Pre-extensively Drug-Resistant Pulmonary Tuberculosis With a Giant Primary Splenic Hydatid Cyst With Multiple Adverse Drug Reactions
Sankalp Yadav

TL;DR
A rare case of drug-resistant tuberculosis combined with a large hydatid cyst in the spleen is reported, highlighting treatment challenges and side effects.
Contribution
This is the first reported case of pre-extensively drug-resistant pulmonary tuberculosis co-occurring with a giant splenic hydatid cyst.
Findings
The patient was diagnosed with pre-extensively drug-resistant pulmonary tuberculosis using nucleic acid amplification and drug susceptibility testing.
A giant hydatid cyst was detected in the spleen through radiometric investigation.
The patient experienced multiple adverse drug reactions during treatment.
Abstract
Drug-resistant tuberculosis is a noteworthy threat to public health, especially in high-burden countries. Management of these types of tuberculosis is lengthy and associated with a number of adverse drug reactions. Pre-extensively drug-resistant tuberculosis is a serious type of disease that is caused by the strains of Mycobacterium tuberculosis that are resistant to either rifampicin or both, i.e., rifampicin and isoniazid, and resistant to any fluoroquinolones. A splenic hydatid cyst is relatively rare and has never been reported in a case of pre-extensively drug-resistant pulmonary tuberculosis. The present case is a rare case of a young Indian male who was diagnosed with pre-extensively drug-resistant pulmonary tuberculosis through a cartridge-based nucleic acid amplification test and second-line drug susceptibility testing. Further, a diagnostic radiometric investigation showed a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
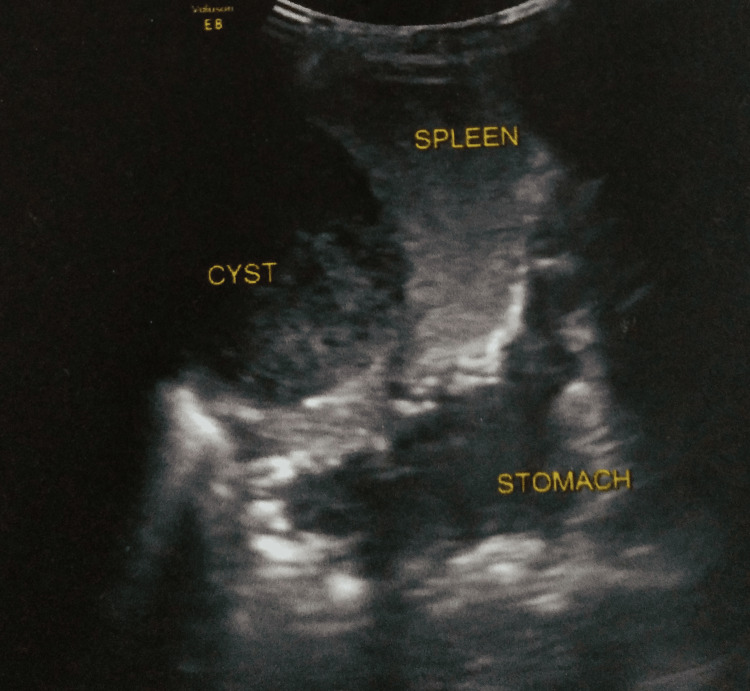 Figure 1
Figure 1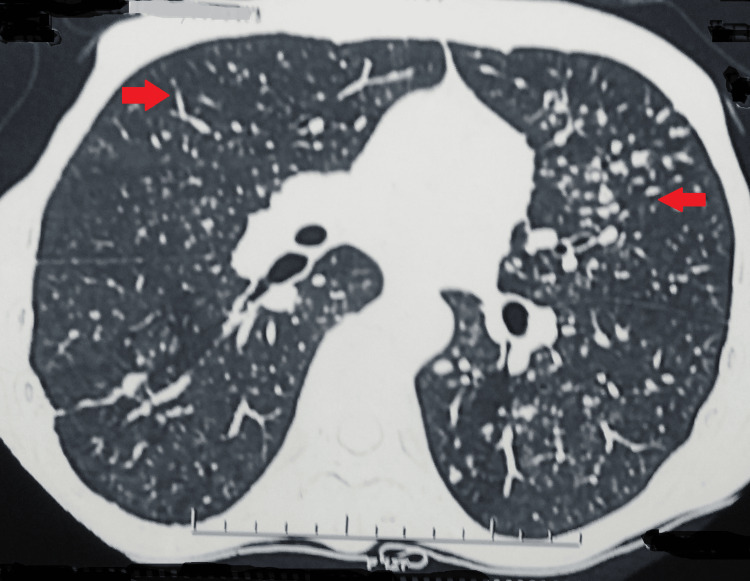 Figure 2
Figure 2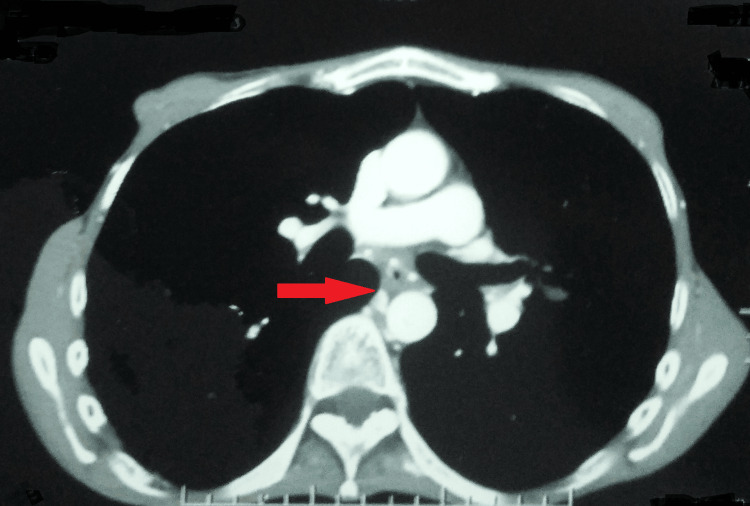 Figure 3
Figure 3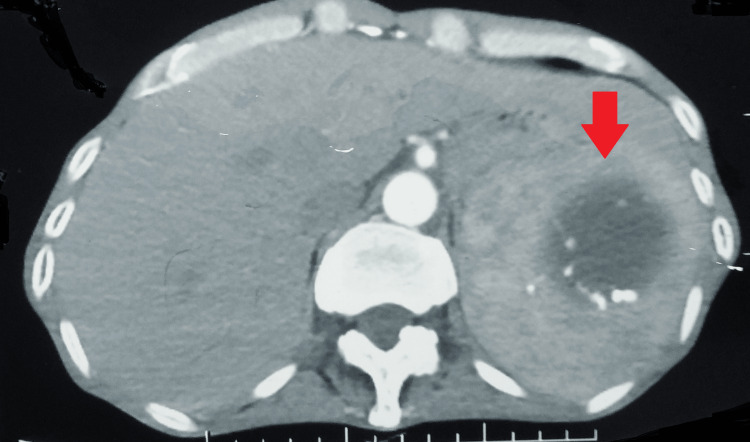 Figure 4
Figure 4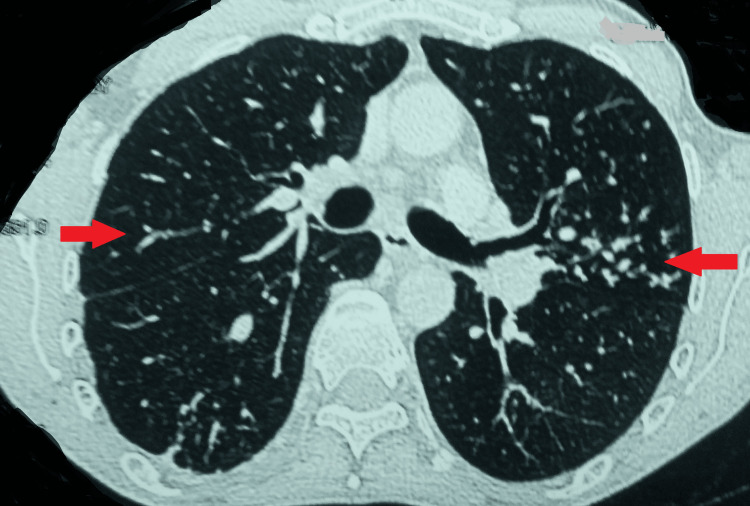 Figure 5
Figure 5 Figure 6
Figure 6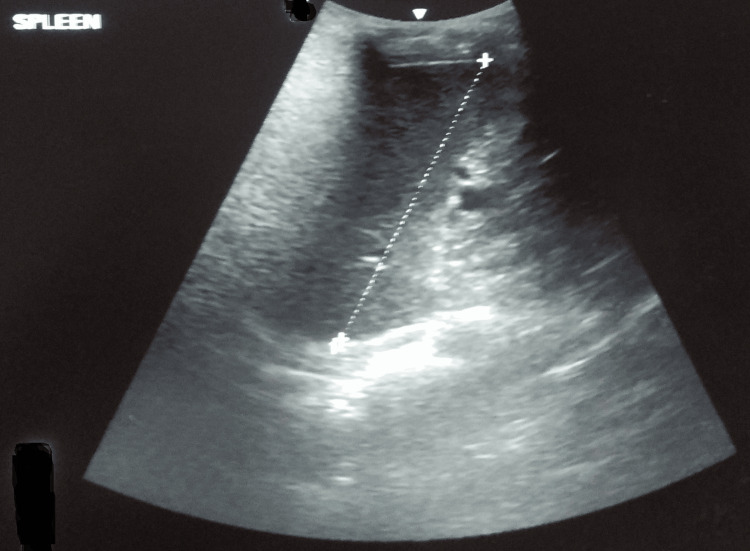 Figure 7
Figure 7| Test | Result | Reference range |
| Hemoglobin | 9.9 g/dL | 11.9-15 |
| Platelet count | 1.9 x 109/L | 1.5-4.0 x 109 |
| Total leukocyte count | 7.4 × 109/L | 4-10 |
| Erythrocyte sedimentation rate | 63 mm/hr | 0-20 |
| Bilirubin (conjugated) | 0.9 µmol/L | <1 |
| Human immunodeficiency virus | Non-reactive | Reactive-Non-reactive |
| Fasting blood sugar | 4.20 mmol/L | 3.9-5.6 |
| Serum electrolytes (Sodium, Potassium, Magnesium, and Calcium) | Normal | Normal-Abnormal |
| Serum creatinine | 55 µmol/L | 53-97.2 |
| Urine routine and microscopic | Normal | Normal-Abnormal |
