Tracheal Deviation and Airway Management: Clinical Considerations From a Cadaver
Takutoshi Inoue, Toru Yamamoto

TL;DR
This paper highlights the challenges of airway management in patients with severe tracheal deviation due to unusual aortic anatomy, using a cadaver case to emphasize the need for detailed anatomical knowledge.
Contribution
The paper presents a unique cadaver case with meandering multiple aortas causing tracheal deviation and outlines clinical risks for airway management.
Findings
Severe tracheal deviation was associated with difficulty in tracheal intubation and ventilation.
The tortuous brachiocephalic artery posed a risk of hemorrhage during emergency tracheostomy.
Anatomical knowledge is critical for safe airway management in such cases.
Abstract
Severe tracheal deviation detected on preoperative chest radiographs is one of the risk factors for difficult tracheal intubation and difficulty in ventilation using an endotracheal tube after tracheal intubation when managing the airway through tracheal intubation under general anesthesia. In this report, we describe the cadaver of an 81-year-old woman with marked tracheal deviation due to meandering multiple aortas. This report details the importance of anatomical knowledge in developing a detailed airway management plan. The deviated trachea was removed from the cadaver and the tracheal tube was inserted at the glottis to the proximal end of the glottal marker. The tube tip was in contact with the tracheal wall, suggesting ventilation difficulty during intubation. The tortuous brachiocephalic artery passed in front of the trachea, which posed a risk of massive aortic hemorrhage and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
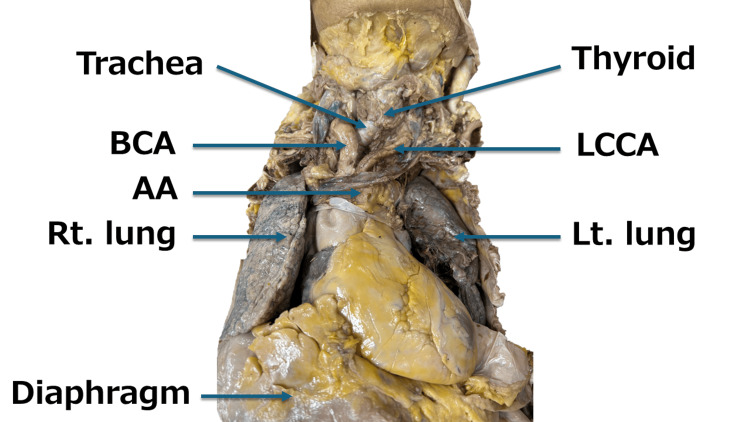 Figure 1
Figure 1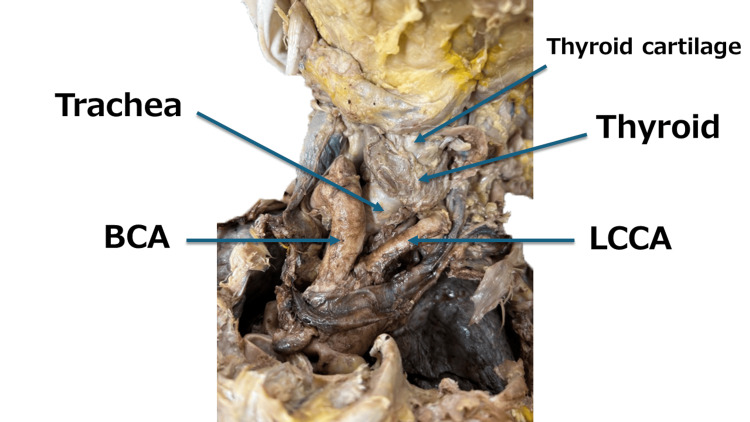 Figure 2
Figure 2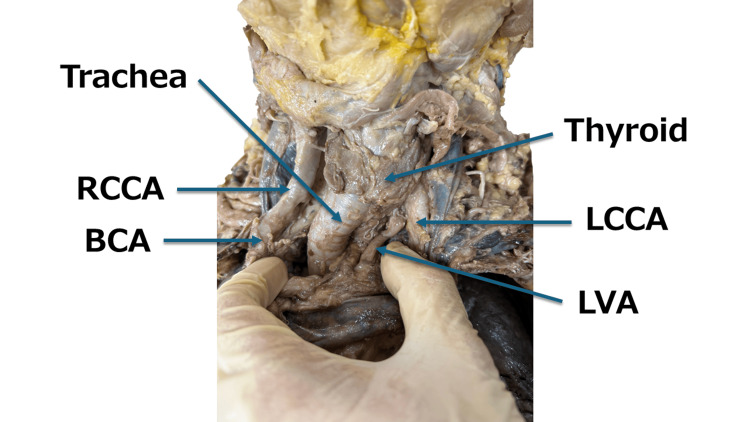 Figure 3
Figure 3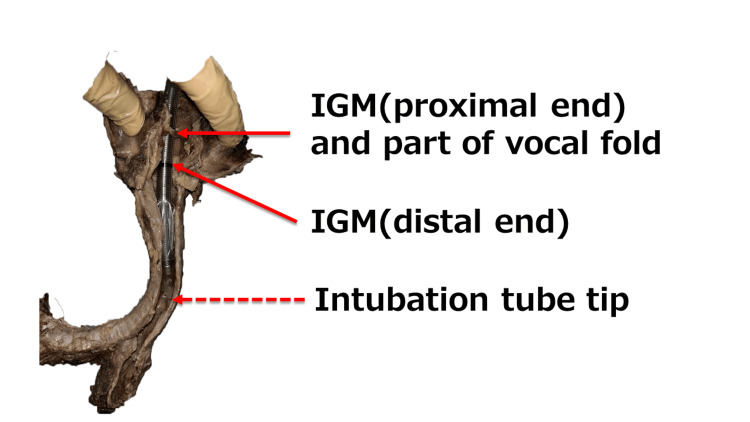 Figure 4
