Psychiatrists’ Illustration of Awe in Empathic Listening Assessments: A Pilot Study
Parameshwaran Ramakrishnan, Thomas M Brod, Thomas Lowder, Prasad R Padala

TL;DR
This pilot study explores how psychiatrists experience awe during empathic listening sessions with patients, revealing themes of mindfulness and transcendence.
Contribution
The study introduces an evidence-based framework for examining awe and non-agency in empathic listening within psychiatry.
Findings
Awe and non-agency were consistently observed in both psychiatrists and patients during empathic listening assessments.
Themes of mindfulness and transpersonal mindfulness emerged from the analysis of verbal and nonverbal interactions.
The findings suggest a 'mindfulness-to-transcendence' framework for studying transcendence in psychiatry.
Abstract
Background “Awe” is typically an inspiring emotional response to perceptually vast stimuli signifying the transcendence beyond all cognitive frames of reference when we encounter the unexpected. Physicians’ experience of awe in clinical care interactions has not been studied in an empirical, evidence-based way. We aim to present a focused study of awe in a psychiatrist’s empathic listening (EL) assessments and propose an evidence-based framework to study it. Methodology This is an exploratory case series of a psychiatrist’s EL interactions (mean duration/x̄ of 46.17 minutes) with six patients (two males and four females) aged 32-72 years (x̄ =54.67, σ = 16.64). Using the method of autoethnography, the verbal and nonverbal aspects of the EL assessments were analyzed and open-coded to generate qualitative data. Results The study revealed that the data in all the case studies could be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
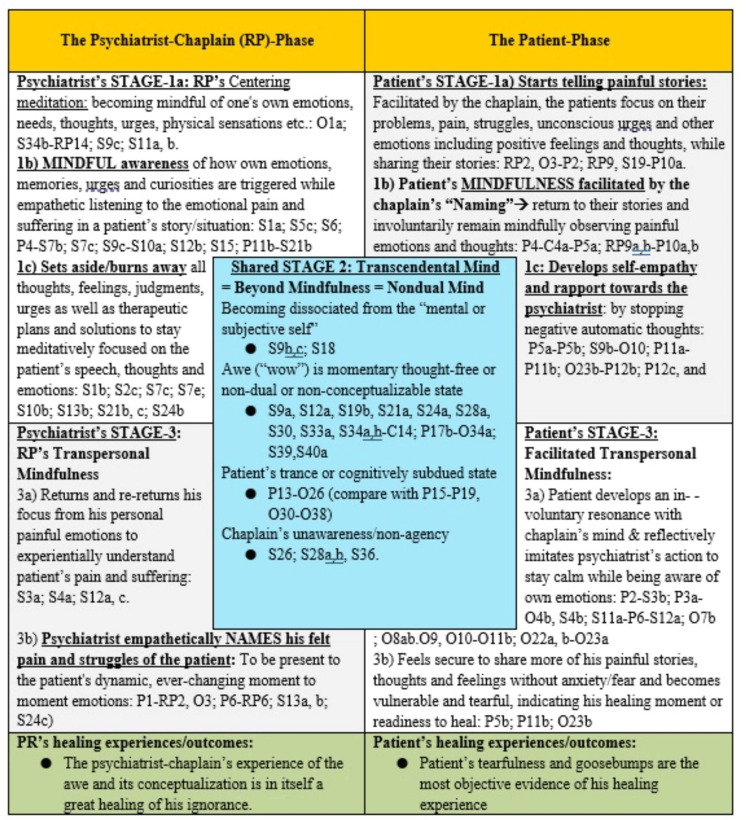 Figure 1
Figure 1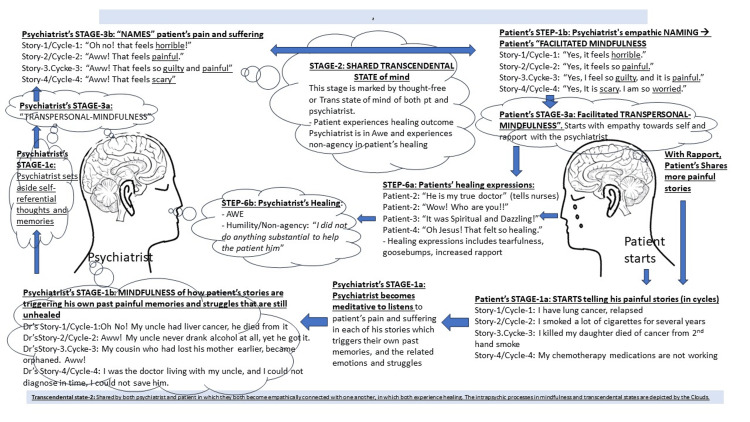 Figure 2
Figure 2| Participant | Age (years)/Gender | Diagnosis | Visit duration | Hospital setting | EL assessment outcomes: -Psychiatrist’s unawareness/non-agency in patient’s healing (before patient’s own revelation). -Awe experience after witnessing the patient’s healing outcome and feedback |
| Patient 1 | 70/Male | MDD | 45 minutes | In-patient | Non-agency: “Wow! How did the patient feel healed! I did not provide any substantial care to this patient!” Awe experience: “I woke up with my feet 6 feet above the ground.” “This is my real doctor” |
| Patient 2 | 68/Male | PTSD, MDD | 60 minutes | In-patient | Non-agency: “What could I have done better to feet healed? Awe experience: The patient broke down into tears, revealed goosebumps, and reported a calming effect while describing the visit as “Spiritual” and “dazzling.” |
| Patient 3 | 32/Female | Schizophrenia | 22 minutes | In-patient | Non-agency/Unaware: “What did I do for this profound rapport?” Awe experience: addressing the psychiatrist/RP as “Hello Jesus.” |
| Patient 4 | 34/Female | GAD, MDD | 60 minutes | Out-patient | Non-agency: Unaware of the patient’s healing transformation. Awe experience: Witnessing sheer happiness in the patient |
| Patient 5 | 52/Female | MDD | 60 minutes | Out-patient | Non-agency: Unaware of patient’s healing transformation. Awe experience: “My mother said, why are you going to a psychiatrist? Go and talk to Jesus about your troubles.” “I think I have come to the right place.” |
| Patient-6 | 72/Female | PTSD, MDD | 30 minutes | In-patient | Non-agency: Unawareness of patient’s healing transformation. Awe experience: “Ah! that felt like God’s touch.” |
| Events | Description of codable events | The codes: Each event and related subevents are coded sequentially and uniquely, using letters and numbers |
| Observable speech | Verbal statements uttered by RP as the psychiatrist during his EL care assessment. Verbal and nonverbal statements (silent pauses) uttered by the patients (P) | Each statement of RP and his patient (P) are coded in sequence and assigned to the individual speaker as follows: coded as RP1, RP2, RP3, etc. Coded as P1, P2, P3, etc. |
| Observable behavior | These are RP’s observations (as the participant-researcher) of the patient and the self. The observations corresponding to each verbal interaction can be subtyped into (a) facial or emotional expressions, (b) body language, and (c) other behaviors | The observations (with the subtypes) of behaviors corresponding to each verbal interaction of the EL process are coded as follows: O1a, O1b, O1c, etc. O2a, O2b, O2c, etc. |
