Relationship between the natural cessation time of umbilical cord pulsation in full-term newborns delivered vaginally and maternal-neonatal outcomes: a prospective cohort study
Ruijie Wu, Yuan Zhang, Jiaqi Chen, Tongchao Zhang, Xiaorong Yang, Xiangyu Xu, Mi Li, Dong Li, Xiaoyan Liu, Ming Lu

TL;DR
This study finds that waiting 61–89 seconds for the umbilical cord to stop pulsating naturally after birth may improve maternal and newborn outcomes compared to waiting longer.
Contribution
The study identifies an optimal natural umbilical cord clamping time (61–89 seconds) that may improve maternal and neonatal outcomes.
Findings
No significant differences in maternal postpartum hemorrhage or supplement needs across cord clamping time groups.
Newborns in the 61–89 second group had higher hemoglobin and lower hyperbilirubinemia compared to longer clamping times.
Cord detachment occurred faster in groups with longer natural clamping times.
Abstract
To analyze the impact of the time of natural cessation of the umbilical cord on maternal and infant outcomes in order to explore the time of clamping that would be beneficial to maternal and infant outcomes. The study was a cohort study and pregnant women who met the inclusion and exclusion criteria at the Obstetrics and Gynecology Department of Qilu Hospital of Shandong University from September 2020 to September 2021. Analysis using Kruskal-Wallis rank sum test, Pearson’s Chi-squared test, generalized linear mixed model (GLMM) and repeated measures ANOVA. If the difference between groups was statistically significant, the Bonferroni test was then performed. A two-sided test of P < 0.05 was considered statistically significant. A total of 345 pregnants were included in this study. The subjects were divided into the ≤60 seconds group (n = 134), the 61–89 seconds group (n = 106) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
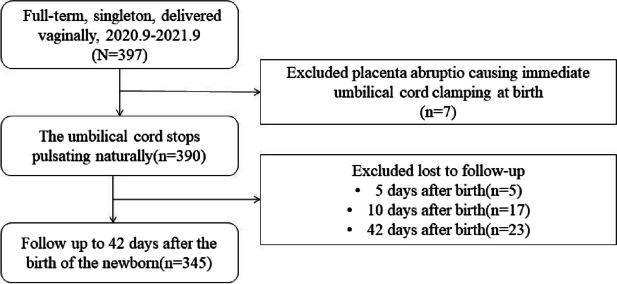 Figure 1
Figure 1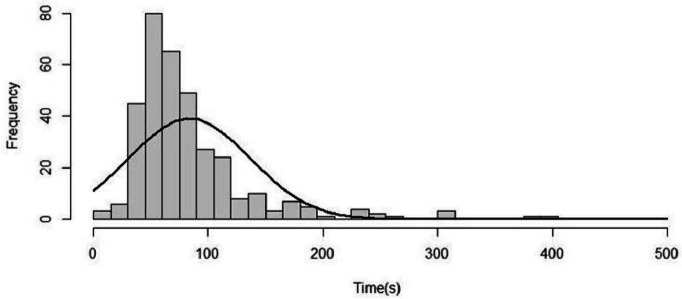 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Congenital Diaphragmatic Hernia Studies · Pregnancy and preeclampsia studies
Introduction
After delivery, the newborn still shares blood circulation with the placenta and umbilical cord. The transfer of blood from the placenta to the newborn is a quite rapid stepwise progression and is almost finished in 3 minutes [1]. When the infant is delivered, about 30% of the blood is present in the placenta [2]. The blood flows into the newborn with the contraction of the umbilical artery and the uterus. The relationship between umbilical cord blood flow and umbilical cord pulsation is more complex. When the umbilical cord pulsation stops, the umbilical cord blood flow may not stop yet, and the blood flow may be still from mother to foetus [3]. If immediate or early cord clamping (ECC) is replied to, it may reduce the incidence of hyperbilirubinemia and polycythemia in newborns, and also reduce the requirement for phototherapy [4]. However, it may also increase the need for neonatal oxygen therapy and the risk of maternal postpartum hemorrhage [5]. Delayed cord clamping (DCC) usually defined as clamping the umbilical cord more than 60 second after delivery or when cord pulsation stops [6]. DCC may cause some benefits. It can reduce the incidence of anemia, iron deficiency, iron deficiency anemia, intraventricular hemorrhage (IVH), chronic lung disease and necrotizing enterocolitis. It could equally have a positive impact on the neurological and cognitive development of children aged 8 months and 12 months [7, 8]. It also improves the survival rate of preterm infants and reduces the risk of maternal anemia due to blood loss during the third stage of labor [9]. Potential disadvantages of DCC are the need for jaundice treatment and maternal blood transfusion [6, 8]. Therefore, there are advantages and disadvantages to early or delayed cord clamping for mothers and infants (both preterm and term), and there is still considerable international debate about the best time to clamp the umbilical cord.
