis Ababa, the nation's capital. According to the data from the registrar and alumni directorate, there were 2,269 regular undergraduate students (1,282 males and 1,024 females) in the university at the beginning of the 2019/20 academic year. Of the total regular students, 1,245 were in their second year, and 1,024 were in their third year. First-year students for the 2019/20 academic year were not registered at the time of data collection.
Study population
All Injibara University undergraduate regular students during the study period were included in this study.
Inclusion criteria:
All Injibara University undergraduate regular students during the study period were included in this study regardless of having or not having their first sexual intercourse. Exclusion criteria:
Students with vision disability were excluded from the study as they can't fill self-administered questionnaire.
Sample size and sampling technique
The sample size was determined using a single population proportion formula using the following assumptions: the probability of an event from the previous study was 35%, the proportion of students who had experienced risky sexual behaviors in a study conducted at Mizan Aman College of Health Sciences (14), the probability of type 1 error or alpha was 0.05, and the 95% confidence level. The sample size was also calculated using the double population proportion formula for the second objective by considering different odds ratios (ORs) of significant factors from previous studies, including alcohol consumption, peer pressure and khat chewing. However, the largest sample size, which was found in the following formula, was considered as the final sample size.
Adding a 10% nonresponse rate and design effect 2, we use a final sample size of 770.
A multistage sampling technique was employed to select students from four colleges of Injibara University (Social Sciences and Humanities College, Business and Economics College, Agriculture, Food and Climate College, and Natural and Computational Sciences College). Samples were proportionally allocated to each college and then further allotted based on the year of study and the number of males and females proportionally. Finally, participants were selected randomly using the lottery method from the selected class.
Variables of the study
Dependent Variables: Risky sexual behavior (Yes/No).
Independent variables
Sociodemographic variables: Age, sex, religion, parental education level, pocket money, marital status, and year of study.
Knowledge and psychosocial factors: HIV risk perception, use of VCT, peer pressure, knowledge of contraceptive methods, and basic HIV knowledge.
Behavioral factors: Substance use, alcohol, khat, cigarette and social media use pornography videos, Facebook.
Operational definition
Risky sexual behaviors: a student who practiced at least one of the following**:** early initiation of sexual intercourse, unprotected sex, having sex with sex workers, having sexual intercourse with multiple sexual partners and practicing sexual intercourse while under the influence of substances in the last 12 months (14–18).
Early initiation of sex: a student who experienced sexual intercourse before 18 years old (14, 19).
Unprotected sex: a student who did not use a condom at every act of sexual intercourse (sex without a condom or inconsistent use of a condom) was considered to have unprotected sex.
Multiple Sexual Partners: a student who had more than one sexual partner in the last 12 months prior to the study (14).
Sexually active: a student who reported that she/he has had sexual intercourse, irrespective of their marital status at least once prior to the study (20).
Basic HIV knowledge: A participant was considered to have basic knowledge of HIV transmission and prevention methods if he/she responded “YES” to the following two questions: (1) People can reduce their chance of getting HIV by having just one uninfected and faithful sexual partner, and (2) People can reduce their chance of getting HIV by using a condom every time they have sex (6).
HIV Risk Perception: Students were asked “What are the chances that you might get HIV?” Responses include no chance, low chance, moderate chance, high chance, and do not know. Then, the data were dichotomized into “Yes” and “No” (21).
Knowledge of contraceptive methods: a student who could list at least one modern contraceptive method was considered knowledgeable (22).
Substance use: a student who has consumed at least one of the substances (khat, cigarettes, and illicit drugs) in any amount in the last 12 months is considered a substance user (23, 24).
Data collection tools and procedure
A pretested and semi structured Amharic-version self-administered questionnaire was used to collect the data. The questionnaire was first prepared in English and then translated to Amharic and back to English by language experts to check consistency and conceptual similarity. Two MSc instructor supervisors and four BSc data collectors were recruited to collect the data. The data collectors and supervisors were trained for 1 day to make them familiar with the questionnaires and the way how to orient the study participants in filling the questionnaire. A pretest was conducted on 5% of the sample size at the University of Gondar before the actual data collection period, and the necessary revisions of questions were made.