| Serum thyroid-stimulating hormone levels | 0.5 mU/L | 0.4-4.0 |
| Serum uric acid | 3.7 | 3.5-7.2 mg/dL |
| Electrocardiogram | Normal (baseline QTcF-387 ms) | Normal-Abnormal |
| ELISA for detection of IgG antibodies for | Positive | Positive-Negative |
| Drug | Route of administration | Dose | Duration |
| Bedaquiline | PO | 400 mg X OD and then 200 mg AD | 24 weeks (2+22) |
| Linezolid | PO | 600 mg X OD, followed by 300 mg X OD | 18 months (6+12) but replaced with delamanid 100 mg X BD at the sixth month |
| High-dose moxifloxacin | PO | 600 mg X OD | 540 days |
| Clofazimine | PO | 100 mg X OD | 540 days |
| Cycloserine | PO | 500 mg X OD | 540 days |
| Pyridoxine | PO | 100 mg X OD | 540 days |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Amoebic Infections and Treatments · Parasites and Host Interactions
Introduction
In high-burden countries like India, public health is at risk because of infectious diseases like tuberculosis [1]. In recent years, there has been a significant increase in the number of tuberculosis cases. This could be attributed to a more streamlined notification and monitoring of the program. Nonetheless, the incidence and prevalence of tuberculosis remain at 188 and 312 per 0.1 million people, respectively, even with such vigilante measures [2].
