Spectrum of myocardial involvement in patients with COVID-19 – An echocardiography study
Manoj kumar Dubey, Avinash Mani, Vineeta Ojha

TL;DR
This study identifies specific heart muscle changes in COVID-19 patients using echocardiography, aiding in the diagnosis of heart involvement.
Contribution
The study reveals a unique pattern of myocardial dysfunction in COVID-19 patients detectable via echocardiography.
Findings
Echocardiography showed hypokinesia of anterolateral and apical segments in all patients.
Strain-derived ejection fraction was lower in four-chamber views, indicating regional dysfunction.
Reduced global longitudinal strain with normal ejection fraction suggests global systolic impairment.
Abstract
Covid-19 patients can have both regional and global ventricular dysfunction. We aim to study the spectrum of myocardial involvement in Covid-19 patients on echocardiography. This is a single center, observational study where wall motion abnormality patterns were studied in Covid-19 patients along with global and regional longitudinal strain analysis (GLS). 30 Covid-19 patients were included in the study, with a mean age of 35.3±6.4 years. Echocardiography revealed characteristic wall motion abnormality involving hypokinesia of anterolateral and apical segments, which produced an operculum like appearance in all patients. Strain derived ejection fraction(EF) was lower in 4 chamber as compared to 2 chamber indicating regional myocardial dysfunction. Reduced GLS values in presence of normal EF indicates global systolic function impairment. Endocardial effacement was also noted in these…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
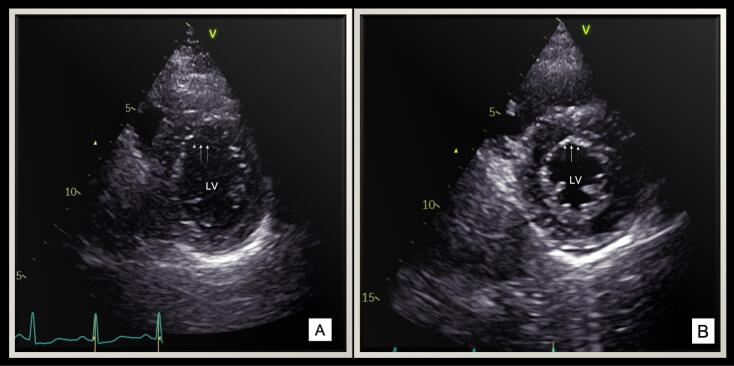 Figure 1
Figure 1|
|
|
| Age, years | 35.3 ± 6.4 |
| Females | 14 (45) |
| Diabetes | 0 |
| Hypertension | 0 |
| Dyslipidemia | 0 |
| Smoker | 0 |
| Symptoms | |
| Asymptomatic | 5(15) |
| Fever | 11(35) |
| Chest pain | 9(30) |
| Dyspnea | 3(10) |
| Palpitations | 2(6.6) |
| Cough | 2(6.6) |
| Spo2, % | 96.8 ± 0.9 |
| Rhythm abnormalities | |
| Normal sinus rhythm | 15(50) |
| Sinus tachycardia | 10(33) |
| Sinus bradycardia | 3(10) |
| Atrial fibrillation | 2(7) |
| ST/T changes on ECG | 12(40) |
| IL-6, pg/ml | 11.4 ± 1.75 |
| D-dimer, ng/ml | 0.59 ± 0.14 |
| Serum CRP, mg/L | 10 ± 2.23 |
| Serum Ferritin, ng/ml | 1343.3 ± 33.6 |
|
|
|
| LV internal dimension diastole, mm | 44 ± 3.7 |
| LV internal dimension systole, mm | 30.3 ± 3.6 |
| LV ejection fraction (M-mode), % | 58.3 ± 6.7 |
| LV ejection fraction (4 CH), % | 55.5 ± 4.1 |
| LV ejection fraction (2CH), % | 58.7 ± 4.7 |
| Wall thickness, mm | 8.7 ± 1.1 |
| Wall motion abnormality, % | |
| Anteroseptal | 14(45) |
| Anterior (basal) | 16(53) |
| Anterolateral | 30(100) |
| Inferoseptal | 2(6.6) |
| Inferior (Basal) | 0 |
| Inferolateral | 0 |
| Anterior (apex) | 30(100) |
| Septal (apex) | 30 (100) |
| Inferior (apex) | 0 |
| Lateral (apex) | 30(100) |
| RV systolic pressure, mmHg | 14.8 ± 3.9 |
| TAPSE, mm | 18.5 ± 2.1 |
| RV FAC, % | 46.2 ± 4.4 |
| Diastolic dysfunction, % | 6 (20) |
| Intracardiac thrombus, % | 0 |
|
|
|
| Mean global longitudinal strain (GLS) | - 17.2 ± 1.97 |
| Patients with reduced GLS | 14 (45) |
