A Case of Cotyledonoid Dissecting Leiomyoma With Associated Disseminated Peritoneal Leiomyomatosis: The Significance of Frozen Section in Identification of This Unusual Entity
Diksha Karki, Girishma Shrestha, Saurav L Joshi

TL;DR
This paper reports a rare case of a benign uterine tumor with peritoneal spread, emphasizing the importance of frozen section biopsies for accurate diagnosis.
Contribution
The paper presents the first documented case of cotyledonoid dissecting leiomyoma with disseminated peritoneal leiomyomatosis.
Findings
Frozen section biopsy confirmed the benign nature of peritoneal deposits during surgery.
Histopathology and immunohistochemistry confirmed the smooth muscle origin of the tumor.
No recurrence was observed in a seven-month follow-up period.
Abstract
Cotyledonoid dissecting leiomyoma (CDL) is a rare variant of uterine leiomyoma. The tumor is benign, but the appearance and growth pattern are unusual and alarming. Disseminated peritoneal leiomyomatosis (DPL) is another rare tumor that can mimic malignancy. The occurrence of these two tumors in a single case is even rarer and has not been found in the literature to the best of our knowledge. We report a case of CDL with DPL in a 43-year-old Nepalese woman who presented with abdominal pain and per vaginal bleeding. Ultrasound showed a heterogeneous hypoechoic mass of size 25.1 × 15.5 × 9.4 cm in the pelvic cavity. A CT scan of the abdomen and pelvis revealed an ill-defined, heterogeneously enhancing lesion in the pelvis around the uterine fundus with a peritoneal nodule. The intraoperative frozen section evaluated the peritoneal deposit to be benign. Due to the large size of the uterine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
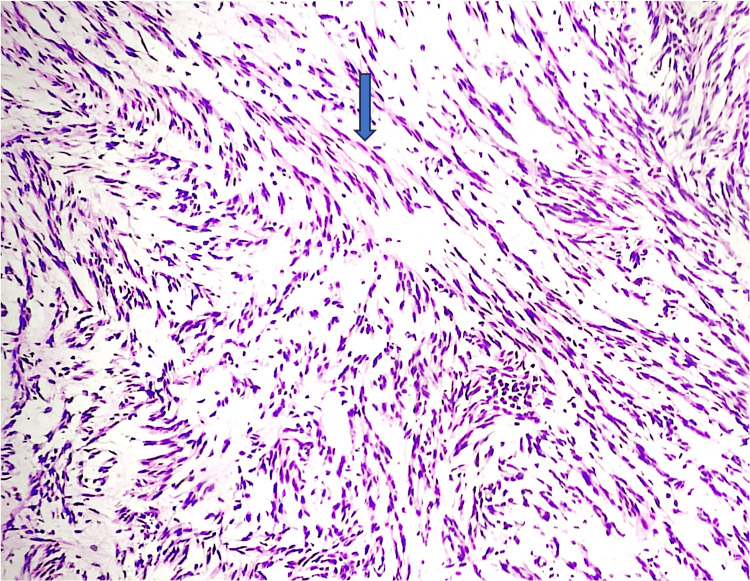 Figure 1
Figure 1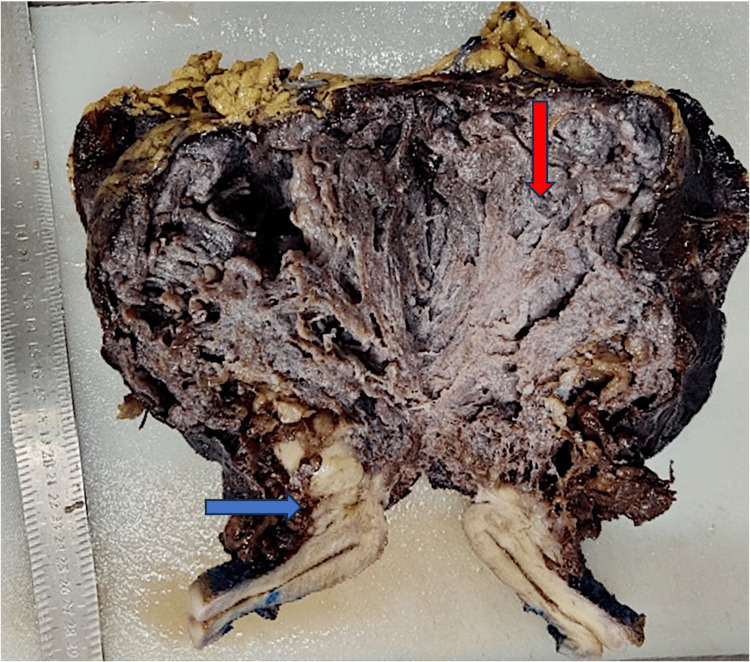 Figure 2
Figure 2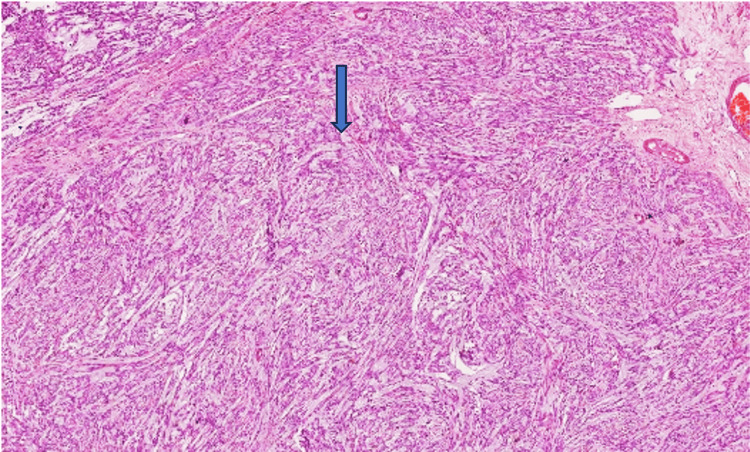 Figure 3
Figure 3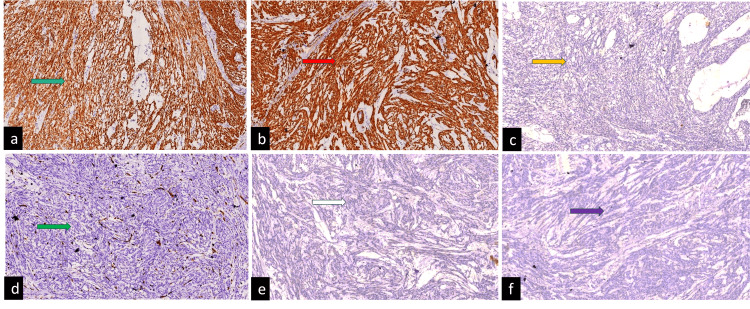 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtmospheric and Environmental Gas Dynamics · Atmospheric aerosols and clouds · Meteorological Phenomena and Simulations
Introduction
Cotyledonoid dissecting leiomyoma (CDL) is a rare variant of leiomyoma that was first described in a series of four cases by Roth et al. [1]. This variant of leiomyoma is characterized by multinodularity with dissection of the myometrium along with exophytic extrauterine growth that looks like the cotyledon of the placenta [1]. Disseminated peritoneal leiomyomatosis (DPL) is another rare benign entity where multiple nodules comprising smooth muscle are found throughout the peritoneal cavity [2]. The unusual growth pattern can make the identification of this benign tumor challenging both clinically and radiologically, and histomorphology, along with the addition of immunohistochemistry (IHC) markers, can pave the path to the correct diagnosis. The literature search shows individual case reports of CDL and DPL, but the occurrence of these two rare tumors in the same patient has not been reported. To our knowledge, this is the first reported case from Nepal.
