Letter to the editor on: prophylactic nicotinamide treatment protects from rotenone-induced neurodegeneration by increasing mitochondrial content and volume
Cinzia Bocca, Judith Kouassi-Nzoughet, Juan Manuel Chao de la Barca, Dominique Bonneau, Christophe Verny, Philippe Gohier, Christophe Orssaud, Pascal Reynier

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
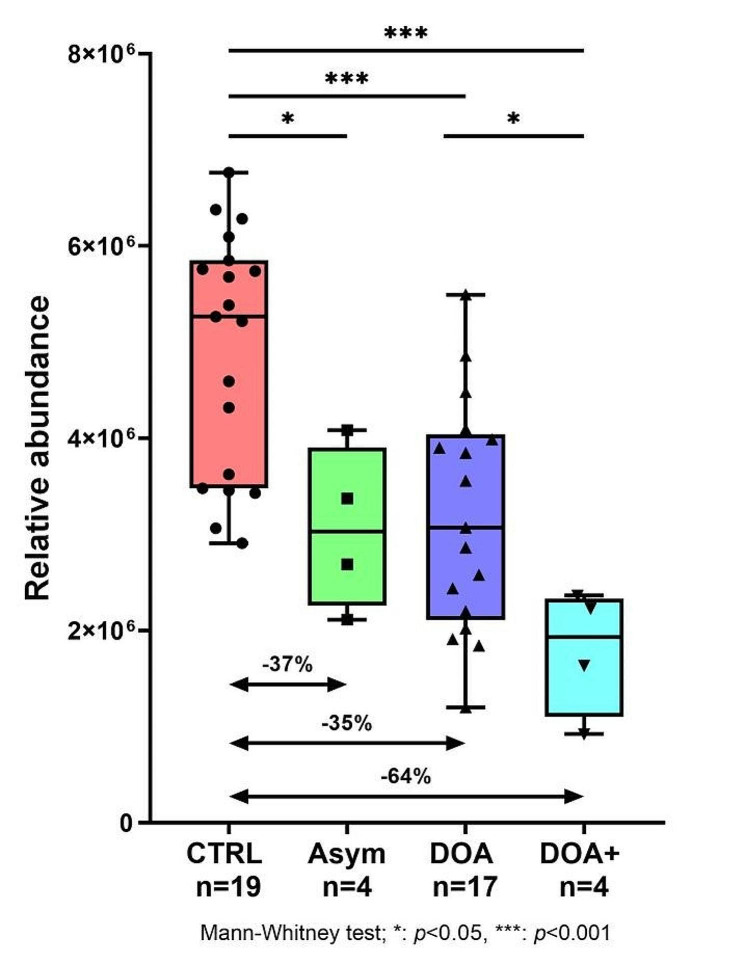 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMitochondrial Function and Pathology · Neurological Disease Mechanisms and Treatments · Sirtuins and Resveratrol in Medicine
Dear editor,
We have read with great interest the article published by Otmani et al. in Acta Neuropathologica Communications reporting that nicotinamide (vitamin B3) protects retinal ganglion cells against rotenone-induced neurodegeneration [1]. In a previous pre-clinical study, published in 2017 in Science, the same team had shown that oral intake of nicotinamide could prevent retinal ganglion cell loss in a murine model of glaucoma [2]. Subsequently, encouraging results of two clinical trials of nicotinamide in individuals affected with glaucoma were reported [3, 4]. In the current study, Otmani et al. provide a pre-clinical rationale for the use of nicotinamide in Leber’s Hereditary Optic Neuropathy (LHON), one of the two most common hereditary optic neuropathies.
We would like to provide additional arguments in favor of the use of nicotinamide in optic neuropathies. Using a hypothesis-free metabolomics approach, performed in 2021 on 18 individuals affected with LHON and to 18 healthy controls, we evidenced that individuals with LHON had a nicotinamide deficiency in blood compared to controls [5]. The metabolomic signature in plasma of individuals with LHON comprised 13 discriminating metabolites including dietary metabolites (nicotinamide, taurine, choline, 1-methylhistidine and hippurate), mitochondrial energetic substrates (acetoacetate, glutamate and fumarate) as well as inosine, an essential metabolite for purine biosynthesis.
In addition, we carried out a similar metabolomics investigation in individuals affected with Dominant Optic Atrophy (DOA) caused by OPA1 pathogenic variants, the other most common form of hereditary optic neuropathy. In this study, we compared the plasma of 25 affected individuals with that of 20 healthy controls [6]. Within the metabolomic signature of DOA, we found, a C_6_H_6_N_2_O chemical compound, not identified at the time of the publication, whose concentration was significantly lowered. Subsequently, this compound was identified as nicotinamide. A deeper analysis taking into account the severity of the DOA phenotype showed that, compared with healthy controls, nicotinamide was lowered by 37% in asymptomatic carriers (p < 0.05), by 35% in DOA patients (p < 0.001) and by 64% in patients with most severe syndromic form of the disease referred to as DOA+ (p < 0.001) (Fig. 1, unpublished data). Altogether, these results give arguments in favor of the therapeutic interest of nicotinamide in both isolated and syndromic forms of DOA.