| Subjective thoughts and feelings | These are RP’s (self-reflective) subjective observations of his cognitive and emotive (intrapsychic) processes corresponding to each of the verbal/nonverbal interactions. They are subtyped into (a) those that refer to RP’s self, triggered by the patient’s statements or behavior; (b) how they informed RP about the patient; (c) what does RP do with those thoughts and emotions | These subjective observations with subtyped are coded as follows: S1a, S1b, S2c, S1d, etc. S2a, S2b, S2c, S2d, etc. S3a, S4b, S3c, S3d, etc. S4a, S4b, S4c, S4d, etc. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedia Influence and Health · Communication in Education and Healthcare · Film in Education and Therapy
Introduction
Physicians have reportedly felt amazed at witnessing unexpected healing outcomes of their patients through their empathic listening (EL) interactions [1]. Such amazement in clinical healing outcomes has been identified as “awe” by physicians as well as patients [2]. Because of the lack of a conceptual understanding of how their patients could have felt healed in their EL process, physicians have self-described them as “magical” [3,4]. In clinical care, those “magical” EL moments occur unannounced and in uncharted ways amid the routine or mundane actions that clinicians perform, such as recording height and weight, assessing blood pressure, prescribing medications, and asking patients to complete validated questionnaires [3]. While witnessing sheer happiness in their patients, physicians may say, “I don’t know why; I didn’t do anything” (i.e., a feeling of “non-agency”) and the patient may merely say “Well. She listened” [3]. The word “listening” in this context refers to the psychiatrist/physician’s ability to empathize deeply with the feelings of pain and suffering that underlie the patient’s spoken and unspoken words. In this sense, the physician’s “empathic listening” is his/her “presence” or “just being there” with the patient’s pain and suffering [4,5].
Contrasting the lack of EL training in medical school or residency education, the clinical chaplains are trained [6] to intentionally use EL as their primary clinical care tool for transmitting and transmuting “awe” [7]. Clinical chaplains may refer to their process of EL and being present to patients’ pain and suffering as the “companioning the bereaved” model of care [8]. In their EL care, chaplains too have reported feelings of “providing nothing” (i.e., a feeling of “non-agency”) to their patients though they witness amazing healing outcomes among their patients [9]. Thus, the feelings of awe and non-agency may be ubiquitous in EL-based clinical care interactions.
Currently, awe is also described as an “emotional response to perceptually vast stimuli that transcend current frames of reference” [10], and a sign of a cognitive-schema-free state of mind [11]. Researchers have identified neural representation/correlates of awe [12,13], and of non-agency, a (nonpathological) apathetic state in which one is free from the conceptual thought of being a doer/doing [14]. Though these emotions are widely experienced by physicians and therapists [1,2], evidence-based studies are limited. While physicians have described the awe-inspiring healing outcomes as “magical,” clinical chaplains understand awe as an experience of the “Divine presence” in their EL care [9,15,16]. As physicians educated and trained in analytical thinking, the onus is on us to conceptualize the framework of automatic transcendence into the “thought-free” “cognitive schema-free” or “self-less” state of mind that is brought through the EL process. In this study, we will use the term Transcendence as a proxy for the term “Divine” [9] to avoid the need to indulge in theological discussions, which is not the focus of this study.
This paper aims to present a systematic assessment of a psychiatrist’s emotional experience of awe and non-agency on witnessing the patients’ healing transformation during EL interactions with six patients. The objective is to understand how the emotions of awe, and non-agency, which are described to have neural correlates can fit into the current contemplative neuroscience/mindfulness-based framework of EL assessment [17-19] and help in advancing evidence-based studies.
