Fibrolamellar Hepatocellular Carcinoma (FLHCC) in a Young Patient Presenting With Nausea and Vomiting After a Greasy Meal
Mohamed Ismail, Sahiba Singh, Menna-Allah Elaskandrany, David s Kim, Yazan Abboud, Michael Bebawy, Abena Oduro, Ritik mahaveer Goyal, Omar Mohamed, Weizheng Wang

TL;DR
A 38-year-old man with no liver disease history was diagnosed with rare liver cancer after presenting with nausea and vomiting following a fatty meal.
Contribution
Highlights a rare presentation of FLHCC and emphasizes the need for thorough evaluation in young patients with hepatic lesions.
Findings
FLHCC was diagnosed in a young patient without underlying liver disease through biopsy after nonspecific symptoms.
Successful surgical resection was performed with postoperative stability at six months.
The case underscores the importance of considering FLHCC in differential diagnoses for hepatic lesions in young individuals.
Abstract
Fibrolamellar hepatocellular carcinoma (FLHCC) is a rare and distinct subtype of liver cancer, predominantly affecting younger patients without underlying liver diseases. This case report discusses a unique presentation of FLHCC in a 38-year-old male with a past medical history of a well-controlled seizure disorder. The patient presented with nausea, vomiting, and abdominal pain following a fatty meal. Laboratory tests revealed elevated liver enzymes and anemia, and imaging showed a large hepatic lesion. Initial management included a septic workup and broad-spectrum antibiotics. However, a liver biopsy performed subsequently revealed the presence of FLHCC. The patient underwent a successful open right hepatectomy and was managed postoperatively with consideration of his seizure disorder. Follow-up at six months showed a stable postoperative condition without any evidence of recurrence.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3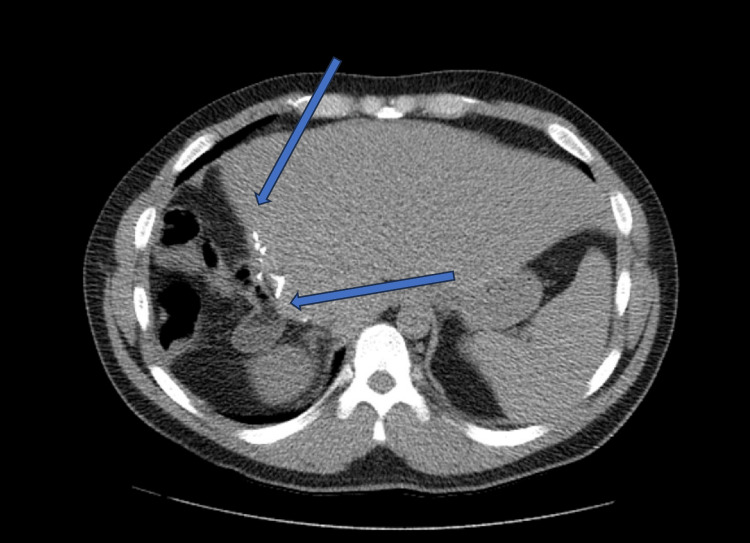 Figure 4
Figure 4| Lab test | Patient values | Reference range |
| Hemoglobin (HGB) | 10.9 g/dl | 14-18 g/dl |
| WBC | 12 K/µl | 4-11 K/µl |
| Alkaline Phosphatase | 153 U/L | 40-130 U/L |
| Bilirubin Total | 0.9 mg/dl | <= 1.0 mg/dl |
| AST | 48 U/L | 0-40 U/L |
| ALT | 124 U/L | 0-41 U/L |
| Procalcitonin | 3.78 ng/ml | <0.50 ng/ml |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Cancer Mechanisms and Therapy · Cholangiocarcinoma and Gallbladder Cancer Studies
Introduction
FLHCC is a rare malignancy with a relatively unknown etiology and comprises about 1% of cases of liver neoplasms [1-4]. Patients diagnosed with hepatocellular carcinoma (HCC) generally belong to an older age group and often exhibit coexisting cirrhosis and elevated liver enzyme levels. In contrast, FLHCC predominantly affects a younger demographic, typically between the ages of 14 and 33. Notably, FLHCC occurs in the absence of cirrhosis and is usually not associated with any preexisting diseases [1-6].