Questionnaires were distributed among randomly selected students just after university lessons, and the filled questionnaires were collected on the same day. The selected students were seated at a reasonable distance when they filled out the questionnaire, and they were provided with a box with an opening at the front desk into which they placed all completed questionnaires to ensure anonymity and also to reduce social desirability bias The data collection process was closely monitored by the principal investigator and the supervisors throughout the data collection period. Filled questionnaires were checked regularly for completeness of information, and any problems were immediately discussed with the data collectors.
Data processing and analysis
Data were entered using Epi Info version 7 and exported to SPSS version 25 for analysis. Frequency tables, percentages, and means were used to describe the data. Risky sexual behavior was coded as “1” = “Yes” and “0” = “No” then univariate binary logistic regression was fitted to screen factors for the multivariable binary logistic regression. The Chi-square (χ^2^) assumption was checked for each variable before fitting the univariate binary logistic regression analysis. Variables with P-values ≤0.2 in the bivariable analysis were entered into the multivariable analysis to identify independent factors associated with risky sexual behavior. The adjusted odds ratio (AOR) with 95% CI was calculated, and statistical significance was declared at a P-value of 0.05 in the multivariable analysis. The goodness of fitness of the model was checked using Hosmer and Lemeshow test.
Results
Sociodemographic characteristics
A total of 770 students participated in the study, providing a response rate of 100%. The mean age of the participants was 23.02 (±2.52 SD) years, and the majority of the participants (586, 76.1%) were between the age groups of 18 and 24 years. More than half 397 (51.6%) of the participants were males, and only 30 (3.9%) were ever married. More than three-fourths 599 (77.8%) of the respondents were Orthodox Christian followers, and nearly two-thirds 482 (62.6%) of the participants were second-year students (Table 1).
Substance and social media use
More than one in ten students 93 (12.08%) were substance users. Of these, 68 (8.8%) chewed khat, 57 (7.4%) smoked cigarettes, and 40 (5.2%) smoked Hashish. Nearly two-thirds of the participants [484 (62.9)] used Facebook, and 246 (31.9%) had a habit of watching pornography (Table 2).
Sexual behaviors and HIV-related knowledge
Of the total respondents, 470 (61%) had basic knowledge of HIV transmission and prevention. More than one-third (281, 36.5%) of the participants perceived that they were not at risk of HIV infection. More than two-thirds (542, 70.4%) of the students ever tested for HIV. Nearly half 346 (45%) of the respondents were sexually active, of whom 208 (60%) were males and 138 (40%) were females. The mean age at first sexual intercourse was 18.01 years (SD ± 2.35 years) (18.56 years (SD ± 2.1 years) for males and 17.18 years (SD ± 2.5 years) for females (Table 3).
More than one-third 294 (38.2%) of the participants had risky sexual behavior. Of these, 131 (17%) of the participants started sex before the age of 18 years, 78 (10%) had more than one sexual partner in the last year, 77 (10%) had sexual intercourse under the influence of substance, and 239 (31%) did not use condoms consistently (Figure 1).
Risky sexual behaviors among Injibara undergraduate regular University students, Northwest Ethiopia, January, 2020 (n = 770).
More than half 193 (57.8) of the respondents did not use condoms during their last sexual intercourse. Among sexually active females, 4 (2.9%) had sex for money, and more than one-third of 75 (36.1%) sexually active males had sexual intercourse with female sex workers.
Of the total respondents, 274 (73.5%) females and 222 (56%) males had knowledge of contraceptive methods. Nearly two-thirds (88, 63.8%) of sexually active females had used at least one type of modern contraceptive method, and 16 (11.6%) females had a history of unwanted pregnancy or abortion.
Factors associated with risky sexual behaviors
In this study, factors such as, tested for HIV, basic HIV knowledge, HIV risk perception, peer pressure, watching pornography films, and substance use were associated with risky sexual behavior in the multivariable analysis.