We hypothesize that the emotions of awe and non-agency signify the transcendental (beyond mindfulness) state of mind attained automatically through the EL process, a mindful meditative approach to psychiatric assessment [17-19]. In that sense, the experiential and neuroscientific understandings of the transcendental state of mind signified by the emotions of “awe” and non-agency can be built into the current mindfulness-based framework of the EL assessment process.
Materials and methods
The study and its setting
This is an exploratory, retrospective study of six clinical case studies that met our inclusion and exclusion criteria. Three of the case studies were drawn from in-patient clinical chaplaincy settings at a tertiary care center in California. The other three case studies were drawn from psychiatric settings at a tertiary care medical center in Arkansas. Hospital guidelines were followed to eliminate the patient/participants’ identifiable privacy information. Inclusion criteria were patients over 18 years of age and older with a clinical diagnosis of mental disorder, and first contact with this researcher, RP. Minors (<18 years) may become suggestible during the EL interactions or resist the self-reflective or mindful-meditative process that EL interactions are supposed to facilitate. Hence, they were not included. Exclusion criteria were patients with acute psychosis and severe agitation, substance-related disorder in acutely intoxicated states, and any acutely ill neurological conditions, such as strokes and delirium. The University’s Institutional Review Board (IRB) was consulted, and the study was cleared as “not human subject research” and exempted from IRB approval.
Participants and materials
The first author of this paper (RP) is a psychiatrist who was also trained as a Clinical Chaplain in an Association of Clinical Pastoral Education (ACPE)-accredited Clinical Pastoral Education (CPE)/Spiritual Care residency program [6]. Clinical chaplains are trained in the art of EL, which is their primary assessment tool in the spiritual care process [17-19]. In this study, RP illustrates how EL care can be applied to psychiatric assessment for a better clinical outcome. The following are the summaries of the EL interactions between RP and his patients. The demographics, clinical care settings, duration of clinical interaction, and awe experience are listed in Table 1. The patients were aged between 32-72 years (mean age, x̄ = 54.67 years and SD/σ = 16.64), and the mean duration of clinical assessment was 46.17 minutes.
Case 1
A 70-year-old Caucasian male, a retired physician, had a history of major depressive disorder (MDD) and non-small-cell lung cancer (Stage III), status post-right upper lung lobe resection five years ago. His depression was treated with 10 mg of escitalopram daily. The chaplain/RP-patient encounter occurred on the fourth day of the patient’s hospitalization. He was admitted for persistent pneumonia in light of an early (Stage I) recurrence of lung cancer. The patient shared his pain and regret for smoking cigarettes for several decades, his pain and guilt that his daughter died of cancer from secondhand smoke, and his current fear that the “chemotherapy is not working.” At the end of a 45-minute EL interaction, the patient became tearful, requested a prayer, and ended the visit. After leaving the patient, RP started to feel that “I did not do anything substantive to help the patient.” RP felt that a good cognitive behavior therapy session would be more helpful than EL for the patient and decided to follow up. The next morning, on a follow-up visit (15 minutes), the patient eagerly waved his hand as soon as he saw RP entering the floor, introduced RP to his nephew, profusely thanked RP for the visit on the previous night, and said: “I woke up with my feet above the ground.” His nurse informed him that the patient had eaten his breakfast for the first time in four days. When RP was leaving the room, he overheard the patient telling his nephew “He is my real doctor” (the patient was unaware that RP was a psychiatrist). RP felt pleasantly shocked, “Wow! How did the patient feel healed? I thought I did not provide any substantive care to this patient!”
Case 2
A 68-year-old Caucasian male with a history of post-traumatic stress disorder (PTSD) and MDD was grieving the recent demise of his 72-year-old partner. His symptoms were treated with 20 mg of citalopram daily. RP was called for spiritual care services. RP identified the major conflict the patient was going through was honoring his partner’s wish for his body to be donated to the anatomy department and cremated. The patient’s four family members who were sitting around the bed with the dead partner requested RP to say a prayer. Before settling down to pray, RP facilitated each of the family members to share their memories and stories with the deceased person. During the prayer, RP lifted all the memories that each of the family members had shared. By the end of the prayer, every family member, except this patient, was in tears, indicating how they felt touched by the empathic and healing presence of their chaplain/RP. After completing the visit, this chaplain left wondering “What could I have done better to help the patient feel healed,” as that patient was not in tears like the rest of the family. However, RP later discovered that the patient remembered RP’s presence as “Spiritual” and “dazzling” (see Appendices for the supervisor’s hand-written note describing the patient’s experiences). On receiving the note and the supervisor’s feedback that the patient had revealed the goosebumps that he was still experiencing, and broke down into tears, RP was pleasantly surprised, “Wow! How did I not know about the patient’s healing!”