Like HCC, FLHCC can invade hepatic veins and manifest as Budd-Chiari syndrome or cause Caval compression syndrome and obstructive jaundice by mass effect due to its large size [5]. Rarely, it can present as gynecomastia in males, fulminant liver failure, recurrent deep vein thrombosis, hypoglycemia, or encephalopathy [4,7]. Some studies have also demonstrated a female preponderance of FLHCC [3,7].
FLHCC does not arise from the common risk factors associated with HCC. Instead, it may be linked with various metabolic paraneoplastic disorders, such as abnormalities in vitamin B12-binding protein, sex steroid metabolism, ammonia processing, neurotensin synthesis, and gonadotropin production, as well as certain genetic syndromes like Gardner syndrome and Fanconi anemia [4,5]. The clinical picture is diverse, but all of these conditions need to be kept in mind as they can be underlying to this disease process.
Symptoms of FLHCC are nonspecific and can range anywhere from the patient being asymptomatic to having nausea, abdominal fullness, weight loss, hepatomegaly, and abdominal pain, which is the most common symptom [1,4,5]. About 50% of patients affected present at advanced stages when the carcinoma has already metastasized, negatively affecting their clinical course [1,6]. However, if detected early enough, surgical resection significantly improves survival outcomes [1,7,8]. The low incidence of the carcinoma makes it challenging to recruit patients for clinical trials, and as a result, treatment options for FLHCC are limited [9,10]. Our case presents another incidence of a novel malignancy, where nonspecific symptoms and unusual patient presentation posed a challenge for diagnosis.
Case presentation
A 38-year-old male patient with a history of a well-controlled seizure disorder managed on 150 mg of lamotrigine daily presented to the hospital reporting nausea, vomiting, and mild, diffuse abdominal pain that commenced following the consumption of a fatty meal the night before. He recalled a similar episode of abdominal pain occurring four months prior, which had resolved spontaneously, leading him to forgo medical consultation. Upon physical examination, the patient exhibited normal vital signs, although tenderness was observed in the right upper quadrant. Laboratory tests revealed elevated levels of liver enzymes, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase. Additionally, anemia was noted with a hemoglobin (HGB) level of 10.9, alongside increased white blood cell (WBC) counts and a heightened procalcitonin level (Table 1).
Tests for hepatitis B surface antigen (HBsAg) and hepatitis C virus antibody (HCV Ab) were negative. An abdominal ultrasound detected a 10.3 x 6.6 x 10.0 cm mass in the right hepatic lobe. Further assessment with computed tomography (CT) scan of the abdomen and pelvis with Intravenous (IV) contrast confirmed the presence of a large hepatic lesion in the right lobe, measuring approximately 10.0 x 6.4 x 10.4 cm, with heterogeneous attenuation (Figure 1).
CT scan of the abdomen and pelvis with IV contrast A large hepatic lesion in the right lobe, measuring approximately 10.0 x 6.4 x 10.4 cm, with heterogeneous attenuation.
Notably, tumor markers, including alpha-fetoprotein (AFP) and carcinoembryonic antigen (CEA), were within normal ranges. The initial clinical impression was a hepatic abscess, although a necrotic liver tumor was considered a differential diagnosis. Consequently, infectious disease specialists were involved, and the patient was subjected to a septic evaluation (including blood and urine cultures, and chest x-ray) and commenced on broad-spectrum antibiotics (piperacillin/tazobactam 3.375 g IV every 6 hours and metronidazole 500 mg every 8 hours).
An interventional radiology-guided liver biopsy was performed. Results from the septic workup were negative. Histopathological examination of the biopsy specimen revealed malignant cells, characterized by dyscohesive cells with enlarged nuclei, prominent nucleoli, oncocytic cytoplasm containing intra-cytoplasmic lumens and granules, and occasional fibrous tissue fragments and granular debris. These pathological findings were highly suggestive of fibrolamellar hepatocellular carcinoma (Figure 2).
Microscopic Histological Patterns of FLHCC(A) Malignant cells, characterized by dyscohesive cells with enlarged nuclei, prominent nucleoli, oncocytic cytoplasm containing intra-cytoplasmic lumens and granules, with background fibrosis and granular debris (H&E, high power magnification). (B) Enlarged nuclei, oncocytic cytoplasm, with background fibrosis and granular debris (H&E, low power magnification).