The American College of Obstetricians and Gynecologists (ACOG) recommends delayed umbilical cord clamping in full-term neonates and preterm infants for at least 30–60 seconds after birth [10]. The World Health Organization (WHO) recommends that the umbilical cord should be clamped between 1 and 3 minutes after birth as part of the active management of the third stage of labor (AMTSL), in order to improve maternal and neonatal outcomes unless the baby has special circumstances such as neonatal asphyxia and the need for resuscitation [11]. National Institute for Health and Care Excellence (NICE) recommends if there is no concern about the integrity of the umbilical cord or if the baby’s heart rate is below 60 beats per minute and is not getting faster, it is best to clamp the cord 1–5 minutes after delivery [12].
Whether to clamp the umbilical cord early or delayed has always been a controversial topic [13]. Although a large number of studies have shown the positive impact of delayed cord clamping on mother and baby, most have not focused on the impact of the time to natural cessation of cord pulsation on maternal and infant outcomes. And there is still a shortfall in guiding the recommended optimal time to clamp the cord. In our study, artificial clipping was performed when the umbilical cord pulsation naturally stopped, disregarding the complex relationship between subsequent umbilical blood flow and umbilical cord pulsation. We aimed to compare the relationship of different times of umbilical cord disconnection with the outcomes of mothers and infants.
Methods
Study design and participants
We recruited study participants (women who delivered full-term newborns) for a prospective cohort study at the Department of Gynecology and Obstetrics, Qilu Hospital, Shandong University between September 2020 and September 2021. Full-term infants were defined as gestational age between 37 and 42 weeks. Inclusion criteria: (1) pregnant women age from 18 to 35 years; (2) 37 weeks gestation; (3) vaginal delivery, including lateral episiotomy; (4) participants who voluntarily participate in the study will obtain written informed consent before participation in the study. Exclusion criteria: (1) pregnant women diagnosed with COVID-19; (2)pregnant women with internal and surgical comorbidities; (3) maternal anemia; (4) multiple pregnancies; (5) ABO hemolysis, RH hemolysis; (6) full-term newborns are found to have anomalies and the anomalies affect bilirubin metabolism, such as congenital anal atresia and congenital biliary atresia; (7) pneumonia, hemolytic disease of term newborns and other diseases affecting bilirubin metabolism during the follow-up of term newborns; (8) term small for gestational age (term-SGA); (9) abnormalities on examination after delivery of the placenta, such as placenta praevia, placenta abruptio, placenta rotunda and anterior vascular hemorrhage; (10) stillbirth; (11) postnatal full-term newborn Apgar score ≤ 7 at 1 minute.
The natural cessation time of umbilical cord pulsation and grouping
The interval between the delivery of the baby and the cessation of the pulse of the chord is referred to as the time of cessation of the pulsation of the cord. After birth, the baby was placed between the mother’s knees, wrapped in a sterile towel to keep warm, and the midwife uses her palm to detect the pulse of the umbilical cord close to the baby’s end, while the mobile midwife uses a movement stopwatch to time the movement to the second. When the umbilical artery stops pulsing, the umbilical cord is cut and ligated immediately.
Based on recommendations from the World Health Organization and other agencies, and combined with data collected in the study, participants were divided into three groups according to the duration of umbilical cord arrest: ≤60 seconds, 61–89 seconds, and ≥ 90 seconds.
Study variables
Participants in the study were surveyed using convenience sampling, a non-probability sample method. The variables we collected can be summarized in four parts, the first being demographic information collected after admission to the maternity ward, such as mother’s name, age, occupation, education, ethnicity, BMI (pre-pregnancy and pre-natal), blood type, smoking and alcohol consumption. The second part is clinical information, such as maternal blood count (hemoglobin, red blood cell pressure, etc.) within 1 day before delivery, the cord blood and the total nucleated cells (TNCs) after the umbilical cord is severed. The third section is maternal outcomes, such as maternal postpartum hemorrhage (recorded separately 2 and 24 hours after delivery), blood transfusions (24 hours after delivery), and medication (iron, other drugs or health supplements) for 42 days after delivery. The fourth section is neonatal outcomes, such as blood gas analysis of the umbilical cord artery and vein after delivery (this indicator is taken by the midwife on the delivery team immediately after delivery and blood gas analysis is performed), birth weight and sex of the newborn obtained 2 hours after delivery, blood bilirubin (24 hours, 48 hours, 72 hours, 5 days, 10 days, 42 days after delivery of the newborn). Newborn blood bilirubin was measured using a JH20-1C transcutaneous yellow pox meter and averaged at four points on the forehead, brow, corner of the eye and forehead.