Case 3
A 32-year-old African American female with schizophrenia was admitted to the closed mental health unit (MHU) with a relapse of her paranoia and disorganized behavior. She was mute and withdrawn. The chaplain/RP was called (on a Friday) by the unit’s nurse supervisor to visit with the patient to just “smile and say a prayer” as the patient was seen holding on to her Bible and not interacting with any staff. EL process was attempted despite the patient remaining mute or answering in monosyllables. Through his EL process, RP too stayed silent, being mindful of his thoughts and emotions, and reflecting on his frustrations, current and past. He reflected on his past frustrations with catatonic patients. Becoming mindful of his ruminations, he made a self-reflective statement, “when we are preoccupied with our pain, frustrations, and struggles, we stay silent and not interact with people.” The patient became mindful with such a self-reflective statement, and she shared her fear/paranoia, though very minimally. Staying mindful of her transference and setting aside his discomfort, the chaplain offered a prayer and ended the visit, feeling embarrassed with the care he provided for the patient. On the third day, Monday, when he was consulted for yet another psychiatric patient, he entered the MHU, still feeling embarrassed of his previous visit with patient 3 and hoping that he would not come face-to-face with her. However, as soon as he entered the MHU, this patient who was standing at the other end of the long corridor caught his eyes, waved her hand, and loudly addressed him saying “Hello Jesus.” The chaplain felt shocked to hear being addressed in such a profound way. “Wow! What did I do for her to call me by that glorious name?!” was the chaplain-RP’s question.
Case 4
A 34-year-old Caucasian woman with a history of general anxiety disorder and MDD came to the clinic with worsening anxiety symptoms. During the session, the psychiatrist/RP maintained reflective questioning, facilitating the patient to share her stories. While elaborating on her depressing stories, she started to reveal her difficulties in her current relationship. As she paused a bit, the psychiatrist paused his note-taking and turned toward the patient and noticed her voice was choking with pain. At the end of that interaction, the patient cheered up. The psychiatrist turned back with a pleasant smile that revealed his surprise, a moment of Awe! The patient, who was looking straight and deeply into his eyes said, “Thank you for listening.”
Case 5
A 52-year-old Caucasian woman being treated for chronic insomnia was referred by her primary care physician as she was not comfortable prescribing Zolpidem anymore. The patient shared her troubles with chronic insomnia and that she needed Zolpidem. As the psychiatrist listened (EL) to her stories, she started to pour over the details of sadness in her life, and her symptoms met the diagnosis of recurrent MDD that had never been addressed. After becoming tearful over and again sharing her stories with her EL psychiatrist/RP, she looked deeply into the psychiatrist’s eyes and revealed “When I was leaving home to come to this clinic, my mother said, why are you going to a psychiatrist? Go and talk to Jesus about your troubles.” She paused and added, “I think I have come to the right place.” The psychiatrist did not expect that coming and had a “Wow” moment then. After a long discussion, she agreed to start taking mirtazapine for her sleep, depression, and appetite.
Case 6
A 72-year-old woman with a history of PTSD and recurrent MDD was admitted to the medical floor for treatment of her chronic obstructive lung disease. Psychiatry was consulted for depression and passive suicidal thoughts. On this psychiatrist/RP’s assessment, she shared symptoms that amounted to current MDD with a moderate degree of severity. She also kept returning to share her past traumas. On EL to her references to past PTSD, she became tearful and shared her ongoing trauma from her current boyfriend. Touched by the empathy received during the session she broke down crying. Her hands became tremulous, and she held the railings of her bed. The psychiatrist gently placed his palm on her hand which was holding the railing. She calmed down, opened her eyes with a pleasant smile, and said: “Wow! That felt like God’s touch.” Such an expression was unexpected, and an Awe-provoking moment for this psychiatrist. The patient paused and said, “Thanks for not judging me.”
The focus of study in each of the above case summaries is on (1) how, through the psychiatrist’s EL interactions, the patients had experienced healing in the form of their increased rapport, vulnerable tears, goosebumps, cheerful affect, and religious/spiritual emotions. Such changes in mood and affect, even temporarily, are considered signs of healing [20-22]. (2) How those healing transformations were unexpected by the psychiatrist-chaplain (RP), and how the awe moments transpire in him. Thus, RP studied his mental-emotional processes that transpired when he interacted with each of the patients included in this study. In that sense, he is a participant-researcher, and hence a study material himself. Such a methodology of studying one’s own mental-emotional self while studying the patients’ healing experiences is elaborated below.
Methodology
Evidence-based study of awe in EL clinical interaction is an inductive process. In that, we start with the results and go backward to inductively analyze the qualitative data drawn from the EL interaction process. As seen in the case summaries (Table 1), the patients’ healing expressions came in unexpected ways at the end of the EL interactions provoking awe in RP. While the patients were crediting RP for their healing, RP was wondering “How did that healing happen!” “Why is he crediting me?” “I did not provide any substantial care to this patient!” Such a feeling of having no role in patients’ healing, termed “non-agency” in this paper, has been reported by other EL physicians and chaplains as well [3,9]. These experiences of witnessing unexpected healing outcomes and the emotions of awe and non-agency become the signpost of evidence-based study of EL assessment.
The Mindfulness-Based Autoethnography Method of Studying Awe in EL Assessment
The study of one’s own behavior (including their thoughts and emotions) as they interact with people around them is called autoethnography, while the study of other individuals in an environment is ethnography [23]. A combination of methods of autoethnography and ethnography have been applied to study clinical chaplains’ EL/spiritual care assessments [24,25]. The autoethnographic study of clinical EL interactions includes two processes: First, the researcher/RP has to mindfully “zoom in” to observe the granular (“microscopic”) details of the subjective elements of own thoughts, feelings, intentions, urges, etc. These mindful observations of one’s intrapsychic world provoke self-empathy. Second, using wisdom and self-empathy, the researcher/RP would “zoom out” to mindfully observe how he interacts with the external world, the patient, and the clinical situation [17-19,26]. Thus, RP is a participant-researcher in this study.
