A rare case of isolated persistent left superior vena cava diagnosed by echocardiography
Dorota Smolarek, Hanna Jankowska, Karolina Dorniak, Marcin Hellmann

TL;DR
A rare case of a persistent left superior vena cava was diagnosed using echocardiography in a 35-year-old man.
Contribution
This case highlights the diagnostic value of echocardiography in identifying isolated persistent left superior vena cava.
Findings
Echocardiography revealed an enlarged coronary sinus and confirmed isolated PLSVC.
Agitated saline injection confirmed drainage via the left superior vena cava into the coronary sinus.
The case underscores the clinical importance of recognizing this rare vascular anomaly.
Abstract
The persistent left superior vena cava (PLSVC) is an infrequent vascular variant. PLSVC with absent right superior vena cava, also known as isolated PLSVC, is an exceptionally rare entity. In this case we present a patient with isolated PLSVC draining to coronary sinus, diagnosed incidentally during echocardiography. A 35-year-old man underwent a transthoracic echocardiography which showed an enormously dilated coronary sinus. Hand-agitated saline was injected via peripheral intravenous cannulas. The contrast appeared firstly in the coronary sinus before it opacified the right atrium. Since this was also visible by the right antecubital saline injection, it indicated an extremely rare case of PLSVC with the absence of right superior vena cava which was confirmed by cardiac magnetic resonance. The finding of a distinctively dilated coronary sinus in echocardiography led us to further…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
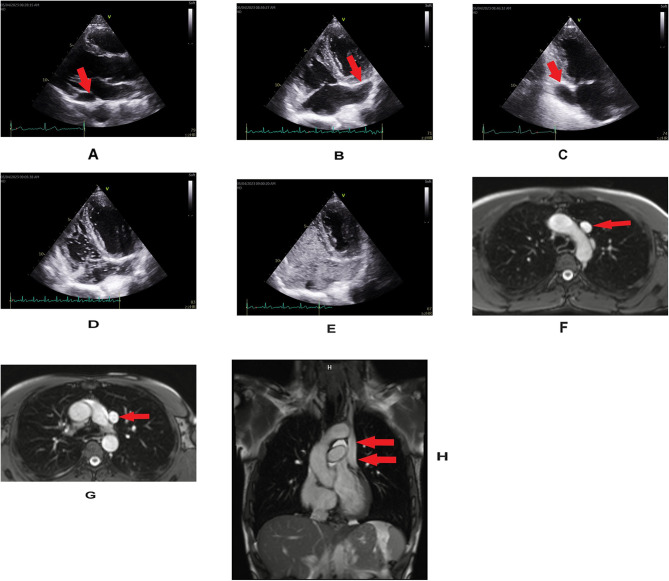 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Coronary Artery Anomalies · Cardiac Arrhythmias and Treatments
Background
The persistent left superior vena cava (PLSVC) is a remnant of the embryonic left anterior cardinal vein [1]. Most cases of PLSVCs coexist with the presence of right-sided vein and this condition is recognised as superior vena cava (SVC) duplication. PLSVC with the agenesis of right SVC, also known as isolated PLSVC, is an exceptionally rare entity [2]. Almost half of patients with this vascular variant have additional cardiac anomalies such as atrial septal defect, endocardial cushion defects, or tetralogy of Fallot [3].
Case presentation
A 35-year-old man with systemic sclerosis (SSc) was referred to our cardiology outpatient clinic for a routine transthoracic echocardiography. The diagnosis of SSc was made four years earlier on the basis of a clinical picture and presence of autoantibodies (anti-Scl-70). The main symptoms regarded a skin thickening of the fingers of both hands, fingertip lesions, darker skin pigmentation and microcheilia. Moreover, the features of interstitial lung disease were identified in computed tomography and ultrasonography. No cardiovascular complaints were present. Transthoracic echocardiography showed a normal size of ventricles with preserved systolic function, low probability of pulmonary hypertension and enormously dilated coronary sinus (CS) visible in all echocardiographic views (Fig. 1A, B, C). There were no signs of other cardiac lesions such as valvular heart disease or atrial septal defect. Pulsed-wave doppler did not reveal any abnormal shunting between the left atrium and the CS. As there was a suspicion of PLSVC hand-agitated saline was injected via peripheral intravenous cannulas. The contrast appeared firstly in the huge CS before it opacified the right atrium (Fig. 1D, E; Suppl. Video). Since this was also visible by the right antecubital saline injection, it indicated a rare case of PLSVC with the absence of right SVC. The diagnosis was confirmed by cardiac magnetic resonance imaging which visualized the isolated PLSVC using standard steady-state free precession acquisitions, covering the entire chest in orthogonal (i.e. in both transverse and coronal) 8 mm thick cross-sections with 2 mm spacing to delineate anatomy. These acquisitions pertained to a standard cardiac protocol, namely to avoid missing rare but potentially important extracardiac findings (Fig. 1F, G, H).