Case presentation
A 43-year-old Nepalese woman presented with a history of abdominal distension and pain for three months and per vaginal discharge for one month. Her complete blood counts were within normal limits. Ultrasonography of the abdomen and pelvis was done, which showed a pelvic mass measuring 25.1 × 15.5 × 9.4 cm with moderate echogenic fluid collection and probe tenderness. Her tumor marker CA125 was within normal limits. A CT scan of the abdomen and pelvis was performed, which showed an ill-defined heterogeneously enhancing lesion seen in the pelvis around the uterine fundus, encased within the peritoneal fluid collection without separate visualization of bilateral ovaries, and nodular enhancing thickening of the lining peritoneum, which was suspected to be bilateral ovarian malignancy with peritoneal metastasis. As the mass was suspicious of malignancy, the patient underwent a staging laparotomy, followed by a biopsy of the peritoneal deposit, right fallopian tube, and ovary, and was sent for a frozen section. A frozen section (Cryostat 6250, Dakewe) biopsy from peritoneal deposits showed benign-looking spindle-shaped cells with eosinophilic cytoplasm devoid of atypia (Figure 1).
A frozen section biopsy from peritoneal deposits shows benign-looking spindle-shaped cells (shown in the blue arrow) with eosinophilic cytoplasm devoid of atypia, mitosis, and necrosis.
Mitosis and necrosis were not identified. An intraoperative diagnosis of a benign spindle cell lesion was made. Sections from the right fallopian tube and ovary were negative for malignancy. Intraoperatively, a huge exophytic brown mass was seen arising from the posterior surface of the uterus, approximately measuring 20 × 15 × 10 cm, for which the patient underwent total abdominal hysterectomy, left salpingo-oophorectomy, pelvic peritoneal biopsy, and was sent to the histopathology lab. On gross examination, a mass of size 22 × 15 × 11 cm is present, arising from the posterior surface of the uterine serosa. The outer surface is irregular and dark brown. The cut surface shows an exophytic brown-colored solid cystic mass with interconnecting spaces with outer myometrial involvement. The myometrial component of mass has a multinodular appearance with a solid gray-white area (Figure 2).
The cut surface shows an exophytic brown-colored solid cystic mass with interconnecting spaces (shown in the red arrow) and outer myometrial involvement. The myometrial component of mass has a multinodular appearance with a solid gray-white area (shown in the blue arrow).
