Navigating the depths: an endoscopic triumph in removing a massive duodenal polyp
Fatih Aslan, Orhun Cig Taskin, Serhat Ozer, Bahadir Hakan Oguz

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
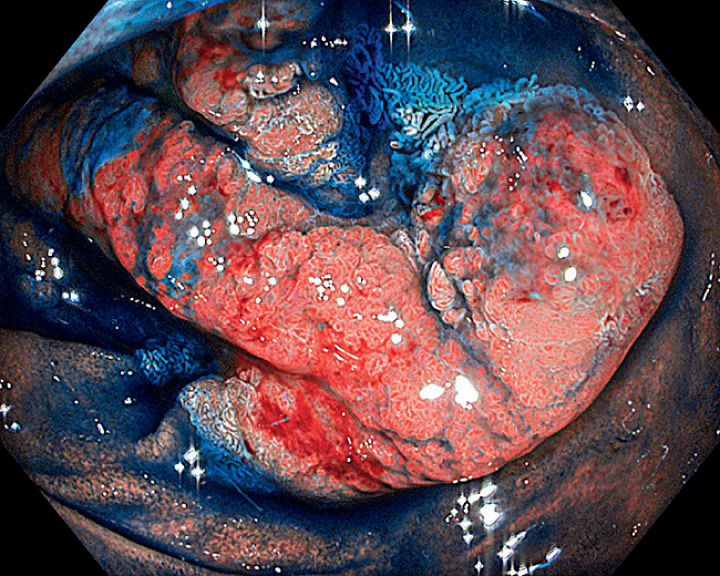 Fig. 1
Fig. 1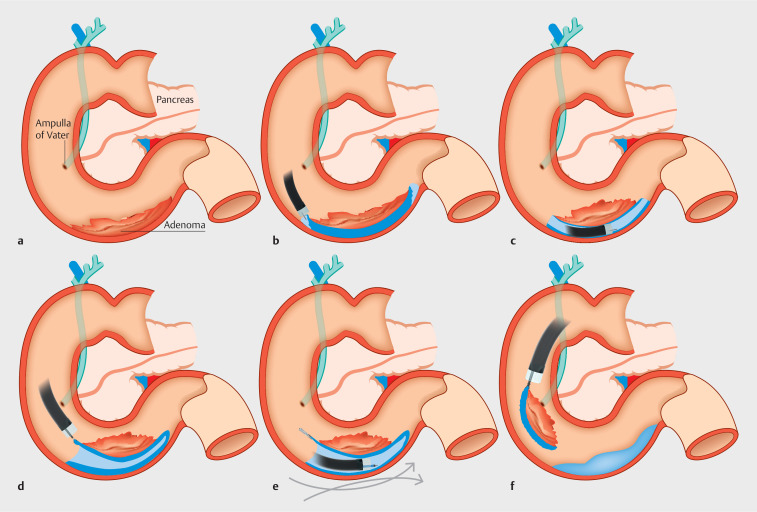 Fig. 2
Fig. 2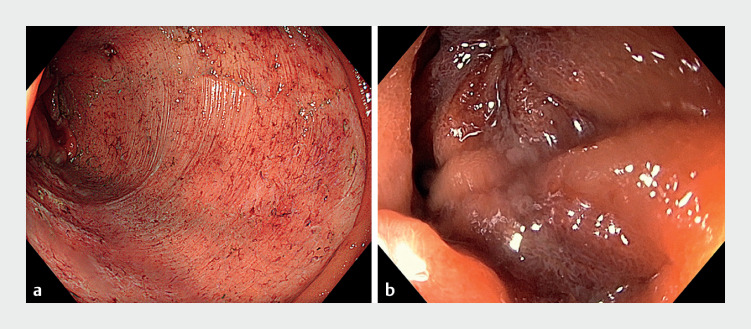 Fig. 3
Fig. 3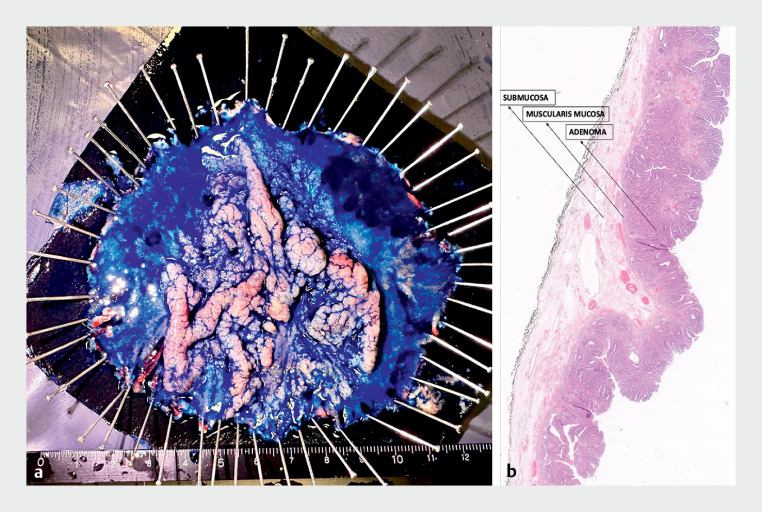 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Metastasis and carcinoma case studies
Endoscopic submucosal dissection (ESD) is a minimally invasive method for treatment of early gastrointestinal (GI) tumors at any site; however, duodenal ESD is technically challenging because of the anatomic features and high risk of complications, including bleeding and perforation 1 . Here, we report a case of en bloc removal of a distal duodenal polyp of 10 cm in length using ESD, followed by endoscopic closure.