A significant challenge with tuberculosis control is drug-resistant tuberculosis. Recent years have witnessed an increase in the overall number of drug-resistant tuberculosis cases [3]. Drug-resistant tuberculosis falls into four groups: isoniazid-resistant tuberculosis, pre-extensively drug-resistant tuberculosis, multi-drug-resistant/rifampicin-resistant tuberculosis, and extensively drug-resistant tuberculosis [4].
Pre-extensively drug-resistant tuberculosis is now defined as tuberculosis caused by strains of Mycobacterium tuberculosis that meet the criteria for both multidrug-resistant and rifampicin-resistant tuberculosis, as well as resistance to any fluoroquinolone [5]. Per the India TB Report 2023, about 2,411 cases out of 10,143 samples were of pre-extensively drug-resistant tuberculosis. Besides, about 93% of these cases were initiated on treatment [4].
A splenic hydatid cyst, a result of infection by *Echinococcus granulosus *larvae, is an infrequent condition, with less than 3% of cases reported even in endemic countries. It is often associated with vague symptoms, which makes its diagnosis challenging [6].
The simultaneous occurrence of a splenic hydatid cyst with pre-extensively drug-resistant pulmonary tuberculosis makes it difficult to diagnose and manage the situation. Herein, the case of a 41-year-old Indian male is described. He presented with complaints of fever, cough, abdominal pain, and loss of appetite. A diagnosis of pre-extensively drug-resistant pulmonary tuberculosis with a splenic hydatid cyst was made, and treatment was initiated.
Case presentation
A 41-year-old Indian man from a low socioeconomic background reported fever, cough with expectoration, abdominal pain, and appetite loss in 2022. He was asymptomatic two weeks prior, and then he had a low-grade evening-rise fever without chills or rigors. Further, he had a cough with yellow-colored expectoration for one week, which was continuous, non-blood-tinged, and not associated with any aggravating or relieving factors. He also reported intermittent left-sided abdominal pain that was insidious in onset for two weeks. Furthermore, there was a loss of appetite; however, there was no significant weight loss.
No prior history of trauma, convulsions, or unusual weight loss was present. He was a delivery boy with a history of working on farms. Also, he had a history of tuberculosis twice in the past (the first episode of drug-sensitive pulmonary tuberculosis in 2002 with a treatment outcome as cured and the second in 2008, which was also drug-sensitive pulmonary tuberculosis with a treatment outcome as cured). There was no record of migration, abuse of drugs, imprisonment, camp stays for refugees, or night shelter stays. Furthermore, there was no prior surgical history.
A general examination revealed a 98.6 °F temperature, 79 beats per minute pulse, 110/80 mmHg blood pressure, 17 breaths per minute respiratory rate, 68 kg weight, and 99% oxygen saturation (SpO_2_) on room air. His systemic examination was remarkable for bilateral crackles on auscultation. Additionally, the abdominal examination was remarkable for tenderness in the left hypochondrium; however, no visceromegaly was noted on palpation. Moreover, clubbing, icterus, cyanosis, pallor, koilonychia, and lymphadenopathy were absent.
He underwent standard radiographic and blood investigations. The sputum fluorescent microscopy was positive (2+) for Mycobacterium tuberculosis. This was further confirmed as drug-resistant tuberculosis with low detection of Mycobacterium tuberculosis with resistance to rifampicin on a cartridge-based nucleic acid amplification test (CBNAAT).
Ultrasonography of the abdomen revealed a well-defined, fairly thick-walled cystic lesion measuring 66 x 73 x 59 cm in the spleen. It showed coarse echoes and curvilinear calcifications in the wall (Figure 1).
USG of the abdomen showing a well-defined cystic lesionUSG: ultrasonography
Further, the patient complained of hemoptysis (10-15 ml per episode); hence, a computed tomography pulmonary angiogram was performed, which was suggestive of multiple centrilobular nodules of varying sizes scattered in bilateral lung parenchyma, with many of them showing a tree-in-bud appearance (Figure 2).