The antibiotic regimen was discontinued following this diagnosis, and the patient was referred to surgical oncology for further management. The investigation for metastasis using a whole-body CT scan yielded negative results, leading to the formulation of a surgical plan to resect the tumor. The patient underwent a successful open right hepatectomy, and a Jackson-Pratt (JP) drain was placed in the right upper quadrant during the procedure (Figure 3).
CT scan of abdomen and pelvis With IV Contrast Status post right hepatectomy for FLHCC
Postoperatively, the patient had an uneventful recovery in the post-anesthesia care unit (PACU) and was subsequently transferred to the general ward. The JP drain was removed, and following a neurology department evaluation for epilepsy management, the patient was discharged in stable condition. A six-month follow-up at the surgical oncology outpatient clinic revealed the patient to be asymptomatic, and a follow-up CT scan of the abdomen and pelvis with IV contrast showed a stable postoperative state, with no enhancing hepatic lesions noted (Figure 4).
CT scan of abdomen and pelvis with IV contrastSix-month follow-up CT scan demonstrated a stable postoperative condition, with no enhanced hepatic lesions observed.
Discussion
The uncommon occurrence and indistinct clinical findings of FLHCC can lead to a failure in early detection [3,4,7]. This emphasizes the diagnostic challenges in managing this carcinoma, and as a result, many patients present at an advanced stage in the disease [1,6].
Diagnosis of FLHCC is usually achieved by the patient's clinical presentation and imaging [10]. Ultrasonography is commonly used for evaluation; however, features are usually nonspecific and necessitate further imaging by either CT or magnetic resonance imaging (MRI) [1,4,11]. Lesions are typically hypervascular, solitary, well-delineated, and may have a central scar [1,4,11]. Indeterminate lesions by imaging may need to undergo fine needle aspiration or biopsy for definitive diagnosis [4]. FLHCC can be confused for hypervascular liver lesions such as hepatic adenomas, focal nodular hyperplasia, hemangiomas, and hepatocellular carcinoma and must be differentiated [4,11].
Furthermore, nearly all cases of FLHCC have been identified with the presence of an oncogenic DNAJB1-PRKACA fusion protein and a heightened capacity for serum vitamin B12 binding, both of which were not evaluated in our case [2-6,10]. Although they are not specific for this carcinoma, these findings, along with clinical presentation and imaging, can help provide a diagnosis. The DNAJB1-PRKACA fusion gene can also aid in differentiating FLHCC from HCC since it is not present in the latter case [8].
Pathology remains the gold standard for diagnosis, and FLHCC tumor cells will demonstrate an eosinophilic cytoplasm with prominent nuclei and a fibrous stroma arranged in parallel lamellae [5,8,10].
In scenarios where hepatocellular carcinoma (HCC) is suspected in patients with non-cirrhotic livers and diagnostic imaging fails to conclusively identify HCC-as exemplified by our patient with a non-cirrhotic, healthy liver where imaging did not confirm liver cancer, yet the differential diagnosis raised the possibility of either liver cancer or a hepatic abscess-a histological examination through liver biopsy may become imperative [12]. The clinical team, assessing the necessity of a fine needle biopsy, engaged in thorough discussions with the patient regarding the risks and benefits of the procedure. Given the relatively low risk of tumor seeding, as documented in prior studies, the patient consented to the biopsy.
The practice of utilizing image-guided liver biopsies, conducted via CT scans and ultrasound, is affirmed as the premier diagnostic standard for lesions that are indeterminate upon imaging [13]. Pain, ranging from mild discomfort to more pronounced discomfort, emerges as the most prevalent complication, affecting up to 84% of patients who undergo liver biopsy. While serious adverse events such as gallbladder perforation, bile peritonitis, haemobilia, pneumothorax, or hemothorax are exceedingly rare, they highlight the inherent risks of the procedure [12]. Notably, despite the predominance of arteriolar severe hemorrhages, the application of ultrasound guidance has been shown to not significantly mitigate bleeding risks, though it effectively reduces the frequency of overall complications [12].