Statistical analysis
The main observation index is the time of cessation of umbilical cord pulsation, according to previous studies [13], the time of umbilical cord pulsation is (120.1 ± 85.9) seconds, the expected error is not more than 10, take α = 0.05 to substitute into the formula:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\textrm{n}={\left[\frac{u_{1-\alpha /2}\sigma }{\delta}\right]}^2,$$\end{document}and calculate n = 284, considering the lost to follow-up and other factors, set a 5% loss to follow-up rate, the number is at least 300 pregnant women.
Descriptive statistics were used for the clinical characteristics of the population. Data for normal continuous variables are presented as mean and standard deviation (SD), and skewed continuous variables are presented as median and interquartile range (IQR); categorical variables are described by frequency and percentage. For maternal and infant outcomes in the different cord clamping groups, the Kruskal-Wallis rank sum test was used for continuous variables to assess the statistical significance of differences; the Pearson’s Chi-squared test was used for categorical information; those with overall differences were then compared between two groups. For the six time points of 24 hours, 48 hours, 72 hours, 5 days, 10 days and 42 days after delivery, we used a generalized linear mixed model (GLMM) to compare the differences between the neonatal outcomes of the different subgroups, using repeated measures of categorical information such as whether the neonate had hyperbilirubinaemia, was taking health supplements or medication. Similarly, for neonatal blood bilirubin at the six time points above, we used repeated measures ANOVA to compare differences between groups and between time points, and then carried out Tukey post-hoc tests if the differences were statistically significant. A value of P < 0.05 for a two-sided test is considered statistically significant. All analyses were performed in R program (Version 4.2.2, R core team, 2022) and IBM SPSS Statistics 25.
Results
Overview
Between September 2020 to September 2021, 397 pregnant women met the inclusion and exclusion criteria. Of these, 7 were excluded for immediate umbilical cord clamping due to placental abruption after delivery., and 45 were lost to follow-up. Finally, 345 participants who met the criteria and had complete data were analyzed (Fig. 1).Fig. 1. Participant flowchart
The natural cessation time of umbilical cord pulsation
In this study, a total of 345 participants were included. They were divided into three groups based on the cord-clamping time, with 134, 106 and 105 participants in each group from shortest to longest time respectively. The age of maternal is 31.0 ± 4.0 years. The range of time of umbilical cord pulsation cessation is 10.00 ~ 403.00 seconds. The median time is 68.00 seconds (IQR: 54.00–95.00).A Shapiro-Wilk normality test for the natural cessation time of umbilical cord pulsation revealed a positively skewed distribution of the data (P < 0.05, Kurtosis = 12.01, Skewness = 2.56) (Fig. 2).Fig. 2. Distribution of time to natural cessation of umbilical cord pulsation in the study population
Baseline characteristics for maternal