Figure 4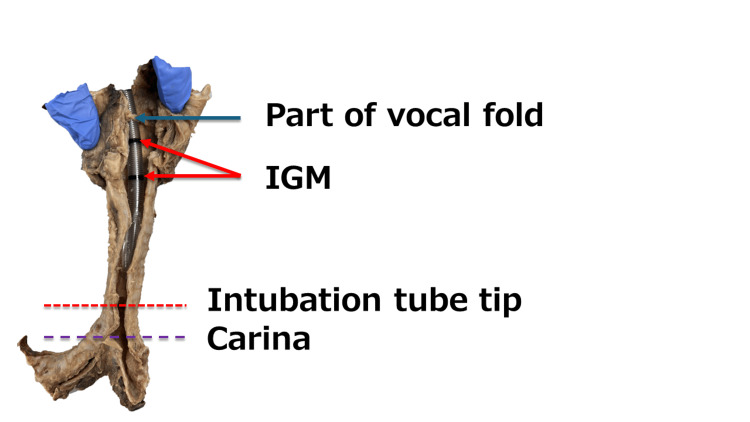 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Tracheal and airway disorders · Trauma Management and Diagnosis
Introduction
Tracheal deviation is sometimes seen on preoperative chest radiographs. Tracheal deviation is defined as trachea shifts to one side from its normal position in the neck or chest. There are several causes of tracheal deviation, including thyroid disease [1] and meandering of the aortic arch (AA) [2]. Although the epidemiological frequency of occurrence is unclear, severe tracheal deviation during tracheal intubation under general anesthesia is a risk factor for difficult intubation during induction of general anesthesia [3,4] and difficulty in ventilation with an endotracheal tube after tracheal intubation [5,6]. Here, we report a case of tracheal deviation due to the meandering of multiple aortas during anatomical practice at Teikyo University School of Medicine in 2023 along with some findings.
Case presentation
This case presentation was performed in accordance with the requirements of the Declaration of Helsinki. The authors followed the guidelines for the research involving cadavers established by the Japanese Association of Anatomists for this report.
This case report involved an 81-year-old female with a height of 155 cm, weight of 70 kg, and body mass index of 29.1 kg/m^2^. The main cause of death was hepatocellular carcinoma, and the subject had indications of cardiac hypertrophy. No other information regarding prenatal history was available. However, hepatocellular carcinoma suggested hepatitis or liver cirrhosis. For anatomy practice, formalin was injected through the left femoral artery and then the subject was embalmed with formalin and alcohol. While opening and dissecting the thoracic cavity (Figure 1), we observed that the trachea was just above the AA and had deviated significantly to the right. The brachiocephalic artery (BCA) and right common carotid artery (RCCA) were tortuous and the BCA meandered across the anterior wall of the trachea (Figures 2, 3).
