Multiple Muscle Metastases as the First Presentation of Gastric Cancer: A Case Report and Review of Literature
Polyxeni Pichioni, Dimitrios Kokkinovasilis, Stylianos Stylianou, Georgios Kipouridis, Alkiviadis Kalogeropoulos, Saant Al Mogrampi

TL;DR
A rare case of gastric cancer first showing as multiple muscle metastases in the abdominal wall is presented, with successful treatment and ongoing survival.
Contribution
Reports a rare initial presentation of gastric cancer with muscle metastases and reviews existing literature on similar cases.
Findings
A 45-year-old female presented with gastric cancer first detected through abdominal wall and skeletal muscle metastases.
Systemic chemotherapy led to a reduction in muscle lesions and the patient remains alive 17 months post-diagnosis.
Literature review highlights the rarity of muscle metastases as the initial manifestation of gastric cancer.
Abstract
The presence of an abdominal wall mass may serve as the initial presentation of an unknown gastric malignancy. The invasion of the abdominal wall and the occurrence of multiple skeletal muscle metastases originating from gastric cancer are exceedingly uncommon. We present a case of a 45-year-old female patient exhibiting widespread abdominal wall infiltration and skeletal muscle metastases derived from gastric cancer. The primary presentation included a distressing diffuse abdominal mass in the left upper and lower quadrants. Abdominal computed tomography revealed extensive swelling of multiple skeletal muscles within the abdominal wall, raising suspicions of gastric malignancy. Biopsies of the affected muscles, along with upper gastrointestinal tract endoscopy and colonoscopy, were performed. The upper endoscopy examination unveiled a poorly differentiated diffuse-type gastric…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
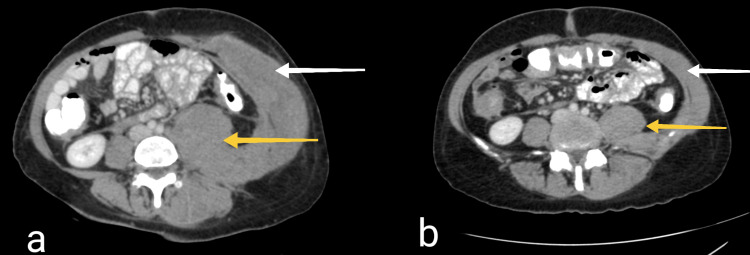 Figure 1
Figure 1| Authors | Year | Age | Sex | Other sites of metastasis | Treatment | Survival |
| Chu et al. [ | 1995 | 61 | Female | Many adjacent organs | Gastrectomy, resection of affected organs | 6 months (alive) |
| Katsumoto et al. [ | 2007 | 68 | Female | Abdominal tumors | Distal gastrectomy, systemic chemotherapy | Not Available |
| Carlomagno et al. [ | 2015 | 81 | Female | Transverse mesocolon | Gastrectomy, transverse colon and abdominal wall resection | Died 20 days post-operation |
| Cho et al. [ | 2015 | 71 | Female | None | Gastrectomy, partial resection of abdominal wall | Died 3 months post-operation |
| Misumi et al. [ | 2019 | 76 | Male | None | Distal gastrectomy, repeated extractions of abdominal wall masses | 1 year and 6 months post operation (alive) |
| Nakamura et al. [ | 2021 | 70 | Male | Transverse colon | Gastrectomy, transverse colon and abdominal wall resection, chemotherapy | 6 months post operation (alive) |
| Fukui et al. [ | 2021 | 75 | Male | Port site metastasis, left gluteal subcutaneous metastasis | Laparoscopic total gastrectomy, mass resection, radiotherapy | 78 months post gastrectomy (alive) |
| This study | 2024 | 45 | Female | Multiple muscle metastases, peritoneal dissemination | Systemic chemotherapy | 17 months (alive) |