Immediately after each patient visit, the EL care interactions were transcribed verbatim by RP using a contemporaneous note-taking methodology [17,18,24]. The granular details that are jotted down are of this psychiatrist/RP’s self-reflective observations of his and his patient’s speech and behavior, as well as his own intrapsychic processes, such as his thoughts, emotions, internal struggles, past painful memories, and urges that got triggered while listening to the patients’ stories [17-19,24,25].
The transcription itself is a mindful-meditative/self-reflective process, which includes (1) the psychiatrist’s mindful awareness of his thoughts and emotions that were getting triggered by the patient’s stories, (2) his struggles in staying non-judgmentally and empathetically present to the patient’s pain and struggles. Thus, the human “self” is the primary instrument of study in autoethnographic research [27]. Having a mindfulness-based framework of autoethnography is argued to lend itself to evidence-based contemplative neuroscientific studies [17,18]. Identifying the Aha/Wow, awe-inspiring moments that signify the transcendental mental state that transpires during their mindful-meditative process of the EL interaction is the key (signpost) to evidence-based studies on EL.
Open-Coding Method of Developing Qualitative Data for Inductive Analysis
EL interactions are methodical. To study these interactions, one needs to quantify the qualitative data. The qualitative data in the EL interaction includes the observable events such as the spoken and unspoken statements, facial expressions, body language, and physical interactions. In addition, because of the auto-analytical nature of its study, the qualitative data includes the metadata about the data provider/RP’s intrapsychic processes with which the qualitative data itself is produced. Thus, an autoethnographic study of the EL interaction is an epistemological process in which the participant-researchers would study/understand their own intrapsychic (thoughts and feelings) processes that are generating the data. The methodology of open coding for analyzing the qualitative data and the metadata to quantify them is described as epistemic network analysis (ENA) [28], and it has both human and machine-readable standards. The open-coding process, described in the past as grounded theory methodology [29], was typically based on human-readable standards, and it has been well-tested in studying EL assessments in the past [17-19]. Open coding enables us to study the seemingly disparate data sets amenable to be inductively analyzed and organized into a meaningful theoretical framework [30]. The open-coded qualitative data sets in this study were curated by human-readable standards that can be reproducible, enabling researchers to document their workflow, as well as organize their data in a format that is agnostic to software of any kind [28]. The open-coding method founded on human-readable standards is adopted and applied to code the qualitative data deductively and inductively. By deductive means the narrative corpus of the EL interaction was curated to produce three levels of abstraction: (1) verbatim statements of this researcher (RP) and his individual patients, including nonverbal expressions, such as silent pauses; (2) RP’s observations (O) as a participant-researcher; and (3) RP’s subjective (S) thoughts and feelings. The details of how these abstractions are developed into codable themes are presented in Table 2.
To illustrate how the EL interaction can be studied to identify the granular details that can be developed into themed abstractions that can be open-coded and analyzed, we are presenting the “Verbatim case report” of Case 1 (see Appendices).
Results
The granular details which are open-coded (see “Verbatim report” of Case 1, Table 3 in Appendices) can be developed into the following thematic groups: (1) psychiatrist’s mindfulness, (2) psychiatrist’s transpersonal mindfulness, (3) patient’s facilitated mindfulness, and (4) patient’s facilitated transpersonal mindfulness, which were consistent with the findings observed in previous studies [17,18]. The phenomena of awe and non-agency were classed into the fifth theme of transcendence. To understand how the phenomena of transcendence could be organized into the mindfulness-based framework of the EL process, we further analyzed the granular details of the EL interaction that related to RP’s emotional experiences, awe and non-agency (Table 3 in Appendices, Figure 1).
Tabular illustration of the mindfulness-to-transcendence framework of the empathic listening assessment process.The codes representing the verbatim statements of the first author (also the participant-researcher) RP and his patients and RP’s observations and subjective thoughts and feelings that got triggered in the empathic listening (EL) interaction have been elaborated in Tables 2, 3. After inductive analysis, those codes were assigned to the thematic groups of mindfulness, transcendence, and transpersonal-mindfulness, as indicated in this figurative table. Together, these thematic groups can be sequenced to form the “mindfulness-to-transcendence” (MT) framework, as discussed in the text. The contemplative neuroscientific underpinnings of this thematic MT framework were verified using electroencephalogram-based brain-computer-interface devices, which will be presented in the subsequent papers.Image credits: Ramakrishnan Parameshwaran.
Illustrating the phenomena of clinician’s non-agency in the patient’s healing
Please see Table 3 in Appendices and Figure 1 for the open codes that are referred to in this section. At the end of RP’s (45-minute) visit, the patient broke down into tears (O23b). Vulnerable tearfulness in therapy has been recognized to signify patients’ healing experience [17,18,20-22]. However, this patient did not verbalize any healing experience at that time. The patient’s thankful expressions at the end of that chaplaincy visit were subdued (P13-O26), contrasting his high elation the following morning (P17a, b; P15-19, O30-36, especially O33b). After his spiritual care visit, RP went about performing several routines such as entering his clinical notes, discussing the treatment plan with the nurse (O27a, b, c), and leaving the medical floor toward his night shift sleep room. Only after walking through the long hospital corridor, RP suddenly (S27a) started to feel “I did not provide any substantial care to this patient!” (S27a). It was as if he was in a deep meditative trance until that point on his walk through that long corridor. Such a state of trance or altered consciousness is reportedly experienced by hypnotherapists during their therapy sessions [31] and by meditators in their deep meditative states [32,33].