| Average number of segments with reduced longitudinal strain | 3.4 ± 1.8 |
| Mean LS in affected segments | -10.5 ± 2.3 |
| Segments with reduced longitudinal strain, % | |
| Anteroseptal | 12 (40) |
| Anterolateral | 18 (60) |
| Inferoseptal | 0 |
| Inferolateral | 0 |
| Anterior | 27 (90) |
| Inferior | 0 |
| Septal | 2 (6.6) |
| Lateral | 21 (70) |
| Number of segments with increased PSI | 2.3 ± 1.2 |
| Segments with increased PSI, % | |
| Anteroseptal | 5 (15) |
| Anterolateral | 21 (70) |
| Inferoseptal | 0 |
| Inferolateral | 0 |
| Anterior | 24 (80) |
| Inferior | 0 |
| Septal | 0 |
| Lateral | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Cardiovascular Effects of Exercise · COVID-19 Clinical Research Studies
Introduction
Cardiovascular involvement has been well documented in COVID-19 patients. The clinical presentation can include acute coronary syndrome, myocarditis, heart failure, ventricular arrhythmias and pericardial effusion.^1,2^ Myocarditis in Covid-19 patients is attributed to direct myocardial injury and immune mediated damage, with clinical presentation ranging from mild troponin elevation to decompensated heart failure.^3,4^ Cardiovascular magnetic resonance (CMR) imaging is considered as the gold standard for the diagnosis of myocarditis using the Lake Louis criteria.^5^ However, the lack of easy availability of CMR remains a major hurdle and highlights the importance of echocardiography in decision making.
2D echocardiography in Covid-19 patients has revealed left ventricular dysfunction along with wall motion abnormalities.^6^ Right ventricular dysfunction is also noted in a quarter of patients. Patients with myocarditis can have a dilated ventricle with either global or segmental abnormalities.^7^ No specific myocardial involvement pattern has been identified in Covid-19 patients. Establishing causal relationship between myocardial involvement and Covid-19 may be difficult using echocardiographic alone. In the current study, we aimed to identify specific myocardial involvement patterns in Covid-19 patients. Identification of specific patterns can help establish echocardiography as a sensitive diagnostic modality for identifying Covid heart.
Materials and Methods
This was a prospective, observational study done at a tertiary care center, over a period of 6 months from January 2021 to June 2021. Covid-19 patients, diagnosed using positive RT-PCR and ECG changes were included in the study. Patients with severe Covid-19 and multisystem organ involvement were excluded from the study. All patients underwent transthoracic echocardiogram using Vivid T8 (GE Healthcare systems, Chicago, USA). Left and right ventricular function were assessed along with LV strain analysis(AFI). Post systolic strain index (PSI) was also calculated from strain analysis.
All data was recorded in a tabular format and presented as summary statistics. Student’s t-test was used to estimate significant difference between ejection fractions measured in 4 chamber and 2 chamber. Pearson correlation analysis was done to determine association between longitudinal strain and PSI. A p value of < 0.05 was considered as significant.