A 57-year-old man presented with dyspepsia and fecal occult blood positivity. On upper GI endoscopy, a flat lesion of around 10 cm, with an irregular surface pattern, was noted in the third part of the duodenum, 8 cm distal to the ampulla of Vater ( Fig. 1 ). Mucosal biopsies revealed high grade dysplasia. Magnetic resonance imaging and endoscopic ultrasound were normal, except for duodenal wall thickness. Our local multidisciplinary committee recommended a surgical approach, either a Whipple operation or duodenectomy; however, the patient refused surgery and ESD was used instead ( Video 1 ).
Endoscopic view of the duodenal adenoma after the application of indigo carmine dye.
Endoscopic removal of a giant distal duodenal adenoma.Video 1
ESD was performed using a standard gastroscope with the patient under general anesthesia. The water pressure 2 , single-tunnel 3 , and single-clip traction 4 methods were used ( Fig. 2 ), resulting in en bloc removal of the lesion in 183 minutes. Given the risk of delayed perforation and bleeding, the resection area was closed with a single endoscopic Overstitch suture system, using a double-channel gastroscope ( Fig. 3 ). A nasoenteral tube was placed distal to the resection area and the patient was commenced on an oral diet after 4 hours. He was discharged on the third postoperative day, without experiencing any adverse events. The final pathology report was consistent with a tubulovillous adenoma with high grade dysplastic foci; no invasive cancer was noted ( Fig. 4 ). During follow-up endoscopy after 6 months, there was no evidence of recurrence ( Video 1 ).
Schematic view of the endoscopic submucosal dissection procedure showing: a the adenoma situated in the duodenum; b mucosal incision of the distal and proximal parts of the adenoma using the water pressure technique; c submucosal dissection of the adenoma using the single-tunnel technique; d left and right lateral mucosal incisions; e traction applied to the adenoma using the clip-traction technique; f endoscopic removal of the adenoma.
Endoscopic views of: a the resection area after completion of the endoscopic submucosal dissection; b the resection area following closure with the Overstitch suturing system.
Pathologic examination of the excised adenoma showing: a the macroscopic appearance; b the histologic appearance on hematoxylin and eosin (H&E) staining, which was consistent with an adenoma (magnification, × 2).
In conclusion, distal duodenal ESD, when combined with certain methods, is a safe and effective method in experienced hands and can be a reasonable alternative to surgery. In addition, we are of the opinion that the endoscopic Overstitch system can prevent delayed complications, even for large resection areas, and that early enteral feeding helps faster recovery.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kato M Kanai T Yahagi N Endoscopic resection of superficial non-ampullary duodenal epithelial tumor DEN Open 20222 e 5410.1002/deo 2.5435310765 PMC 8828234 · doi ↗ · pubmed ↗
- 2Kato M Takatori Y Sasaki M Water pressure method for duodenal endoscopic submucosal dissection (with video)Gastrointest Endosc 20219394294932853646 10.1016/j.gie.2020.08.018 · doi ↗ · pubmed ↗
- 3Aslan F Akpinar Z Kucuk M Single tunneling technique for treatment of giant laterally spreading tumor with endoscopic submucosal dissection Video GIE 2017215515729905280 10.1016/j.vgie.2017.01.022PMC 5990989 · doi ↗ · pubmed ↗
- 4Hasatani K Yoshida N Aoyagi H Usefulness of the clip-and-snare method using the pre-looping technique for endoscopic submucosal dissection of gastric neoplasia: a randomized controlled trial Ann Gastroenterol 202235485510.20524/aog.2021.067934987288 PMC 8713345 · doi ↗ · pubmed ↗