We argue that this psychiatrist-chaplain/RP had a similar experience of trance or altered state of consciousness from which he slowly emerged at the end of his long walk through the corridor several minutes after his EL session. This is similar to how hypnotherapists, for example, Gilligan, realize that they were in a trance while providing hypnotherapy to their patients only after reviewing the video recording of their hypnotherapy sessions [31].
The state of trance is intrinsic to a patient-therapist relationship, wherein both the therapist and the patient enter into a dissociative shared trance state [34]. Therefore, the patient may also have reflectively and unconsciously transcended into the selfless/beyond-mindful state along with RP and had experienced a similar trance state that may have corresponded with the time and duration of the trance experienced by RP. This trance-like state explains how the patient was subdued at the end of the EL/spiritual care session. In the case of RP, the deep meditative process which induces the trance state may also have freed him from the conceptual thought of being a doer/doing [14] and hence the feeling of “non-agency.”
Studying the phenomena of awe and mechanism of healing in EL/spiritual care
In a shared trance state [34] where the dichotomy of doer vs. doing and self vs. other is dissipated, the psychiatrist and the patient are said to be in a non-dual state of consciousness [14,35-37]. In this non-dual state is the perception of overwhelmingly expanded consciousness that transcended the individual’s (RP and patients’) restrictive cognitive schemas of self vs. other. In that transcendental state of mind, RP and the patient would have experienced the awe.
RP re-visited the patient expecting to find the patient in the same depressed state that he saw the previous evening (O27a, b). However, he was pleasantly surprised (S34a, RP14, see Table 3 in Appendices) upon witnessing the patient in a “happy” state of mind. That joy that followed the patient’s vulnerability and tearfulness (P5b, P11b, O23b) may be argued as his emotionally healed state, especially when we note how his vegetative functions such as appetite and sleep improved (P17b, O41a). RP’s verbal expression of “Wow!!” (RP14) and inner feeling (S34a) reveal his experience of awe, a pleasant surprise or shock from facing the unexpected outcome of the patient’s healing (S36). Furthermore, on closer study of the granular details of the EL interaction, one may note there were several occasions when RP experienced Awe/Wow (S9a, S12a, S19b, S21a, S24a, S28a, S30, S33a, S34a,b, S40a). These moments of Awe transpired as RP was shocked or surprised by unexpected disclosures of the patient (P5b, P10b, P11b, P12b) and a sudden turn of events in the interaction (P6).
To understand how RP could have possibly experienced shock or surprise on so many occasions during the EL interaction we pay attention to RP’s mindful-meditative activity of suspending all his judgmental thoughts and feelings (S7e, S8b, S10b, S11b, S13b, S20b, S23c). Such an act of suspending one’s judgmental thoughts (epochē, Greek) is understood as a religious reader’s meditative method of transcendence [38]. Thus, through the EL interaction, RP had repeatedly been transcending into the non-dual state of mind into which he continually invited the patient through mindful facilitation. As trance is intrinsic to such an empathic physician-patient relationship [34], the patient too would have experienced the transcendence and hence healing.
Thus, the events of awe, non-agency, and the healing outcomes belong to the stage of “beyond mindfulness” or better termed “transcendence.” This stage of transcendence has not been reported previously in the literature discussing the chaplain’s EL process [17,18]. Accommodating this newly described state of transcendence into the mindfulness-based framework of chaplaincy is crucial for an evidence-based understanding of the transcendence aspects of the healing in the psychiatrist’s EL interactions. The mindfulness-to-transcendence (MT) framework of the EL assessment process is illustrated in Figure 1 and Figure 2.
Figurative illustration of the mindfulness-to-transcendence framework of the empathic listening assessment process.Image credit: Ramakrishnan Parameshwaran.
Discussion
Summary
In the six case studies presented in this paper, we have consistently found how an EL interaction is a mindful meditation process, which includes the following thematic stages: (1) the psychiatrist’s mindfulness. This stage begins with the psychiatrists’ empathic and attentive focus on the pain and suffering that the patients share verbally and nonverbally while telling stories about their losses. Then the psychiatrist would become mindful of how their painful memories similar to those of the patient’s loss and the related thoughts and emotions are getting triggered while listening to their patients’ stories. (2) While gaining an emotional and experiential understanding of the patient’s pain and struggles psychiatrists would continually discard all their self-referential and judgmental thoughts and feelings about their patients. In addition, they become indifferent/unattached to their own preconceived ideas, intentions, urges, and plans for treating the patient. In becoming indifferent to their clinical expectations and therapeutic ambitions (a positive and nonpathological approach), the psychiatrists gain the wisdom that the patients themselves have the innate ability to become self-empathic to heal themselves. Such wise psychiatrists would have entered the (3) transcendental or beyond-mindful state wherein, staying transpersonally mindful of their patient’s pain and struggles, they would merely verbalize to name the various emotions and struggles that their patients may be experiencing. (4) Such a “naming” process of wise psychiatrists would herald the patients’ stage of “facilitated mindfulness” in which the patients would become self-empathic to their pain and suffering related to their losses. Through the psychiatrists’ continued facilitation of their mindfulness, the patients enter their (5) stage of “facilitated transpersonal mindfulness,” in which they unconsciously and reflexively discard their mental and emotional preoccupations with their losses, reflecting their psychiatrists’ indifference to the idea of “fixing” their problems through cognitive schemas. Becoming free from their cognitive schemas is their self-transcendence. That transcendence is a conscious space that is beyond mindful awareness, which is shared by both psychiatrists and their patients. These thematic stages of the EL assessment process have been organized to arrive at the MT framework (Figures 1, 2).