Students who had never been tested for HIV were 1.62 times (AOR = 1.62, 95% CI: 1.15–2.31) more likely to have risky sexual behavior than those who had been tested for HIV. Similarly, students who lacked basic knowledge of HIV were 2.16 times (AOR = 2.16, 95% CI: 1.56–2.98) more likely to engage in RSB than those who had basic HIV knowledge.
Participants who faced peer pressure for sexual intercourse were approximately 2 times (AOR = 1.90, 95% CI: 1.37–2.64) more likely to have risky sexual behavior than those who did not face peer pressure.
Participants who use substances were 3.56 times (AOR = 3.56, 95% CI: 2.11–6.06) more likely to have risky sexual behavior than those who did not use substances. Participants who watched pornography films were 1.58 times (AOR = 1.58, CI: 1.11–2.23) more likely to be involved in risky sexual behavior than those who did not watch pornography films. Students who had no perceived HIV risk were 1.37 times (AOR = 1.37, CI: 1.02–1.19) more likely to have risky sexual behavior than those who had HIV risk perception (Table 4).
Discussion
In this study, the prevalence of risky sexual behavior was 38.2% (95% CI: 35%–42%). This finding was comparable with studies conducted in governmental higher institution students of Debre-Markos town 42% (25), Jimma University 42.1% (26), Mizan Aman University 35% (18), and a systematic review and meta-analysis findings of risky sexual behavior among students in Ethiopian universities 42.8% (17) and 41.62% (27). However, this finding is higher than studies conducted in Arbaminch University students, where the prevalence was 31.4% (28), Aksum University 17% (29), Wolkitie University 20% (30), Debre-Tabor University 28.4% (31), Sri Lanka 12.4% (32), and Southern Nigeria 17.9% (33).
On the other hand, the prevalence of risky sexual behavior in our study is lower than that in studies conducted at Debre-Markos University (58.2%) (34), Jig-Jiga University (54.8%) (35), Bahir-Dar University (62%) (36), Medawalabu University (70.9%) (37), South Africa (81%) (38), Turkey (51.9%) (39), and Brazil (97%) (40). This difference might be due to approaches taken to quantify risky sexual behavior and sociocultural differences. For example, in our study, we assessed multiple sexual partners 12 months prior to the study, while others considered having had more than one sexual partner any time in the past. On the other hand, the study from Bahir-Dar considered any student who is sexually active as having risky sexual behavior (36).
The study revealed that respondents who had never been tested for HIV were 1.62 times more likely to have risky sexual behaviors than those who had been tested for HIV. This finding is supported by evidence from Malawi (41) and the USA (42). The possible reason might be that risk reduction counseling by health care workers to those who tested could help to reduce risky sexual behavior (43).
This study showed that participants who lack basic knowledge of HIV/AIDS transmission and prevention methods are two times more likely to engage in risky sexual behaviors than their counterparts. This finding is supported by studies conducted in Nigeria (44), China (45), and the USA (46). The reason could be that participants who have good knowledge will outweigh the risk of contracting HIV and will be cautious in their sexual relationships (47, 48).
In this study, respondents who consume substances such as smoking cigarette or chewing chat or consume hashish were approximately 3.5 times more likely to practice risky sexual behaviors than their counterparts. This was again supported by studies conducted among students at Madawalabu University (37), Bahir-Dar University (36), Debre Markos University (34), Uganda (49), Debre-Tabor University (31), and studies in nine Asian Countries (50). Usually, substance use and risky sexual behavior go hand in hand (51). This might be due to the nature of these substances, which alter rational decision-making ability, decrease inhibitions and increase the risk-taking behavior of individuals, leading them to have unsafe sex (52).
Peer pressure showed a significant association with risky sexual behavior, with a double increase in the odds of RSB among students with peer pressure compared to students with no peer pressure. This finding was supported by studies conducted among students in Jimma University (53), Nigeria (54), Rwanda (55), and Adama Ethiopia (56). This might be because students share their day-to-day life experience with their friends, and they are likely to behave in a manner intimate friends practice (57). Evidence has revealed that peers have significant influences on young people's behavior (58). Strengthening peer education programs is essential to fostering a culture of healthy peer influence.