Computed tomography pulmonary angiogram showing bilateral involvement of the lungs
There were hypertrophied and tortuous common bronchial, 5th, 6th, and 7th intercostal arteries. A well-defined fluid-attenuating cystic lesion with peripheral wall calcifications was seen in the spleen, likely a hydatid cyst (Figures 3, 4).
Computed tomography pulmonary angiogram suggestive of hypertrophied and tortuous bronchial artery
Computed tomography of the lungs showing a well-defined fluid-attenuating cystic lesion with peripheral wall calcifications in the spleen
Meanwhile, reports of second-line drug-susceptibility testing were suggestive of fluoroquinolone resistance (low). Hence, a final diagnosis of pre-extensively drug-resistant pulmonary tuberculosis with a primary splenic hydatid cyst was made, and he was advised a pre-treatment evaluation (Table 1).
As his pre-treatment evaluation was within the reference range, a weight-based all-oral longer regimen per the national guidelines was initiated (Table 2).
For the splenic hydatid cyst, he was referred to the surgeon who advised a splenectomy but the patient refused the same. He was on medical management with tablet albendazole. A review by the nodal drug-resistant tuberculosis center stated that the splenectomy could be offered post-completion of his all-oral, longer treatment.
He continued his treatment with occasional episodes of adverse drug reactions like a raise in corrected QT interval by Fredericia (QTcF) (519 ms), which was promptly managed with a correction of the electrolytes. He also had linezolid-induced grade III paresthesia detected on the nerve conduction study, which was managed with the replacement of linezolid with delamanid at the sixth month.
A follow-up contrast-enhanced computed tomography of the chest at the completion of 18 months was suggestive of acute-on-chronic infective sequelae and revealed multiple discrete centrilobular nodules scattered in the bilateral lung parenchyma (left > right) many of them showing a tree-in-bud appearance. Multiple fibrocalcific nodules and fibroatelactic changes were also seen in the bilateral upper lobes. Note was made of a large hypodense cystic lesion of size 6.3 x 6.4 cm seen at the upper pole of the spleen, showing peripheral calcific foci, likely a hydatid cyst (Figures 5, 6).
A follow-up contrast-enhanced computed tomography of the chest suggestive of acute-on-chronic infective sequelae
Contrast-enhanced computed tomography showing a well-defined cyst in the spleen
As a result, his treatment was extended for two more months. Presently, he is on extended treatment with no fresh complaints. However, even after regular counseling, he is reluctant to go for surgical management of the hydatid cyst. He was monitored with regular ultrasonograms for the splenic cyst and the latest reports show a well-defined cystic lesion in the spleen (Figure 7).
Latest ultrasonography showing a well-defined cystic lesion in the spleen
Discussion
Drug-resistant tuberculosis is a big problem in achieving the goals of tuberculosis elimination in countries like India. It is widely reported that drug resistance is an outcome of man-made factors such as inadequate drug therapy, ignorance on the part of the prescribing physician or surgeon, difficulty acquiring drugs for low-income patients because of fiscal issues or social security, frequent shortages of second-line antituberculous drugs because of poor management and/or financial constraints, use of drugs or fixed drug combinations that contain unknown bioavailability of the drugs, lack of motivation at the beginning of treatment, and insufficient self-administration of drugs not being closely monitored during the intensive phase of therapy [7].
Diagnosis of pre-extensively drug-resistant tuberculosis is a challenging task, mainly due to the delay in the reporting of the patients at the health facilities. The National Tuberculosis Elimination Program of India is targeted at tuberculosis elimination, and the same is evident from the timely detection and initiation of management in the present case [8]. However, the treatment is lengthy and costly (in the private sector with exceptions), associated with a high pill burden, social stigma, adverse drug reactions, and a complex process that calls for the knowledge and abilities of a team that includes a counselor, a pulmonologist, and an expert in infectious diseases [3]. The primary approach is conservative, with management by second-line antituberculous medicines. In India, the World Health Organization recommends an all-oral-longer therapy [9]. But this management is associated with a large number of adverse drug reactions that are often asymptomatic, as seen in the present case, like the raised QTcF that was noted at the routine follow-up and the grade-III paraesthesia that was managed with the replacement of linezolid.