We therefore have launched a clinical trial (https://classic.clinicaltrials.gov/ct2/show/NCT06007391) to test the safety and efficacy of three grams per day of oral nicotinamide for six months in 25 individuals with DOA who will have ophthalmic, neurological and biological (blood nicotinamide concentration) monitoring.
Finally, primary open-angle glaucoma, was the third disease for which our hypothesis-free metabolomics approach revealed a nicotinamide deficiency in affected individuals compared to healthy controls. This deficiency was confirmed by an independent targeted mass spectrometry measurement on two cohorts of individuals (34 and 30 patients compared to 20 and 15 healthy controls respectively) [7].
There is therefore a deregulation of nicotinamide metabolism in glaucoma, the most common form of optic neuropathy worldwide, as well in LHON and DOA, the two most common hereditary optic neuropathies.
We can wonder whether such deficiency in nicotinamide could be present in other rare and common forms of optic neuropathies, and whether nicotinamide might not universally protect retinal ganglion cells. The origin of this relative deficiency in nicotinamide is undoubtedly not of dietary origin but probably rather the result of a dysfunction of mitochondrial energy metabolism leading to an excessive consumption of nicotinamide used by cells for the endogenous synthesis of Nicotinamide Adenine Dinucleotide (NAD) which plays a major role in this energetic metabolism. Future clinical trials are needed to further characterize the potential of blood nicotinamide concentration as a biomarker for optic neuropathies or, more generally, for pathologies involving mitochondrial dysfunction. Indeed, plasma nicotinamide assay is rarely used in clinical practice, and the most widespread assay using High Performance Liquid Chromatography coupled to ultraviolet detection (HPLC-UV) performed on whole blood, is not very sensitive. The recent use of mass spectrometry in plasma samples should make it possible to detect more subtle variations in nicotinamide concentration that may be of clinical interest. It will also be of great interest to know the results of future clinical trials using nicotinamide in these different forms of optic neuropathies.
Fig. 1. Comparison of nicotinamide level detected after a metabolomic approach [6] in the plasma of healthy controls (CTRL), asymptomatic OPA1 pathogenic variants carriers (Asym), and patient with isolated (DOA) or syndromic (DOA+) forms. * p < 0.05; *** p < 0.001
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Otmani AJóhannesson G Brautaset R Tribble JR Williams PA Prophylactic nicotinamide treatment protects from rotenone-induced neurodegeneration by increasing mitochondrial content and volume Acta Neuropathol Commun 20241213710.1186/s 40478-024-01724-z 38429841 PMC 10908050 · doi ↗ · pubmed ↗
- 2Williams PA Harder JM Foxworth NE Cochran KE Philip VM Porciatti V Vitamin B 3 modulates mitochondrial vulnerability and prevents glaucoma in aged mice Science 2017355632675676010.1126/science.aal 009228209901 PMC 5408298 · doi ↗ · pubmed ↗
- 3Hui F Tang J Williams PA Mc Guinness MB Hadoux X Casson RJ Improvement in inner retinal function in glaucoma with nicotinamide (vitamin B 3) supplementation: a crossover randomized clinical trial Clin Exp Ophthalmol 202048790391410.1111/ceo.1381832721104 · doi ↗ · pubmed ↗
- 4De Moraes CG John SWM Williams PA Blumberg DM Cioffi GA Liebmann JM Nicotinamide and pyruvate for Neuroenhancement in Open-Angle Glaucoma: a phase 2 Randomized Clinical Trial JAMA Ophthalmol 20221401111810.1001/jamaophthalmol.2021.457634792559 PMC 8603231 · doi ↗ · pubmed ↗
- 5Bocca C Le Paih V Chao de la Barca JM Kouassy Nzoughet J Amati-Bonneau P Blanchet OA plasma metabolomic signature of Leber hereditary optic neuropathy showing taurine and nicotinamide deficiencies Hum Mol Genet 2021301212910.1093/hmg/ddab 01333437983 PMC 8033144 · doi ↗ · pubmed ↗
- 6Bocca C Kouassi Nzoughet J Leruez S Amati-Bonneau P FerréM Kane MSA plasma metabolomic signature Involving Purine Metabolism in Human Optic Atrophy 1 (OPA 1)-Related disorders Invest Ophthalmol Vis Sci 201859118519510.1167/iovs.17-2302729340645 · doi ↗ · pubmed ↗
- 7Kouassi Nzoughet Jde la Chao JM Guehlouz K Leruez S Coulbault L Allouche S Nicotinamide Deficiency in Primary Open-Angle Glaucoma Invest Ophthalmol Vis Sci 20196072509251410.1167/iovs.19-2709931185090 · doi ↗ · pubmed ↗