Basic characteristics of maternal are presented in Table 1. In terms of occupation and chronic illness, there were statistically significant differences between the three groups. In the three groups, 16.4, 13.2 and 4.8% of the mothers had chronic diseases, respectively, according to the shortest to longest duration of spontaneous cessation of the cord’s pulsation. Whereas, there were no differences between the groups concerning age, age at menarche, BMI, education, gestational age, lifestyle habits (exposure to smoking and alcohol), drugs or health supplements during pregnancy (drugs are mainly iron, and health supplements are mainly vitamins and DHA), oxygen inhalation after 36 weeks of pregnancy (on medical advice or on the mother’s own will). There was also no statistically significant difference between the groups with or without oxytocin and glucose solution without electrolytes before delivery and the time of umbilical clamping (P > 0.05)(Table 1). Table 1. Baseline demographic and clinical characteristics of maternalCharacteristic≤60s(n = 134)61–89 s(n = 106)≥90s(n = 105)PAge (year)30.99 ± 3.9830.95 ± 4.2330.93 ± 3.86> 0.990Age at menarche (year)0.890 ≤ 14115(85.8)93(87.7)90(85.7) > 1419(14.2)13(12.3)15(14.3)BMI (kg/m^2^) Pre-pregnancy21.83 ± 3.6921.91 ± 2.7521.65 ± 3.160.560 Antenatal26.75 ± 4.1926.83 ± 3.6926.98 ± 3.280.930Occupation0.036^#^ Civil servant23 (17.0)34 (32.0)19 (18.0) Professional and technical staff50 (37.0)37 (35.0)45 (43.0) Other61 (46.0)35 (33.0)41 (39.0)Education0.880 High level31 (23.0)21 (20.0)24 (23.0) Middle level61 (46.0)55 (52.0)48 (46.0) Low level42 (31.0)30 (28.0)33 (31.0)Smoking during pregnancy0.640 Yes2 (1.0)0 (0.0)1 (1.0) No132 (99.0)106 (100.0)104 (99.0)Passive smoking before pregnancy0.370 Yes28 (21.0)15 (14.0)21 (20.0) No106 (79.0)91 (86.0)84 (80.0)Drinking alcohol before pregnancy0.670 Yes2 (1.0)1 (1.80)0 (0.0) No132 (99.0)105 (98.20)105 (100.0)History of chronic illness0.019^^ Yes22 (16.4)14 (13.2)5 (4.8) No112 (83.6)92 (86.8)100 (95.2)Drugs or health supplements during pregnancy0.840 Yes109 (81.0)87 (82.0)83 (79.0) No25 (19.0)19 (18.0)22 (21.0)Oxygen inhalation after 36 weeks of pregnancy0.220 Yes23 (17.2)10 (9.0)14 (13.0) No111 (82.8)96 (91.0)91 (87.0)Pregnant mother’s blood type (ABO)0.100 A27 (20.0)28 (26.0)31 (30.0) B48 (36.0)31 (29.0)40 (38.0) AB16 (12.0)16 (15.0)4 (4.0) O43 (32.0)31 (29.0)30 (28.0)Pregnant mother’s blood type (RH)0.600 RH (+)132 (99.0)105 (99.0)102 (97.0) RH (−)2 (1.0)1 (1.0)3 (3.0)Spouse’s blood type (ABO)0.091 A20 (15.0)19 (18.0)8 (8.0) B75 (56.0)50 (47.0)54 (51.0) AB12 (9.0)10 (10.0)19 (18.0) O27 (20.0)27 (25.0)24 (23.0)Spouse’s blood type (RH)> 0.990 RH (+)133 (99.0)106 (100.0)105 (100.0) RH (−)1 (1.0)0 (0.0)0 (0.0)Gestation0.460 160 (45.0)43 (40.60)43 (41.0) 245 (34.0)42 (39.60)32 (30.0) ≥ 329 (22.0)21 (19.80)30 (29.0)Production0.650 181 (60.0)66 (62.0)59 (56.0) ≥ 253 (40.0)40 (38.0)46 (44.0)Live0.720 182 (61.0)66 (62.0)60 (57.0) ≥ 252 (39.0)40 (38.0)45 (43.0)Abortion0.120 091 (68.0)70 (66.0)64 (61.0) 128 (21.0)20 (19.0)33 (31.0) ≥ 215 (11.0)16 (15.0)8 (8.0)Gestational age (days)276.46 ± 7.03276.85 ± 6.98277.49 ± 6.690.540Oxytocin0.820 Yes47 (34.0)41 (38.0)40 (39.0) No87 (66.0)65 (62.0)65 (61.0)Glucose solution without electrolytes use0.470 Yes5 (4.0)2 (2.0)5 (5.0) No129 (96.0)104 (98.0)100 (95.0)Assisted reproductive technologies0.631 Yes1(0.8)1(0.9)0(0.0) No133(99.2)105(99.1)105(100.0)Normal continuous variables: mean ± SD. Skewed continuous variables: median (IQR). Categorical variables: n, %. SD, Standard Deviation. IQR, Interquartile Range.^#^The significance values were adjusted for multiple testing by Bonferroni correction and statistically significant differences were found between ≤60s group and 61–89 s group in civil servant^^The significance values were adjusted for multiple testing by Bonferroni correction and statistically significant differences were found between ≤60s group and ≥ 90s group in Yes and No
Maternal blood routine examination
Differences in maternal PCT (Plateletcrit) within 7 days antenatal were statistically significant in different neonatal cord natural clamping of pulsation time groups. Differences in routine hematological indices at 24 hours postpartum were not statistically significant in the different subgroups (Supplemental Table 1).