Results
A total of 30 patients were included in this study. The mean age of the study population was 35.3 ± 6.4 years (range 14-50 years) and females comprised 45% of the study population. Fever and chest pain were the most common symptoms noted (35% and 30% respectively) (Table 1). All patients had elevated biomarkers in the study population which shows the prevalent pro-inflammatory state in these patients (Table 1). Half of the study group had rhythm abnormalities in the form of sinus tachycardia (n = 10), sinus bradycardia (n = 3) and atrial fibrillation (n = 2).
Echocardiography revealed normal sized left ventricle and preserved systolic function with a mean M-mode ejection fraction (EF) of 58.3 ± 6.7% in the study group. However, strain derived auto EF was significantly lower in 4 chamber (4C) as compared to 2 chamber(2C) (58.7 ± 4.7% vs 55.5 ± 4.1%, P = 0.002). This points towards the presence of regional myocardial dysfunction in these patients. All patients had myocardial involvement in the form of hypokinesia predominantly involving anterolateral, apicoseptal and apicolateral segments as compared to other segments (Figure 1 A, Table 2).
**
This characteristics wall motion abnormality produces an “operculum” like appearance over the other segments in the short axis view in systole (Figure 1B, Supplementary Video 1). Endothelial involvement was characterized by predominant involvement of interventricular septum (IVS) producing a characteristic jerky motion and stretching of IVS.
Global longitudinal strain (GLS) was reduced in 45% of the study population (Table 3). The anterior and apicoseptal segments had maximum reduction in longitudinal strain values amongst all patients. Peak systolic index was elevated in the involved segments indicating contractile abnormalities. A high degree of correlation was seen between regional longitudinal strain and segmental PSI, demonstrating impaired systolic contraction in the affected segments (r = 0.702, P = 0.001). No gender difference in GLS values were noted in the study population (P = 0.237).
Discussion
The current study intended to evaluate the spectrum of myocardial involvement in Covid-19 patients using echocardiography. Echocardiography revealed reduced global ventricular function as demonstrated by reduced GLS in about half of the study population. All patients had a characteristic wall motion abnormality producing an operculum like appearance in systolic frames. There was predominant involvement of anterior and apical segments as compared to other segments leading to reduced strain derived 4C ejection fraction. Endothelial involvement was noted along with elevated PSI values. To our knowledge, this is the first study which aims to study myocardial involvement pattern noted in Covid-19 patients.
Echocardiography is an invaluable and easily accessible tool for diagnosis of Covid-19 associated myocarditis. Echocardiographic findings in Covid-19 patients were evaluated in a large study conducted by Dweck et al.^6^ Left ventricular abnormalities were noted in 39% patients whereas myocarditis was seen in 3%. In our cohort, patients had global ventricular dysfunction as evidenced by reduced GLS as well as regional predilection as evidenced by characteristic motion abnormalities noted in anterolateral and apical segments. Regional involvement in Covid-19 patients has been documented, ranging from basal and mid ventricular involvement to limited hypokinesia of inferior/inferoseptal segment.^8^ A systematic review of cardiac MRI in 199 Covid-19 patients revealed that global hypokinesia was the most common myocardial involvement pattern in these patients.^9^ On the contrary, our study patients had hypokinesia involving anterolateral and apical segments, giving the appearance of an operculum. This was coupled with effacement of the endocardial lining in these segments and stretching of IVS. This characteristic pattern noted in our patients is a unique one, which has not been described before in Covid-19 patients.
Global longitudinal strain is a sensitive marker for myocardial dysfunction. Echocardiographic evaluation of hospitalized Covid-19 patients revealed that global longitudinal strain was reduced in patients with preserved LV ejection fraction, as noted in our patients.^10^ PSI analysis is also a surrogate marker for evaluation of ventricular dysfunction. Longitudinal strain values were reduced in the involved segments whereas PSI values were elevated, signifying regional myocardial dysfunction. Covid-19 infection has been postulated to cause coronary microvascular dysfunction (CMD) which can lead to subendocardial ischemia. Subendocardial perfusion defects have been demonstrated in patients with history of Covid-19 infection using cardiac MRI.^11^ CMD could be the probable cause for wall motion abnormalities and endocardial effacement noted in our patients. Coronary microvascular dysfunction may cause global wall motion abnormalities which slowly recovers over time. The rate of recovery can be variable for individual segments, with anterior and apical segments showing slower recovery as compared to others, thus producing the characteristic appearance on echocardiogram. Newer evidence pertaining to disturbance of regional perfusion instead of global perfusion, post severe Covid-19 infection is emerging.^12^ Follow up studies need to be undertaken to determine the long-term impact of Covid-19 on myocardium, regarding the reversibility of initial changes.