In becoming free from all the cognitive schemas relating to their losses in life with which they were emotionally bound and stifled, the patients feel free from suffering. In that, they attain their empowered state of self-empathy and self-healing, though they would be in awe at their physician and credit the physician for their healing outcomes. Psychiatric textbooks do talk about how a psychiatrist’s diagnostic assessment, when conducted through EL, can be therapeutic and increase the patient’s sense of agency [39,40]. Psychiatrists, on the other hand, who had relinquished their therapeutic ambitions and intentions through the MT framework of the EL process, would naturally feel they have “not provided anything substantial to heal their patients.”
The study of the granular details of the subjective, mindfulness process is essential to understand how transcendence and its emotions of awe and non-agency emerge: the psychiatrist’s repetitive act of suspending all his cognitive processes (epochē) was essential for their self-transcendence. In that transcendent state, the psychiatrist had become child-like to be non-expectant of anything and therefore to be surprised by the patients’ disclosures and sudden changes in their speech and behavior and to be awed by them. On the part of the patients, with their growing trust in the psychiatrist, they would share more and more painful stories, as if peeling the onion, to reach the most painful story that may be troubling them in the current moment. Such self-revelation on the part of the patients is a sign of their growing rapport, which is, in turn, a sign of the loss of their self-preserving ego boundaries, which is their transcendence (Figures 1, 2). Elsewhere in this paper, we argued that this psychiatrist-chaplain/RP’s experience of trance or altered state of consciousness stretching beyond the EL care session was similar to the experience of hypnotherapists [31]. Thus, while not necessarily a focus of this paper, we have illustrated that the hypnotic state is achievable in an EL assessment without the psychiatrist establishing themself as a hypnotherapist.
Thus, in an EL interaction, “awe” is the emotion of the perception of vast consciousness (self-transcendent space) that transpires when the physicians and their patients become unbound by the cognitive schemas that differentiate them from one another. The deeply empathic presence, which in itself is a caregiving act, is indeed the act of a transcendental mind, which is an altered state of consciousness. In that state, psychiatrists become (positively or non-pathologically) apathetic to their therapeutic intentions and ambitions toward their patients. In turn, they are freed from the conceptual thought of having provided any substantial care to the patients, hence the feeling of non-agency in the patients’ healing outcome. Together, the emotions of awe and non-agency signify the physicians’ transcendence beyond their mindful awareness in which they function during the EL interactions.
This paper and its findings’ standing in the current scheme of things and future directions
Some of the mindfulness-based steps described in this EL process correspond to the Freudian principles of “ungrounded attention, unintentionality, and indifference (termed in this paper as ‘positive or nonpathological-apathy’) to therapeutic ambition” in psychoanalytic psychotherapy [41]. However, with our elaboration on how these Freudian principles could be closely related to the mindful and transcendental states of mind, which is the experience of awe, one may understand how Freudian psychoanalysis could have taken a turn toward a spiritual or transcendent position in Bionian supra-personal/spiritual psychoanalysis [42].
Recognizing awe and non-agency as emotions of transcendence is essential in conceptualizing the empirical MT framework of EL assessments, and the first step toward the evidence-based studies of it. To note, through this inductive analysis, we have closely studied neuroscientific literature on the emotions of awe and transcendence [10,11,35-37,43,44] to string the contemplative events of mindfulness, transcendence, and transpersonal mindfulness in the correct sequence to develop the MT framework of the EL assessment [17-19]. Going back and forth between the neuroscientific literature and the qualitative data confirmed that there could be a contemplative neuroscientific framework underpinning the empirical MT framework of the EL assessment process. We have also conducted follow-up studies to verify this MT framework using portable electroencephalogram (EEG)-based, brain-computer-interface devices, the findings of which will be presented as a sequel to this article.
While a transcendental state has been reported in meditation [45], we may be the first to illustrate how it is achievable by both the psychiatrist and their patient in a clinical setting through their EL (mindfulness-based meditative) interaction. It is through such a self-transcendent state that psychiatrists could grow deeply empathic to gain a first-person experience of their patients’ intrapsychic conflicts for improved accuracy in their diagnostic assessment; psychiatric textbooks do inform us of improved accuracy in EL assessments but they have not illustrated how [38,39]. Using the same case series studies, in the subsequent publication, we will illustrate how EL assessments in psychiatry could improve the diagnostic accuracy of psychiatrists.