Indicators related to the postnatal period of maternal
There were no statistically significant differences between the three groups in postnatal indicators, such as the amount of bleeding and medication taken by the mothers (P > 0.05) (Table 2). Table 2. Postnatal indicators in mothers with different times of natural cessation of umbilical cord pulsationCharacteristic≤60s(n = 134)61–89 s(n = 106)≥90s(n = 105)PBleeding (ml) 2 hours after delivery230.00 (210.00, 259.00)230.00 (210.00, 257.75)220.00 (200.00, 250.00)0.280 24 hours after delivery370.00 (320.00, 441.00)365.00 (315.75, 420.00)375.00 (335.00, 440.00)0.600Iron within 42 days after delivery0.960 Yes14 (10.4)11 (10.4)12 (11.4) No120 (89.6)95 (89.6)93 (88.6)Medication or other health supplements within 42 days of delivery0.380 Yes30 (22.4)20 (18.9)16 (15.2) No104 (77.6)86 (81.1)89 (84.8)Normal continuous variables: mean ± SD. Skewed continuous variables: median (IQR). Categorical variables: n, %. SD, Standard Deviation. IQR, Interquartile Range
Characteristics of newborns after grouping according to the time of natural cessation of umbilical cord pulsation
The gender distribution of newborns was balanced among the three groups, with a male-to-female ratio of 75 (55.9%) vs 59 (44.1%), 62 (58.5%) vs 44 (41.5) %, and 52 (49.5%) vs 53 (50.5%) respectively. There was a statistically significant difference in the birth weight of newborns in the different time of umbilical cord clamping groups. As weight increased, the time to natural cessation of the umbilical cord pulsation was correspondingly longer in newborns (P < 0.05). Similarly, there was a statistically significant difference between the three groups in the number of days the umbilical cord was detached in newborns. The number of days of umbilical cord detachment decreased with increasing time of cord clamping (P < 0.05). As the time of natural cessation of umbilical cord pulsation increased, there were no statistically significant differences in cord blood nucleated cell counts and cord blood pH among the three groups, except for the differences in cord and placenta related indices among the three groups (P < 0.05). All newborns had Apgar scores of 10 at 1, 5 and 10 minutes (Table 3). Table 3. Demographic and clinical characteristics of infants at different times of umbilical cord clampingCharacteristic≤60s(n = 134)61–89 s(n = 106)≥90s(n = 105)PGender0.400 Male75 (55.9)62 (58.5)52 (49.5) Female59 (44.1)44 (41.5)53 (50.5)Length(cm)50.49 ± 2.1550.59 ± 2.0050.91 ± 2.020.210Weight(g)3316.27 ± 356.703387.26 ± 379.203455.52 ± 363.780.037^a^Umbilical cord abscission12.00 (8.00, 15.75)10.00 (7.00, 15.00)9.00 (7.00, 13.00)0.008^a^Cord blood Mass (g)32.00 (23.40, 43.82)32.00 (21.92, 41.42)34.20 (24.50, 45.60)0.330 Volume (ml)56.00 (46.00, 68.00)56.00 (46.00, 70.00)60.00 (48.00, 68.00)0.370 Total nucleated cells2.83 (1.45, 4.34)3.11 (1.81, 5.80)3.55 (2.00, 5.04)0.040Placenta Weight (g)536.32 ± 104.23536.84 ± 106.55555.15 ± 98.230.250 Volume (cm^3^)758.21 ± 156.00746.72 ± 164.68753.49 ± 154.490.890Umbilical cord length (cm)60.28 ± 13.1559.28 ± 9.0558.62 ± 11.310.930pH7.33 ± 0.077.30 ± 0.077.30 ± 0.060.010^a^pO_2_27.80(21.93, 32.73)25.05(21.03, 29.88)27.00(20.43, 31.33)0.146pCO_2_42.31 ± 9.2544.55 ± 9.4644.20 ± 7.640.111Apgar 1 minute– 10134 (100%)106 (100%)105 (100%)Apgar 5 minutes– 10134 (100%)106 (100%)105 (100%)Apgar 10 minutes– 10134 (100%)106 (100%)105 (100%)Symptomatic polycythemia0.210 Yes10 (7.5)3 (2.8)4 (3.8) No124 (92.5)103 (97.2)101 (96.2)Normal continuous variables: mean ± SD. Skewed continuous variables: median (IQR). Categorical variables: n, %. SD, Standard Deviation. IQR, Interquartile Range.^a^The significance values were adjusted for multiple testing by Bonferroni correction and statistically significant differences were found between ≤60s group and ≥ 90s group
Infants blood routine examination
Among the routine blood indicators of newborns within 24 hours of birth, there were statistically significant differences in WBC, RBC, LYM, PCV and HGB among the subgroups at different times of umbilical cord clamping. Furthermore, LYM (7.41 ± 2.16%), PCV (61.77 ± 8.17%) and HGB (194.52 ± 25.84 g/L) all reached their maximum in the 61–89 s group (Table 4). Table 4. Blood count within 24 hours after delivery of the newbornCharacteristic≤60s(n = 134)61–89 s(n = 106)≥90s(n = 105)PWBC (× 10^9^/L)21.03 ± 7.9220.80 ± 4.8519.44 ± 5.900.043^b^NEU (×10^9^/L)53.22 ± 9.0154.40 ± 8.2354.54 ± 9.510.120LYM (×10^9^/L)36.94 ± 8.8536.11 ± 7.8735.89 ± 9.940.180EOS (×10^9^/L)2.60 (1.75, 3.20)2.55 (1.90, 3.70)2.80 (2.00, 3.50)0.370BAS (×10^9^/L)0.30 (0.10, 0.40)0.30 (0.20, 0.50)0.30 (0.20, 0.40)0.580MON (×10^9^/L)6.50 ± 1.696.12 ± 1.576.21 ± 1.630.062PLT (×10^9^/L)265.04 ± 81.04266.10 ± 74.61244.37 ± 82.010.200RBC (× 10^12^/L)5.41 ± 1.045.40 ± 0.815.31 ± 0.640.045^a^NEU (%)11.20 ± 4.7611.41 ± 3.6210.67 ± 3.690.280LYM (%)7.39 ± 1.987.41 ± 2.166.91 ± 2.850.006^a,b^EOS (%)0.51 (0.34, 0.69)0.50 (0.38, 0.75)0.50 (0.37, 0.65)0.650BAS (%)0.05 (0.02, 0.09)0.06 (0.03, 0.09)0.05 (0.03, 0.08)0.190MON (%)1.29 (1.04, 1.61)1.24 (0.97, 1.53)1.15 (0.94, 1.42)0.066PCV/Hct (%)61.28 ± 11.1061.77 ± 8.1759.91 ± 6.890.007^a^HGB (g/L)190.26 ± 44.50194.52 ± 25.84187.88 ± 27.170.010^a^MCV (fL)111.71 ± 13.69111.82 ± 14.88110.81 ± 14.920.480MCH (pg)35.90 ± 1.7235.94 ± 1.5835.70 ± 1.530.490MCHC (g/L)309.45 ± 48.00312.71 ± 32.76316.24 ± 11.780.510RDW (%)16.55 ± 4.2516.71 ± 4.5316.74 ± 4.550.920PDW (fL)16.60 (16.20, 17.00)16.60 (16.30, 17.00)16.60 (16.40, 16.90)0.780MPV (fL)9.50 (9.00, 9.90)9.40 (8.93, 9.80)9.40 (8.90, 9.90)0.910PCT (%)0.26 (0.21, 0.31)0.25 (0.22, 0.30)0.26 (0.19, 0.30)0.540IQR Interquartile Range, SD Standard Deviation, WBC White Blood Cell Count, NEU Neutrophil, LYM Lymphocyte, EOS Eosinophil, BAS Basophils, MON Monocytes, PLT Platelet Count, RBC Red Blood Cell Count, PCV Packed Cell Volume, HGB Hemoglobin, MCV Mean Corpuscular Volume, MCH Mean Corpuscular Hemoglobin, MCHC Mean Corpuscular Hemoglobin Concentration, RDW Red Cell Distribution Width, PDW Platelet Distribution Width, MPV Mean Platelet Volume, PCT Plateletcrit^a^The significance values were adjusted for multiple testing by Bonferroni correction and statistically significant differences were found between ≤60s group and ≥ 90s group^b^The significance values were adjusted for multiple testing by Bonferroni correction and statistically significant differences were found between 61-89s group and ≥ 90s group
Neonatal bilirubin and the incidence of neonatal hyperbilirubinemia
Bilirubin concentrations as detected by transcutaneous measurements at six time points: 24 hours, 48 hours, 72 hours, 5 days, 10 days and 42 days after the birth of the newborn showed statistically significant differences at different time points of measurement(P < 0.05), and the differences were not statistically significant in different subgroups of time to natural cessation of umbilical cord pulsation. Differences in the interaction of measurement time points and grouping factors were also not statistically significant (P > 0.05)(Supplemental Table 2). The Bonferroni post-hoc test showed a statistically significant difference between the ≤60s and ≥ 90s groups, with the ≥90s being higher than the ≤60s group at all different time points of measurement. Similarly, there was a statistically significant difference between the six measurement time points, with the maximum transcutaneous bilirubin reaching 5 days after birth in newborns (Supplemental Fig. 1). The difference in the incidence of neonatal hyperbilirubinemia on the tenth day of life was statistically significant between the three groups at 10 days after birth, with multiple comparisons revealing a statistically significant difference between the 61–89 seconds (0.0%) and ≥ 90 seconds (4.8%) groups (Table 5). Table 5. Incidence of hyperbilirubinemia in neonates at six time points in groups with different times of cessation of cord pulsation after birthCharacteristic≤60s(n = 134)61–89 s(n = 106)≥90s(n = 105)PTime (after birth), (n, %)24 hours0.380 Yes4(3.0)5(4.7)7(6.7) No130(97.0)101(95.3)98(93.3)48 hours0.150 Yes1(0.7)03(2.9) No133(99.3)106(100.0)102(97.1)72 hours0.320 Yes5(3.7)1(0.9)2(1.9) No129(96.3)105(99.1)103(98.1)5 days0.390 Yes5(3.7)5(4.7)8(7.6) No129(96.3)101(95.3)97(92.4)10 days0.020^b^ Yes1(0.7)05(4.8) No133(99.3)106(100.0)100(95.2)42 days> 0.990 Yes1(0.7)1(0.9)0 No133(99.3)105(99.1)105(100.0)^b^The significance values were adjusted for multiple testing by Bonferroni correction and statistically significant differences were found between 61-89s group and ≥ 90s group
Use of health products or medicines for newborns
The study revealed that group of ≤60s had a higher utilization for health supplements (product packaging printed on the “health food” that is health supplements) or medication compared to group of 61–89s, with the sixth time point serving as the baseline. There was a notable statistical difference in the utilization for health supplements or medication between the two groups, with the difference becoming significant from the second time point onwards (P < 0.001). Additionally, as the observation period increased, the utilization for health supplements or medication among newborns also increased. Similarly, the need was higher in group of 61–89s compared to group of ≥90s (Supplemental Table 3, Supplemental Table 4).