The heart and its surroundings (front).When the thoracic cavity was opened, hypertrophy of the left ventricle (LVH) with a cardiothoracic ratio (CTR) exceeding 50% was first observed. Next, a meandering brachiocephalic artery (BCA) passed across the anterior wall of the trachea, narrowing between the thyroid and BCA. In addition to this, the aortic arch (AA), left common carotid artery (LCCA), left lung (Lt. lung), and right lung (Rt lung) were also observed.
Head and neck arteries and trachea (front).A magnified image of the head and neck (front) is shown.BCA: brachiocephalic artery; LCCA: left common carotid artery
Head and neck arteries and trachea (front).To confirm tracheal deviation, the brachiocephalic artery (BCA) and left common carotid artery (LCCA) were retracted in the lateral direction. As a result, not only tracheal deviation but also meandering of the right common carotid artery (RCCA) was observed.LVA: left vertebral artery
The trachea was removed and a longitudinal incision was made in the midline on the posterior surface, maintaining the tortuous trachea’s shape. Tracheal deviation was confirmed when the chest cavity was opened, so a soft spiral tube (ShileyTM Oral/Nasal Tracheal Tube Cuffed 6.5mm I.D., COVIDIEN) was selected. When a tube was inserted and fixed at the proximal end of the glottis marker (IGM: Intubation Guide Mark), the tube tip contacted the trachea wall (Figure 4). The IGM’s position was examined when the tube tip was fixed 2 cm above the tracheal bifurcation. The trachea was stretched straight for accurate caliper and ruler measurements. The tip of the tube was fixed 2 cm above the tracheal bifurcation, and the IGM was located below the vocal cord folds (Figure 5).
Trachea and intubation tube 1.When the tube was fixed at the proximal end of the glottis marker (IGM), the tip of the intubation tube contacted the tracheal wall.IGM: Intubation Guide Mark
Trachea and intubation tube 2.When the tip of the intubation tube was fixed 2 cm above the tracheal bifurcation, the glottal marker (IGM) was located below the vocal folds.IGM: Intubation Guide Mark
Discussion
In the present case, the trachea was compressed and deformed by the BCA and RCCA meandering. In a previous case report, we experienced cases of right common carotid tortuosity and thickening of the BCA that could have complicated a stellate ganglion block, but the cadavers did not have brachiocephalic tortuosity or tracheal deviation [7]. However, this case revealed that the trachea may be compressed and deviated when aortic meandering is aggravated. Although aortic meandering is difficult to quantify, it can be confirmed as an image using three-dimensional ultrasound [7].
Carotid tortuosity, observed here, is a common clinical condition in which the brachiocephalic or carotid artery meanders and elongates, appearing as a pulsatile neck mass [7]. These arteries are an anatomic variant of unknown cause and are typically discovered incidentally during surgery or neck imaging. They are rarely observed as a neck mass [8]. Carotid tortuosity is more common in women than in men, is anatomically predominant on the right side, and is often associated with aging, obesity, hypertension, atherosclerosis, and cardiac hypertrophy [9]. A palpable pulse in the right supraclavicular fossa may indicate right carotid meandering, especially in women with hypertension. In these cases, a thorough examination and appropriate intraoperative and postoperative approaches should be considered [7].
As shown in Figure 4, tracheal intubation at the proximal end of the IGM allows the tube tip to come into contact with the tracheal wall, suggesting possible ventilatory difficulties during intubation. To avoid these complications, we examine the appropriate tube position and the allowable range of motion based on the preoperative chest radiographs and planned surgical procedure and then use a video laryngoscope to ensure glottic visibility during intubation. After tracheal intubation, it is considered necessary to confirm the position of the tube tip using a fiberscope and place it in an appropriate position. Repeatedly verifying the tube tip position with chest X-rays should be avoided to prevent radiation overexposure.
Several factors contribute to tracheal injury associated with intubation, including older age, being female [10], forced intubation technique, inappropriate tube size, improper stylet use, an overinflated cuff, and abnormal tube position [11]. A detailed airway management plan must be developed and a spiral tube softer than polyvinyl chloride should be used to avoid tracheal injury in older women with deviated tracheas. Furthermore, as shown in Figure 5, the IGM was positioned below the vocal folds when the tube tip was fixed 2 cm above the tracheal bifurcation, which is the ideal position for the tube tip. In a patient with significant tracheal deviation, the usual tracheal intubation methods that confirm that the IGM enters the glottis cannot be used to properly position the tube tip.