Fig. 1A, B, C, D, E. Transthoracic echocardiography. A, B, C. Significantly dilated coronary sinus (arrows)- dimensions; parasternal long axis view- 2.3 × 1.4 cm (A), four-chamber view- 2.2 cm (B), two-chamber view- 2.9 × 1.7 cm (C). D, E. The injection of agitated saline into the right arm vein resulting in the opacification of a dilated coronary sinus followed by right atrial filling. F, G, H. CMR. Single-shot SSFP images, showing a single persistent left SVC (arrows), with the right-sided SVC missing in its typical position to the right and posteriorly from ascending aorta. F, G. The image from an axial stack. H. The coronal image CMR-cardiac magnetic resonance, SSFP-steady state free precession sequence, SVC-superior vena cava
Discussion and conclusions
Vascular anomalies represent a broad spectrum of different pathologies involving arteries, veins and lymph vessels [2–5]. Although taking into account all of them, PLSVC is infrequent, it is the most common congenital malformation of thoracic venous return that affects 0.2 to 3% of the healthy population [6]. On the other hand, PLSVC with absent right SVC is an extremely rare venous anomaly [2]. PLSVC forms when the left anterior cardinal vein fails to obliterate during fetal life [1]. It usually originates from the junction of the left subclavian and internal jugular veins, proceeds through the left side of the mediastinum adjacent to the aortic arch. It mostly connects to the right atrium via the CS widening its structure. Less frequently PLSVC drains into the left atrium directly or through an unroofed CS which leads to right-to-left shunt. In current case, the humongous CS (up to 29 mm in apical two- chamber view, with normal values set at 8.27 ± 2.5 mm [7]) might suggest that it was a vascular variant of only one SVC present. The isolated PLSVC carries the entire upper body venous return leading to a huge size of the CS, larger than in the co-existence of the right-sided SVC simultaneously draining directly into the right atrium. Moreover, the fact that both left and right antecubital contrast injection reached the same result, that is, opacification of the enormous CS prior to right atrial filling, indicated the diagnosis of isolated PLSVC. In most cases it causes no hemodynamic consequences and is usually discovered incidentally on either imaging or during intervention. Nevertheless, the proper in-depth diagnosis is vital. PLVSC is a potential factor triggering common arrhythmia- atrial fibrillation, and the presence of isolated PLVSC increases the risk of complications during left atrial ablations [8]. More frequent monitoring for atrial fibrillation and special preparation in case of indications for ablation may be relevant. PLSVC may also have other important clinical implications, such as difficulties with central venous access, cardiothoracic surgeries, and pacemaker or defibrillator implantations, especially in the current era of a rapid development of cardiovascular device therapies with reference to increasing life expectancy and ageing of population.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Video: Bubble contrast echocardiography. Hand-agitated saline was injected via peripheral intravenous cannulas. The contrast appeared firstly in the huge coronary sinus before it opacified the right heart. As the same situation appeared by left and right antecubital saline injection, it indicated a rare case of isolated PLSVC. PLSVC- persistent left superior vena cava
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nsah EN, Moore GW, Hutchins GM. Pathogenesis of persistent left superior vena cava with a coronary sinus connection. Pediatr Pathol. 1991 Mar-Apr;11(2):261–9.10.3109/155138191090647632052508 · doi ↗ · pubmed ↗
- 2Goyal SK Punnam SR Verma G Ruberg FL Persistent left superior vena cava: a case report and review of literature Cardiovasc Ultrasound 200865010.1186/1476-7120-6-5018847480 PMC 2576163 · doi ↗ · pubmed ↗
- 3Sarodia BD Stoller JK Persistent left superior vena cava: case report and literature review Respir Care 2000454411610780037 · pubmed ↗
- 4Tarniceriu CC Hurjui LL Tanase DM The pulmonary venous return from normal to pathological-clinical correlations and review of literature Med (Kaunas)202157329310.3390/medicina 57030293 PMC 800419133809829 · doi ↗ · pubmed ↗
- 5Evans WN Acherman RJ Ciccolo ML Isolated Vascular rings are Common Cardiovascular malformations World J Pediatr Congenit Heart Surg 202314121310.1177/2150135122112297236847763 · doi ↗ · pubmed ↗
- 6Azizova A Onder O Arslan S Persistent left superior vena cava: clinical importance and differential diagnoses Insights Imaging 202011111010.1186/s 13244-020-00906-233057803 PMC 7561662 · doi ↗ · pubmed ↗
- 7D’Cruz IA Shala MB Johns C Echocardiography of the coronary sinus in adults Clin Cardiol 20002331495410.1002/clc.496023030410761800 PMC 6654866 · doi ↗ · pubmed ↗
- 8Peregud-Pogorzelska M Zielska M Zakrzewski M Cryoablation of pulmonary veins for the treatment of paroxysmal atrial fibrillation coexisting with isolated persistent left superior vena cava Kardiol Pol 20187611157210.5603/KP.2018.022130460671 · doi ↗ · pubmed ↗