Discussion
The aim of the prospective cohort study was to compare the effects of different times of natural cord cessation on maternal and infant outcomes, in order to explore the most beneficial time of cord clamping for maternal and infant outcomes.
The time of natural cessation of umbilical cord pulsation may be related to the influence of factors, such as cord length and cord hemodynamics [3, 14]. In our study, neonatal umbilical cords stopped pulsing naturally at the time range of 10.00–403.00s, with a median duration of 68.00s (IQR: 54.00–95.00). Although most full-term neonates’ umbilical cord pulsing stop within 2 min of birth, there is study suggesting that the median duration of umbilical cord pulsing is 213.00s (IQR: 120.00–420.00) [15]. There is also study suggesting that the natural cessation of umbilical cord pulsation in neonates may be extraordinarily prolonged (the mean clamping time in the DCC group was 305 s) [16].
The present study showed that the timing of cord arrest was not affected by the mother’s blood count, including hemoglobin, within 7 days prior to delivery and 24 hours after delivery. Routine blood count is one of the most important indicators for assessing the health status of the mother and baby. Although they can provide information on the health status of the mother and baby, they are not the only factor in determining the time of umbilical cord breakage and the outcome of the mother and baby. In some cases, routine blood indicators may affect the timing of cord cutting and maternal and infant outcomes. Delayed umbilical cord clamping needs to be carefully considered and monitored in cases of maternal anemia or other risk factors associated with anemia [17]. Therefore, special attention should be paid to maternal hemoglobin levels and anemia status when considering the timing of umbilical cord cutting.
Postpartum hemorrhage (PPH) is the leading cause of maternal death in low-income countries, accounting for almost a quarter of all maternal deaths worldwide. PPH is defined as bleeding≥500 ml within 24 hours after the fetus is delivered [18]. In general, there is concern that the prolonged wound closure in the DCC group leads to a longer operative time and thus increased maternal blood loss. However, the study shows that the time of natural arrest of the umbilical cord in newborns does not have an effect on the amount of maternal postpartum hemorrhage (PPH). A meta-analysis by Judith Gomersall, MCom et al. that included 33 studies came to a similarly conclusion that early or late umbilical cord clamping may have little effect on maternal complications, including PPH (≥500 ml) [19].
For newborns, there may be a correlation between the weight of the newborn, the time when the umbilical cord stops pulsating naturally and the time when the newborn’s umbilical cord falls off. It may be that the better the mother’s health, the better the nutrients and survival conditions the newborn receives in the womb, resulting in a heavier newborn. The mother’s well-conditioned body may support the pulsation of the umbilical cord for longer. In addition, the care of the newborn such as the length of time it takes for the cord to fall off may also vary according to the health of the mother and the weight of the fetus, with the greater birth weight of the newborn, the quicker the cord falls off.
According to a review, no significant differences were observed between early and delayed cord clamping in terms of Apgar scores below 7 at 5 minutes [6]. This is consistent with the findings of our study. However, a study by Michael Fogarty et al. showed that delayed clamping reduced the incidence of 1-minute low Apgar scores in preterm infants [20]. Demonstrate that delayed cord clamping does not adversely affect postnatal Apgar scores, at least in newborns. A number of systematic reviews and meta-analyses have similarly reported that delayed cord clamping (DCC) may be more beneficial for preterm infants, such as reducing the chance of intraventricular hemorrhage, improving hemodynamic outcomes, reducing the need for blood transfusions, reducing hospital mortality, and reduced incidence of low Apgar scores within 1 minute [20, 21]. Overall, all of the above studies may provide evidence to demonstrate that delayed cord locking does not adversely affect postnatal Apgar scores, at least in term newborns.