The prevalence of a splenic hydatid, which is the third most typical location for Echinococcus, is 0.5-4% worldwide. Iran has the highest incidence (4%). Hydatid cysts are nearly the only type of parasitic splenic cysts, with about 50-80% of splenic cysts in endemic locations being echinococcal. Reports of splenic hydatidosis date back thousands of years [10]. The first person to report splenic hydatidosis as an autopsy finding was Berlot in 1790. A splenic hydatid cyst could be either primary (isolated to the spleen only) or secondary (accompanied by hydatid cysts in other organs). Primary splenic hydatid cysts are extremely rare and reported in less than 2% of patients [11]. It could be detected accidentally or manifest as vague symptoms. It is native to countries in South America, Africa, the Middle East, South Europe, India, and Australia that raise cattle. The management is mainly surgical, with splenectomy [10]. Large cysts can rupture, causing life-threatening conditions like abdominal pain, urticaria, anaphylaxis, and sudden death [12]. However, in asymptomatic cases or where symptoms are not remarkable, convincing patients for surgery is an arduous task.
Cases of hydatid cysts of the lung with tuberculosis are reported in the literature, but a detailed literature search revealed that a primary splenic hydatid cyst in a pre-extensively drug-resistant pulmonary tuberculosis case is never reported.
Although this is only one such report, it is essential that clinicians report such rare presentations, especially from high-burden countries. This will not only help in knowledge dissemination but will also aid in making or modifying the existing treatment protocols.
Conclusions
A case of pre-extensively drug-resistant pulmonary tuberculosis with a splenic hydatid cyst has not been reported before to the best of this author's knowledge.
This case emphasizes the need for a detailed workup, as was done in this case, where the hydatid cyst was diagnosed promptly. However, this case also highlighted the importance of counseling and monitoring for adverse drug reactions, which could be asymptomatic at times. Additionally, cases with such rare presentations are infrequently seen even in endemic countries, which stresses periodic training and dissemination of information about these cases so that fatal outcomes due to diagnostic delays can be avoided.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Multidrug-resistant tuberculosis of the spine with bilateral psoas and pre- and paravertebral abscesses in an immunocompetent Indian female with multiple adverse drug reactions: the world’s first report Cureus Yadav S 016202410.7759/cureus.51835 PMC 1084789738327909 · doi ↗ · pubmed ↗
- 2Global tuberculosis report 2021. WHO 2 2024 2021 Global tuberculosis report 2024 https://www.who.int/publications/i/item/9789240037021
- 3Primary disseminated pre-extensively drug-resistant tuberculosis of the lungs, pleura, chest wall, and abdomen: the world's first case Cureus Yadav S 015202310.7759/cureus.42281 PMC 1044039837609098 · doi ↗ · pubmed ↗
- 4India TB Report 2023 2 2024 2023 https://tbcindia.gov.in/showfile.php?lid=3680
- 5WHO announces updated definitions of extensively drug-resistant tuberculosis 2 2024 2021 https://www.who.int/news/item/27-01-2021-who-announces-updated-definitions-of-extensively-drug-resistant-tuberculosis
- 6Splenic hydatid cyst Can J Surg Karabicak I Yurtseven I Yuruker SS Ozen N Kesim M 010522009 https://pubmed.ncbi.nlm.nih.gov/19865563/PMC 276912819865563 · pubmed ↗
- 7Multidrug-resistant tuberculosis of the spine--is it the beginning of the end? A study of twenty-five culture proven multidrug-resistant tuberculosis spine patients Spine (Phila Pa 1976) Pawar UM Kundnani V Agashe V Nene A Nene A 01034200910.1097/BRS.0b 013e 3181 af 779719829244 · doi ↗ · pubmed ↗
- 8National strategic plan for tuberculosis elimination 2017-2025 2 2024 2017 https://tbcindia.gov.in/Write Read Data/NSP%20Draft%2020.02.2017%201.pdf