Complete response of metastatic cutaneous squamous cell carcinoma and multiple locally advanced basal cell carcinomas with concomitant pembrolizumab and sonidegib therapy
Carlos González-Cruz, Eva Muñoz-Couselo, Carolina Ortiz-Velez, Berta Ferrer, Vicente García-Patos, Carla Ferrándiz-Pulido

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
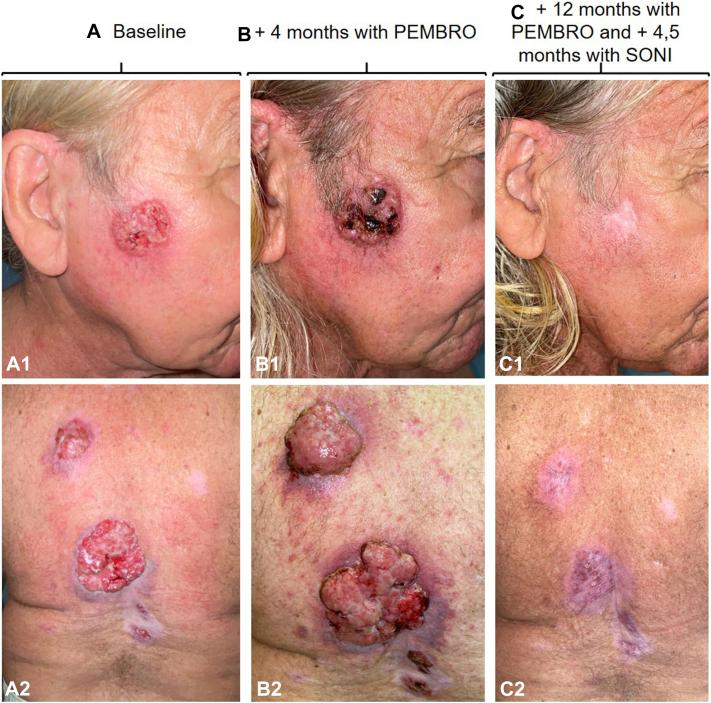 Figure 1
Figure 1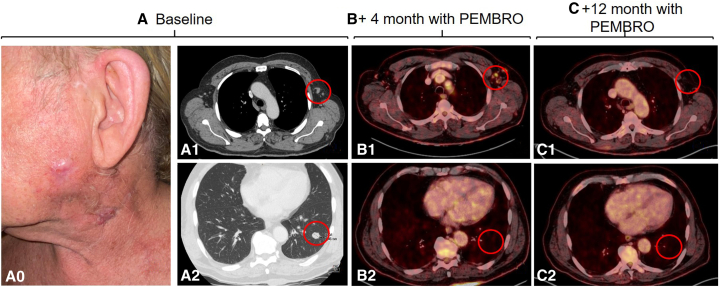 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNonmelanoma Skin Cancer Studies · Hedgehog Signaling Pathway Studies · Cancer and Skin Lesions
Introduction
The treatment of patients with metastatic cutaneous squamous cell carcinoma (cSCC) who also have multiple locally advanced (la) basal cell carcinomas (BCCs) can be challenging and requires multidisciplinary management. We present our clinical experience with concomitant treatment with pembrolizumab and sonidegib in a patient with metastatic cSCC and multiple locally advanced BCCs.
Case report
A 73-year-old man with a history of occupational exposure to mica, asbestos, rock fiber, nickel, and chromium, with multiple BCCs previously treated since the age of 40 years, was referred to our center for evaluation of keratinocyte carcinomas. Following our assessment, 18 BCCs were diagnosed located mainly on the head and trunk (Fig 1, A). Three of them were locally advanced with a diameter of >5 cm, a vegetate growth, ulcerated and invading deep structures. In addition, the patient was diagnosed with a left cervical poorly differentiated cSCC, which was completely excised for histologic diagnosis. A computed tomography scan confirmed the presence of cervical and axillary lymph nodes and pulmonary metastases, which proved to have the same histology than the cSCC (Fig 2, A) (T3N3M1, American Joint Committee on Cancer eighth edition).Fig 1. Locally advanced basal cell carcinoma (BCC) on (A1) cheek and (A2) back. B, BCCs pseudoprogression after 4 months of pembrolizumab. C, BCCs complete response after 4.5 months with sonidegib treatment and 12 months with pembrolizumab.Fig 2A, Baseline left cervical cutaneous squamous cell carcinoma. A0, Clinical image; A1, axillary lymph nodes by CT; A2, pulmonary metastases by CT. B, Dissociate response after 4 months of pembrolizumab treatment. B1, Lymph node pseudoprogression in PET/CT; B2, complete response of the lung metastases by PET/CT. C, Complete response after 12 months with pembrolizumab treatment. C1, Complete response of axillary lymph nodes by PET/CT; C2, complete maintained response of the lung metastases by PET/CT. PET, Positron emission tomography; CT, computed tomography.