The current study has its inherent limitations. The small sample size prohibits us from generalizing the results to the entire spectrum of Covid-19 patients. CMR imaging could not be performed in these patients due to lack of availability and financial constraints. As this was a single center hospital-based study, selection bias could have influenced the results, with sicker patients being excluded from the analysis.
Conclusion
Covid-19 patients have global as well as regional myocardial dysfunction. Specific echocardiographic pattern can help identify myocardial involvement in Covid-19 patients. Echocardiography should be considered the modality of choice in such situations.
Competing Interests
None of the authors have any conflict of interests
Ethical Approval
Ethics approval was obtained from the Institutional ethics committee (IEC/2021-167) and informed consent obtained from the participants.
Funding
None.
Supplementary Files
Supplementary video 1. Echocardiographic clip of short axis view at mid ventricular level shows hypokinesia of anterior and anterolateral segments, producing an operculum like appearance. Rest all segments are contracting normally.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Inciardi RM Lupi L Zaccone G Italia L Raffo M Tomasoni D Cardiac involvement in a patient with coronavirus disease 2019 (COVID-19)JAMA Cardiol 2020578192410.1001/jamacardio.2020.109632219357 PMC 7364333 · doi ↗ · pubmed ↗
- 2Bangalore S Sharma A Slotwiner A Yatskar L Harari R Shah B ST-segment elevation in patients with COVID-19 - a case series N Engl J Med 20203822524788010.1056/NEJ Mc 200902032302081 PMC 7182015 · doi ↗ · pubmed ↗
- 3Oudit GY Kassiri Z Jiang C Liu PP Poutanen SM Penninger JM SARS-coronavirus modulation of myocardial ACE 2 expression and inflammation in patients with SARS Eur J Clin Invest 20093976182510.1111/j.1365-2362.2009.02153.x 19453650 PMC 7163766 · doi ↗ · pubmed ↗
- 4Guo T Fan Y Chen M Wu X Zhang L He T Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19)JAMA Cardiol 202057811810.1001/jamacardio.2020.101732219356 PMC 7101506 · doi ↗ · pubmed ↗
- 5Friedrich MG Sechtem U Schulz-Menger J Holmvang G Alakija P Cooper LT Cardiovascular magnetic resonance in myocarditis: a JACC white paper J Am Coll Cardiol 2009531714758710.1016/j.jacc.2009.02.00719389557 PMC 2743893 · doi ↗ · pubmed ↗
- 6Dweck MR Bularga A Hahn RT Bing R Lee KK Chapman AR Global evaluation of echocardiography in patients with COVID-19Eur Heart J Cardiovasc Imaging 20202199495810.1093/ehjci/jeaa 17832556199 PMC 7337658 · doi ↗ · pubmed ↗
- 7Felker GM Boehmer JP Hruban RH Hutchins GM Kasper EK Baughman KL Echocardiographic findings in fulminant and acute myocarditis J Am Coll Cardiol 20003612273210.1016/s 0735-1097(00)00690-210898439 · doi ↗ · pubmed ↗
- 8Krishna H Ryu AJ Scott CG Mandale DR Naqvi TZ Pellikka PA Cardiac abnormalities in COVID-19 and relationship to outcome Mayo Clin Proc 20219649324210.1016/j.mayocp.2021.01.00633714597 PMC 7816643 · doi ↗ · pubmed ↗