Anemia is one of the most critical factors contributing to neonatal and infant mortality in developing countries [22]. Previous studies of cord clamping have shown beneficial effect of DCC on hemoglobin (Hb) at birth or at different follow-up times in term neonates and demonstrated reduction in anemia. A randomized controlled trial of expected low birthweight newborns in South Africa showed that hemoglobin levels were significantly higher in the DCC (2–3 min after birth) group at 24 hours after birth, but the difference disappeared at 2 months after birth [23]. Meanwhile, a randomized controlled trial in a highly malarious rural area of Zambia found that infants in the ICC group had a faster decline in Hb levels than the DCC group throughout the observation period, and this difference disappeared by 6 months of age [16]. The hematological benefit of DCC disappears after 4 months and may be related to the iron content of the infant’s body, partly due to increased iron stores during growth and partly due to the infant losing more iron through the gastrointestinal tract during diarrhoea or during the feeding of whole milk [24]. The study found statistically significant differences in hemoglobin and erythrocyte pressure among three groups within 24 hours of birth, with a maximum in the 61–89 second group. This suggests that waiting for the umbilical cord to stop beating naturally after delivery or disconnecting it at 61–89 seconds may be beneficial to the newborn.
Bilirubin is an important cytoprotective agent for brain tissue, enhancing its antioxidant defenses to a certain extent. Higher levels of bilirubin within the normal range can provide protective antioxidant effects to the developing brain [25]. A retrospective cohort study of 424 newborns showed that a delayed umbilical weaning regimen for term newborns was associated with significantly higher mean transcutaneous bilirubin levels [26]. This is consistent with our findings. Results of a randomized controlled trial including 73 study participants showed no increase in adverse effects such as hyperbilirubinemia or symptomatic polycythemia in infants who received DCC (≥5 minutes) between 24 and 48 hours [4].
Instead of randomizing the pregnants to ECC or DCC groups based on artificial umbilical cord disconnection in most of the randomized clinical trials, the present study explored the more favourable umbilical cord disconnection time for maternal and infant outcomes by waiting for the umbilical cord to stop pulsing naturally before disconnecting the umbilical cord, which is an issue that has been paid less attention to in the published studies. Additionally, we followed up some of the outcomes, and the results of the present study may provide new evidences to support the optimal umbilical cord disconnection time for newborns born full-term via vaginal delivery. This study has several limitations. Firstly, the study only included newborns born at term in singleton pregnancies delivered vaginally, so the findings may not be generalizable to multiple pregnancies, preterm births and cesarean sections, and further studies are needed to assess the impact of delayed umbilical cord clamping on maternal and infant outcomes in these circumstances. Secondly, the study did not follow up the mother and newborn for a longer period of time to examine the long-term effects of the time to spontaneous cord arrest on maternal and infant outcomes.
Conclusions
Prolonged cessation of the natural pulsation of the umbilical cord may lead to increased hemoglobin levels in the newborn, but does not increase the risk of postnatal hemorrhage in the mother. It is recommended that the umbilical cord is cut within 61–89 seconds of delivery as this may be more beneficial to the health of the newborn and the recovery of the mother.
Supplementary Information
Supplementary Material 1. Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yao AC Hirvensalo M Lind J Placental transfusion-rate and uterine contraction Lancet.1968138038310.1016/S 0140-6736(68)91352-44169972 · doi ↗ · pubmed ↗
- 2Yao AC Moinian M Lind J Distribution of blood between infant and placenta after birth Lancet.1969287187310.1016/S 0140-6736(69)92328-94186454 · doi ↗ · pubmed ↗
- 3Boere I Roest AA Wallace E Ten Harkel AD Haak MC Umbilical blood flow patterns directly after birth before delayed cord clamping Arch Dis Child Fetal Neonatal Ed.2015100 F 121F 12510.1136/archdischild-2014-30714425389141 · doi ↗ · pubmed ↗
- 4Mercer JS Erickson-Owens DA Collins J Barcelos MO Parker AB Effects of delayed cord clamping on residual placental blood volume, hemoglobin and bilirubin levels in term infants: a randomized controlled trial J Perinatol.20173726026410.1038/jp.2016.22227929530 PMC 5334141 · doi ↗ · pubmed ↗
- 5Mohammad K Tailakh S Fram K Creedy D Effects of early umbilical cord clamping versus delayed clamping on maternal and neonatal outcomes: a Jordanian study J Matern Fetal Neonatal Med.20213423123710.1080/14767058.2019.160260330931665 · doi ↗ · pubmed ↗
- 6Mc Donald SJ, Middleton P, Dowswell T, Morris PS. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst Rev. 2013:3.10.1002/14651858.CD 004074.pub 3PMC 654481323843134 · doi ↗ · pubmed ↗
- 7Kc A Rana NMålqvist M Jarawka Ranneberg L Subedi K Effects of delayed umbilical cord clamping vs early clamping on Anemia in infants at 8 and 12 months: a randomized clinical trial JAMA Pediatr.201717126427010.1001/jamapediatrics.2016.397128114607 · doi ↗ · pubmed ↗
- 8Qian Y Ying X Wang P Lu Z Hua Y Early versus delayed umbilical cord clamping on maternal and neonatal outcomes Arch Gynecol Obstet.201930053154310.1007/s 00404-019-05215-831203386 PMC 6694086 · doi ↗ · pubmed ↗