Indeed, the self-transcending meditative state that is reported [43,44] as a self-healing state by other researchers is confirmed in this study. In that sense, even the psychiatrist would inevitably come out feeling healed as much as the patients do. This study illustrates and confirms how EL assessments could provide healing outcomes for psychiatrists and protect them from caregiver burnout, as mentioned in psychiatric textbooks [40]. This article illustrates how it is possible to study the emotions of awe and non-agency which signify the cognitive-schema free or the “unknowable” state of mind. In that, we agree with other researchers on the possibility of studying the unknowable [46,47]. Clinical chaplains who study their spiritual care (actually another term for EL) process refer to their scriptural texts and reverently ascribe the healing outcomes as the act of the Divine, the Unknowable Transcendent [9,15,16]. Discussions on how to understand the Transcendent using theistic language and constructs are out of the scope of this study but may be an inevitable next step if we have to integrate the disciplines of spirituality and psychiatry in an evidence-based way, for which there has been a growing demand [18,48,49].
Strengths and limitations
This is the first empirical study on the phenomena of awe and non-agency in EL assessment in psychiatry. In arriving at the MT framework, we have advanced the empirical framework of the EL assessment process which is grounded in contemplative neuroscience and hence amenable to application in evidence-based studies of it.
This researcher’s experiences of witnessing awe-inspiring healing outcomes may be argued as anecdotal. One may also argue that the healing expressions could be Kleinian manic-defense or “flight into health” [50,51] and hence a pseudo-healing. However, from our experiences in this case series, the limitations of the small sample size notwithstanding, we challenge those arguments because of the consistent findings across all six case studies. We also feel supported by similar publications on clinicians’ experiences of witnessing awe-inspiring healing outcomes in EL care [3,4,52]. We argue that replicability and reproducibility of the findings of this study can be possible by other psychiatrists after CPE training in EL assessment [6] or with training in the method of Bionian supra-personal psychoanalysis [41].
The kind of phenomena (awe, and non-agency) under consideration are those that cannot be observed or experienced by a second or third person. An attempt to reach objectivity was made by providing the supervisor’s hand-written note (see Appendices) which could serve as the third-person correlation grounded on the behavioral domain. An alternative to contemporaneous recording of the interaction after exiting the patient’s room could be an audio/video recording of the interaction itself. However, the subjective thoughts and feelings that the psychiatrist/EL provider experienced during the EL process can only be retrospectively re-read/re-heard from his memory. The accuracy of that recollection depends on the meditative state that the provider maintains during the contemporaneous note-writing process, which can be verified by continuing with the EEG-neurofeedback recording through the note-writing process. Though audio (better) video recording improves the objectivity of this kind of study, the classification of the EL process into focused attention, open mindfulness, and transcendental states (the MT framework) is possible only based on the subjective experiences of the EL care provider. How these subjective, contemplative states can be objectively verified using EEG frequency markers will be presented in our subsequent paper.
Conclusions
This paper delves into psychiatrists’ experiences of awe and non-agency during their EL assessments to highlight them as signifiers of the transcendental state of mind. Through a qualitative and analytical approach, this research uncovers the nuances of the EL process, shedding light on the emotions of awe and non-agency that have previously been overlooked in clinical studies. By embracing a mindfulness-based research methodology, researchers can bridge the gap between scientific skepticism and the philosophical understanding of transcendental states, ultimately demystifying the healing mechanism behind EL assessments. With a deeper appreciation for the role of awe and non-agency in the healing process, psychiatrists can cultivate a pedagogy of EL assessments while still striving to understand the complexities of transcendental states. Despite the conceptual challenges that remain, this study of transcendence is essential for paving the way for future exploration of evidence-based studies on EL assessment in psychiatry and its therapeutic outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Compassionate Connection: The Healing Power of Empathy and Mindful Listening Rakel D New York, NYWW Norton & Company 2018 https://books.google.com/books?hl=en&lr=&id=ij Is Dw AAQBAJ&oi=fnd&pg=PT 4&dq=Rakel,+D:+The+compassionate+connection:+The+healing+power+of+empathy+and+mindful+listening.+2018.&ots=Le G Gn R 6z IZ&sig=Mje U 7ano 7Jfv 8q Q Ahhotc MP Mhcw#v=onepage&q=Rakel%2C%20D%3A%20The%20compassionate%20connection%3A%20The%20healing%20power%20of%20empathy%20and%20mindful%20listening.%202018.&f=false
- 2Awe and the transforming of awarenesses Contemp Psychoanal Andresen JJ 507521351999
- 3Secrets and magic Br J Gen Pract Senior T 1006420142456761010.3399/bjgp 14X 677284 PMC 3905421 · doi ↗ · pubmed ↗
- 4The wise physician Fam Med Gerard RJ 586588311999 https://pubmed.ncbi.nlm.nih.gov/10489642/10489642 · pubmed ↗
- 5But at the Same Time and on Another Level. Clinical Applications in the Kleinian/Bionian Mode Grotstein JS London, UK Routledge 2018 https://www.routledge.com/But-at-the-Same-Time-and-on-Another-Level-Clinical-Applications-in-the/S-Grotstein/p/book/9781855757608
- 6Association for Clinical Pastoral Education. Programs 2 2024 2024 https://acpe.edu/programs
- 7Defining and operationalizing chaplain presence: a review J Relig Health Adams K 124612585820193056516710.1007/s 10943-018-00746-x · doi ↗ · pubmed ↗
- 8Companioning the Bereaved: A Soulful Guide for Counselors & Caregivers Wolfelt AD Chicago, IL Companion Press 2005 https://www.goodreads.com/en/book/show/3100976