Surgical airway management, a last resort during difficult intubation, requires careful planning. In the present case, as the thyroid cartilage, cricothyroid cartilage, and thyroid gland could be dissected and there were no abnormalities around the cricothyroid mesentery, cricothyroid puncture, and incision were considered anatomically and clinically feasible. However, this case was an obese woman, and when the skin was removed, there was a lot of subcutaneous fat, making it difficult to palpate the cricothyroid membrane [12].
In this case, the BCA passed in front of the trachea, suggesting a risk of aortic bleeding during percutaneous tracheostomy and tracheo-innominate artery fistula (TIF) post-surgery. Surgical procedures in the anterior neck (e.g., percutaneous tracheostomy) in patients with high common carotid or brachiocephalic arteries carry a high risk of aortic injury. A three-dimensional analysis is needed in these situations, if possible [9]. TIF is a serious complication post-tracheostomy accompanied by massive tracheal bleeding that is reported in 0.6% of patients three to four weeks after surgery [13]. Approximately 30-50% of cases experience hemorrhage before the outbreak [13]. The prognosis is poor, with a survival rate of 10-30% [13]. Anatomical risk factors include inferior tracheostomy, history of surgery or congenital scoliosis, and deviation of the trachea and BCA due to chest deformity [13]. If an anatomic abnormality is suspected, as in the present case, preoperative imaging by computed tomography should be performed to confirm the anatomic relationship between the trachea and BCA before the tracheostomy procedure [13,14].
Conclusions
Here, we present a case of tracheal deviation due to meandering of cervical aortas to highlight potential difficulties in airway management. Tracheal deviation should be considered as a differential diagnosis when unexpected ventilation difficulties are encountered during tracheal intubation. In performing airway management, it is important not only to confirm the presence or absence of tracheal deviation using preoperative chest radiographs but also to confirm the anatomical relationship between the trachea and carotid artery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical application of fiberoptic bronchoscope combined with visual laryngeal mask awake tracheal intubation technique: a case report Am J Transl Res Cui J Tan ZQ Wang KZ Tian XL Chen XX 14621468152023 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 10006816/36915732 PMC 10006816 · pubmed ↗
- 211 cm Haughton D left cervical aortic arch aneurysm J Cardiothorac Surg Kaul P 108820132361803610.1186/1749-8090-8-108PMC 3639062 · doi ↗ · pubmed ↗
- 3Difficult endotracheal intubation secondary to tracheal deviation and stenosis in a patient with severe kyphoscoliosis: a case report Korean J Anesthesiol Kim HJ Choi YS Park SH Jo JH 3863896920162748231710.4097/kjae.2016.69.4.386PMC 4967635 · doi ↗ · pubmed ↗
- 4Difficult tracheal intubation secondary to a tracheal diverticulum and a 90 degree deviation in the trachea Anaesthesia Davies R 92392555200010.1046/j.1365-2044.2000.01664-18.x 10947774 · doi ↗ · pubmed ↗
- 5Airway obstruction during emergence from general anesthesia in a patient with tracheal deviation Anesth Resusc Alam S Sakura S Kosaka Y 185186321996 https://mol.medicalonline.jp/library/journal/download?Goods ID=ci 9masso/1996/003202/021&name=0185-0186 e&User ID=202.253.111.210
- 6Complications of endotracheal intubation and other airway management procedures Indian J Anaesth Divatia JV Bhowmick K 308318492005 https://journals.lww.com/ijaweb/Citation/2005/49040/COMPLICATIONS_OF_ENDOTRACHEAL_INTUBATION_AND_OTHER.9.aspx
- 7Tortuous carotid artery: a case report from anatomy training body and anesthetic consideration for stellate ganglion block Asian J Med Case Rep Inoue T Yamamoto T 636742022 https://globalpresshub.com/index.php/AJMCR/article/view/1613
- 8Association of tortuous common carotid artery with abnormal distribution of the ansa cervicalis: a case report Acta Medica (Hradec Kralove) Paraskevas G Koutsouflianiotis K Chrysanthou C Iliou K Syrmos N Salmas M 1291316420213433143410.14712/18059694.2021.22 · doi ↗ · pubmed ↗