The boundary between the mass and the myometrium was unclear. No necrosis was identified grossly. The endometrium, cervix, and bilateral adnexa were grossly unremarkable. On microscopic examination, a H&E-stained slide revealed a multinodular pattern showing spindle-shaped cells arranged in bundles and fascicles with a moderate amount of eosinophilic cytoplasm, uniform elongated nuclei, a fine chromatin pattern, and inconspicuous nucleoli. Numerous congested and dilated vessels and edematous connective tissue between nodules were found (Figure 3).
H&E-stained slide revealed spindle-shaped cells arranged in bundles and fascicles with a moderate amount of eosinophilic cytoplasm (shown in the blue arrow), uniformly elongated nuclei, a fine chromatin pattern, and inconspicuous nucleoli.
Areas of hyalinization and hemorrhages were noted. The spindle cells are seen dissecting the myometrial fibers. No necrosis, atypia, or mitosis were identified. Sections examined from the multiple peritoneal deposits also show benign spindle-shaped cells having similar morphology and devoid of atypia, mitosis, and necrosis. Further, IHC was performed, and tumor cells were positive for smooth muscle actin (1A4, Dako) and desmin (D33, Dako) (Figure 4).
On IHC, tumor cells were positive for smooth muscle actin (a, green arrow) and desmin (b, red arrow). Ki67 labeling index was approximately <1% (c, yellow arrow), while they were negative for CD34 (d, green arrow), negative for DOG1 (e, white arrow), and negative for CK (AE1/AE3) (f, purple arrow).IHC, immunohistochemistry
While negative for CD117 (c-kit, Dako), DOG1 (DOG1.1, Dako), CK (AE1/AE3, Dako), and CD34 (QBEnd10, Dako), Ki67 (MIB-1, Dako) labeling index was approximately <1%. Correlating the gross, histopathology, and IHC findings, a final diagnosis of CDL with DPL is rendered.
Discussion
The CDL of the uterus, also known as “Sternberg tumor,” depicts an unusual growth pattern that can create a diagnostic dilemma [1]. The case presented exhibited an exophytic, huge mass arising from uterine serosa, which radiologically and intraoperatively suggested malignancy. In addition, the presence of multiple peritoneal nodules indicated a disseminated disease. In such circumstances, frozen section biopsy has proven to be a promising tool in determining the nature of the lesion, which will avoid unnecessary surgical procedures. The overall accuracy of the frozen section is 93.3%, which allows the surgeons to make appropriate intraoperative decisions [3]. In the present case, a frozen section biopsy from the peritoneal nodules showed spindle cells devoid of atypia and mitosis, suggesting they were benign, which prevented further radical dissection in this patient.
The unusual gross appearance of the tumor with multiple peritoneal nodules and leiomyosarcoma with peritoneal metastasis come under differentials [2,4,5]. However, the histopathological findings, including the absence of tumor coagulation necrosis, mitotic activity, cellular atypia, and a low ki67 index in the IHC, as seen in the current case, can rule out malignancy. The hormonal influence, intraperitoneal implants following morcellation of myoma, genetic factors, and metaplasia of submesothelial mesenchymal cells have been postulated for DPL [4,5]. None of such a history could be traced in the present case, except that she is of reproductive age.
After seven months of surgery, the patient is on regular follow-up, and no associated complications have been identified.
Conclusions
CDL and DPL are rare tumors, and their occurrence in a single patient is an even rarer finding. Awareness of these tumors and recognition of their bizarre gross appearance are important for appropriate classification and to avoid unnecessary surgical procedures in patients. Whenever available, prompt frozen biopsy assessment and further application of IHC markers can pave the way for the correct diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cotyledonoid dissecting leiomyoma of the uterus. The Sternberg tumor Am J Surg Pathol Roth LM Reed RJ Sternberg WH 14551461201996894403810.1097/00000478-199612000-00004 · doi ↗ · pubmed ↗
- 2An unusual presentation of pelvic leiomyomatosis misdiagnosed as disseminated malignancy Case Rep Pathol Marwah N Duhan A Aggarwal G Sen R 394106201220122319823110.1155/2012/394106 PMC 3502812 · doi ↗ · pubmed ↗
- 3The evaluation of intra-operative frozen section diagnosis accuracy of ovarian tumors; old fashioned not out of fashion Asian Pac J Cancer Prev Muruthapongsatorn P Inploy N Prommas S Smanchat B Bhamarapravatana K Suwannarurk K 369737012020193187011110.31557/APJCP.2019.20.12.3697 PMC 7173390 · doi ↗ · pubmed ↗
- 4Disseminated peritoneal leiomyomatosis: an unusual presentation of intra-abdominal lesion mimicking disseminated malignancy Med Pharm Rep Soni S Pareek P Narayan S 1131169320203213345510.15386/mpr-1421 PMC 7051819 · doi ↗ · pubmed ↗
- 5Disseminated peritoneal leiomyomatosis as an incidental finding: a case report Clin Case Rep Morgan ED Kahiye M Kule I Yahaya JJ Othieno E 010202210.1002/ccr 3.5541 PMC 889882035280083 · doi ↗ · pubmed ↗