The interdisciplinary tumor board decided to initiate pembrolizumab at a dose of 200 mg every 21 days for the treatment of both, the metastatic cSCC and the multiple BCCs. The patient presented an initial dissociated response, with regression of the lung metastases after 4 months of treatment but with lymph node and BCCs initial pseudoprogression (Figs 1, B and 2, B). After 8 months of treatment, the patient achieved almost radiologic complete response of the cSCC metastases, with an excellent tolerance to the treatment and only arthralgia grade 1. The response of BCCs was, however, very modest. The clinical decision was to add sonidegib 200 mg daily for the treatment of the BCCs. The patient presented a clinical complete response after 4.5 months of combined treatment (Fig 1, C), when both treatments were discontinued, due to transient elevation of grade 2 transaminases. As the complete response of the BCCs was confirmed by histologic examination, sonidegib was not reinitiated. Treatment with pembrolizumab was reinitiated and discontinued after 15 months since its initiation, presenting radiologic complete response maintained in both squamous cell carcinoma (SCC) and BCC (Figs 1, C and 2, C). The reason for discontinuation was a transient elevation of troponins without clinical manifestations (requested in a routine analysis) which was attributed to immunotherapy. At the present time, 24 months after the start of pembrolizumab and 8 months after cessation of both treatments, the patient maintains a complete response of both tumors.
Discussion
In recent years, the treatment of advanced and metastatic cSCC and laBCC has undergone a significant improvement.1^,^2
Limited case reports describe patients with both, advanced SCC and advanced BCCs exhibiting improved responses when treated sequentially with cemiplimab and sonidegib.3^,^4 The authors consider that the combination of both treatments is well tolerated, being the sonidegib-related toxicities grade 1 and 2.4
Our patient presented an even greater therapeutic challenge. He had a metastatic cSCC and multiple laBCCs. Furthermore, cemiplimab treatment is not funded in our country for the treatment of nonmelanoma skin cancer. Based on efficacy studies of pembrolizumab in the treatment of advanced cSCC and BCC,5^,^6 the interdisciplinary tumor board decided to initiate this treatment on a compassionate use basis, which achieved a complete response in metastatic cSCC. However, the response of BCC was not significant, and sonidegib was added to the treatment, and the patient achieved a complete response after only 4.5 months of treatment. As described in the aforementioned reports, we found that this combination was well tolerated and had a high synergistic effect.
To our knowledge, this is the first clinical report on the concomitant and sequential administration of pembrolizumab and sonidegib in a patient with metastatic cSCC synchronous to multiple locally advanced BCC, achieving complete response of all tumors with good tolerance to the combined treatment. BCC and cSCC are 2 different cancers and in our case immunotherapy demonstrated less efficacy in BCC than in cSCC. Immunotherapy is only indicated in laBCC in second line after progression to hedgehog inhibitors or after unacceptable toxicities to them.7
Conflicts of interest
Dr Ferrándiz-Pulido has participated in advisory boards and/or received honoraria from Sun Pharma and Sanofi. Dr Muñoz-Couselo has participated in advisory boards for Amgen, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, and Sanofi, received honoraria from Amgen, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, and Roche, and participated as principal investigator in clinical trials for Amgen, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, and Sanofi. The other authors have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moreno-Arrones O.M.Béa-Ardebol S.Mayo-Martinez F.Sonidegib as a locally advanced basal cell carcinoma therapy in real-life clinical setting: a national multicentre study Actas Dermosifiliogr 1147202356557110.1016/j.ad.2023.04.02237088285 · doi ↗ · pubmed ↗
- 2Migden M.R.Rischin D.Schmults C.D.PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma N Engl J Med 3794201834135110.1056/NEJ Moa 180513129863979 · doi ↗ · pubmed ↗
- 3Weis J.Grote C.Weichenthal M.Hauschild A.Complete response of advanced cutaneous squamous cell and basal cell carcinomas with sequential cemiplimab and sonidegib therapy J Eur Acad Dermatol Venereol 36Suppl 12022666910.1111/jdv.1740334855253 · doi ↗ · pubmed ↗
- 4Colombo E.Gurizzan C.Ottini A.The association of cemiplimab plus sonidegib for synchronous cutaneous squamous cell carcinoma and basal cell carcinoma of the head and neck: two case reports Front Oncol 132023111114610.3389/fonc.2023.1111146 PMC 1001346536925925 · doi ↗ · pubmed ↗
- 5Grob J.J.Gonzalez R.Basset-Seguin N.Pembrolizumab monotherapy for recurrent or metastatic cutaneous squamous cell carcinoma: a single-arm phase II trial (KEYNOTE-629)J Clin Oncol 382520202916292510.1200/JCO.19.0305432673170 PMC 7460151 · doi ↗ · pubmed ↗
- 6Chang A.L.S.Tran D.C.Cannon J.G.D.Pembrolizumab for advanced basal cell carcinoma: an investigator-initiated, proof-of-concept study J Am Acad Dermatol 802201956456610.1016/j.jaad.2018.08.01730145186 PMC 6839543 · doi ↗ · pubmed ↗
- 7Bossi P.Ascierto P.A.Basset-Seguin N.Long-term strategies for management of advanced basal cell carcinoma with hedgehog inhibitors Crit Rev Oncol Hematol 189202310406610.1016/j.critrevonc.2023.10406637442495 · doi ↗ · pubmed ↗