Respondents who watched pornography films were more likely to have risky sexual behavior compared to their counterparts. Studies at Bahir-Dar University (36) and a meta-analysis finding among college and university students in Ethiopia (27) supported our finding. The reason might be that watching pornography increases the motivation of sexual desire. Furthermore, adolescent students are sensitive to experimenting with what they hear and look as a result of the natural transition stage to adulthood; hence, they are prone to be driven by porn videos they watch to experiment with risky sex (2, 59).
Participants who had no perceived HIV risk were more likely to have risky sexual behavior than those who had perceived HIV risk. This meant that those who thought themselves not at risk of infection to HIV were more likely to practice risky sexual behavior, which might be associated with underestimating the risk of acquiring HIV infection (60, 61). However, this finding was contrary to findings from studies conducted at Mizan-Aman University (14) and Zimbabwe University (62). This implies that students perceive themselves to be at risk of HIV infection considering their involvement in risky sexual behavior (63, 64).
Based on our findings, it is essential to consider strategic interventions designed to improve the sexual and reproductive health of University students. Implementing sexual educational programs to increase awareness about HIV transmission, prevention methods, and safe sexual practices could be important (61, 65, 66). This could be achieved through peer education programs (67), incorporating sexual health education into the university curriculum across various disciplines (68–71), and through social media where adolescents will be interested in reproductive and sexual health messages (72, 73). Offering easy access to and encouraging confidential HIV testing services on campus, accompanied by counseling and support services, is crucial (74). Making condoms and other reproductive health services readily available and accessible in campus health centers, dormitories, and other relevant locations is also essential (75, 76). Implementing tailored interventions for high-risk groups among university students, such as substance users, female students, and those engaging in unprotected sex, is vital (77–79).
Limitations of the study
Our study could be affected by social desirability bias. Therefore, the magnitude of risky sexual behavior could be underestimated due to the sensitive nature of the topic. Sexuality and sex-related topics are particularly more sensitive among adolescents due to the societal outlook and attitude toward sex at a young age. However, this could be minimized since we used a self-administered questionnaire to collect the data. In addition, in this study, we could not establish a temporal relationship between the factors and the outcome due to the cross-sectional nature of the study.
The study was limited to university students, so the results may not be generalizable to other adolescents with diverse lifestyles. Thus, the findings of this study should be interpreted with these limitations.
Conclusion
The prevalence of risky sexual behavior among undergraduate regular university students was high. Risky sexual behaviors are more likely to occur when students are under peer pressure, use substances, have no perceived HIV risk, watch pornography, and have inadequate basic HIV knowledge. Therefore, strategies such as life skill training should be designed to bring positive behavioral changes among university students.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Centers for Communicable Diseases Control and Prevention (CDC). Adolescent and school health, sexual risk behaviors (2021). Available online at: https://www.cdc.gov/healthyyouth/sexualbehaviors/index.htm (accessed January 16, 2022).
- 2UNAIDS. Active Involvement of Young People Agains HIV/AIDS. New York: UNAIDS (2015).
- 3World Health Organization. Sexual health and its linkages to reproductive health: an operational approach (2017).
- 4Yakubu I Salisu WJ. Determinants of adolescent pregnancy in sub-Saharan Africa: a systematic review. Reprod Health. (2018) 15(1):15. 10.1186/s 12978-018-0460-429374479 PMC 5787272 · doi ↗ · pubmed ↗
- 5Idele P Gillespie A Porth T Suzuki C Mahy M Kasedde S Epidemiology of HIV and AIDS among adolescents: current status, inequities, and data gaps. JAIDS J Acquir Immune Defic Syndr. (2014) 66:S 144–53. 10.1097/QAI.000000000000017624918590 · doi ↗ · pubmed ↗
- 6Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF (2017).
- 7Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report. Rockville, Maryland, USA: EPHI and ICF (2021).
- 8Bray SR Born HA. Transition to university and vigorous physical activity: implications for health and psychological well-being. J Am Coll Health. (2004) 52(4):181–8. 10.3200/JACH.52.4.181-18815018429 · doi ↗ · pubmed ↗