The potential for needle biopsies to disseminate cancer cells along the tract of needle insertion has been a subject of concern, although the precise dynamics and actual risk remain partially understood [12]. A widely referenced meta-analysis reported a 2.7% incidence of cancer cell dissemination in 1340 biopsies. However, incorporating findings from three additional, more contemporary studies suggests the possibility of significantly lowering these dissemination rates to below 1% [12,14,15]. Furthermore, the clinical significance of seeding has generally been minimal, with most instances being effectively managed through surgical or ablative interventions, thereby not adversely impacting patient morbidity or mortality [12].
Surgical resection remains the mainstay for treatment, although these tumors are aggressive, and recurrence of the carcinoma is common because of the large tumor size and the majority of patients presenting at an advanced stage [1,3,4,8,10]. Patients unable to undergo resection due to metastasis or major vessel involvement have a 5-year survival rate of 0-5% in comparison to a 58-82% rate of those who underwent surgery [4,7,8]. Favorable prognostic indicators include female gender and locoregional disease without lymph node involvement [3,4,10].
Chemotherapy can be used as a treatment option before or after surgery for FLHCC. However, there is limited research on the most effective chemotherapeutic regimen due to the low occurrence of this type of cancer. It should be noted that there are currently no reported neoadjuvant/adjuvant systemic therapies that have improved survival rates for patients with resectable FLHCC [1,16].
New research has focused on using the latest understanding of FLHCC's pathogenesis and molecular genetics to improve treatment options, along with systemic chemotherapy. For example, a current multi-institutional, randomized controlled trial is exploring the effectiveness of combining mTOR inhibition with estrogen suppression to treat FLHCC. Additionally, studies have shown that FLHCC expresses increased levels of epithelial growth factor receptor and transforming growth factor beta, making these potential targets for future treatments [16].
Conclusions
FLHCC represents a significant diagnostic and therapeutic challenge due to its rarity, unique demographic profile, and often indistinct clinical presentations. This case underscores the importance of maintaining a high index of suspicion for FLHCC in young patients presenting with hepatic lesions, even in the absence of traditional risk factors for liver neoplasms. The fact that FLHCC typically presents at a more advanced stage and the lack of specific systemic therapies highlight the urgent need for early detection and the development of effective treatment strategies.
The emerging understanding of the molecular pathogenesis of FLHCC, including the DNAJB1-PRKACA gene fusion and the role of increased serum vitamin B12 binding capacity, offers new avenues for research and potentially targeted therapies. Continued research is critical to unravel the complexities of FLHCC, improve diagnostic methods, and develop more effective treatment modalities, thereby improving outcomes for this unique and challenging patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fibrolamellar Hepatocellular Carcinoma Smith M Tomboc PJ Markovich B Treasure Island (FL)Stat Pearls [Internet]2024 https://www.ncbi.nlm.nih.gov/books/NBK 553113/31971753 · pubmed ↗
- 2DNAJB 1-PRKACA is specific for fibrolamellar carcinoma Mod Pathol Graham RP Jin L Knutson DL 8228292820152569806110.1038/modpathol.2015.4 · doi ↗ · pubmed ↗
- 3Treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma: a national perspective J Am Coll Surg Mayo SC Mavros MN Nathan H 19620521820142431588610.1016/j.jamcollsurg.2013.10.011PMC 4596238 · doi ↗ · pubmed ↗
- 4Management of fibrolamellar hepatocellular carcinoma Chin Clin Oncol Chaudhari VA Khobragade K Bhandare M Shrikhande SV 51720183039571810.21037/cco.2018.08.08 · doi ↗ · pubmed ↗
- 5Fibrolamellar hepatocellular carcinoma Tumors and Tumor-Like Lesions of the Hepatobiliary Tract Zimmermann A. Springer, Cham 2016
- 6Fibrolamellar carcinoma: challenging the challenge Eur J Cancer Lamarca A Frizziero M Fulton A 14414713720203276887210.1016/j.ejca.2020.06.035 · doi ↗ · pubmed ↗
- 7Clinicopathologic characteristics and survival outcomes of patients with fibrolamellar carcinoma: data from the Fibrolamellar Carcinoma Consortium Gastrointest Cancer Res Ang CS Kelley RK Choti MA 3962013 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 3597938/23505572 PMC 3597938 · pubmed ↗
- 8Fibrolamellar hepatocellular carcinoma that was successfully treated with surgical resection: a case report J Liver Cancer Na SK 1781822220223738341710.17998/jlc.2022.06.10PMC 10035731 · doi ↗ · pubmed ↗