| Authors | Year | Age | Sex | Sites of muscle metastases | Other sites of metastases | Treatment for gastric cancer | Treatment for muscle metastases | Survival after the muscle metastasis diagnosis |
| Oba et al. [ | 2001 | 70 | Male | Left lumbar muscle, left iliopsoas muscle | Brain, liver, lungs, adrenal glands | None | None | 71 days |
| Kondo et al. [ | 2002 | 64 | Female | Left gluteus maximus, left adductor magnus muscle | Abdominal wall | Total gastrectomy with splenectomy | Tumor excision of left gluteal mass, chemotherapy | 13 months |
| Tuoheti et al. [ | 2004 | 48 | Male | Gluteal muscle | Not available | Excision | Wide excision | 6 months |
| Tuoheti et al. [ | 2004 | 89 | Male | Shoulder muscle | Not available | Excision | Radiation therapy | 10 months (alive) |
| Bese et al. [ | 2006 | 60 | Male | Paravertebral muscle | Perigastric and lumboaortic lymph nodes | Gastrectomy, chemoradiotherapy | Palliative chemoradiotherapy | Not available |
| Souayah et al. [ | 2008 | 49 | Male | Right lateral rectus muscle | Not Available | Radiotherapy | Radiotherapy | 10 weeks |
| Tougeron et al. [ | 2009 | 71 | Male | Deltoid muscle | None | Partial gastrectomy, chemoradiotherapy | Chemoradiotherapy | 13 months (alive) |
| Satonaka et al. [ | 2010 | 51 | Male | Right thigh | Lungs, brain, skin | Chemotherapy, radiotherapy | Chemotherapy, radiotherapy | 7 months |
| Sakuma et al. [ | 2011 | 64 | Female | Gluteal muscle | Retroperitoneal and peritoneal dissemination | Total gastrectomy | Chemotherapy | 18 months (alive) |
| Gogou et al. [ | 2012 | Not available | Male | Femoral muscle | No liver or lung metastases | Gastrectomy | Wide excision, radiotherapy | 30 months |
| Pergolini et al. [ | 2014 | 67 | Male | Adductor muscle | Widespread metastatic disease | Chemotherapy | Chemotherapy | 74 days |
| Lourenço et al. [ | 2014 | 68 | Male | Right thigh | None | Chemotherapy | Chemotherapy | Not available |
| Koga et al. [ | 2015 | 71 | Male | Latissimus dorsi, transverse abdominal, iliopsoas, femoral muscle | None | Preoperative chemotherapy, total gastrectomy | Chemotherapy | 18 days |
| Temido et al. [ | 2017 | 42 | Male | Extraocular muscle | Bone metastasis, mediastinal and abdominal ganglia | None | None | Shortly after diagnosis |
| Kamitani et al. [ | 2018 | 47 | Male | Left latissimus dorsi, paraspinal muscle, quadriceps | None | Distal gastrectomy, chemotherapy | Chemotherapy | 7 months |
| Aguirre et al. [ | 2019 | 57 | Female | Obturator internus, vastus lateralis, quadratus lumborum, psoas, gluteus maximus, piriformis muscle | Peritoneal carcinomatosis | Total gastrectomy, chemoradiation | Palliative radiotherapy | 3 months after discharge |
| Goto et al. [ | 2019 | 54 | Female | Left medial rectus muscle | Ovary and mesentery, thoracic bone marrow | Chemotherapy | Radiotherapy | 3 months |
| Korehisa et al. [ | 2021 | 64 | Male | Right gluteal muscle | Peritoneal dissemination | Distal gastrectomy, chemotherapy | Chemotherapy, radiotherapy | 2 months |
| Garcia et al. [ | 2021 | 44 | Female | Left deltoid muscle | None | Gastrectomy, chemotherapy | Excision | Not available |
| Daneti et al. [ | 2021 | 42 | Male | Multiple muscle metastases | Not available | Antropyloric stenting | Supportive care | 6 weeks |
| Sellami et al. [ | 2022 | 53 | Male | Right superior oblique muscle | Lungs | Chemotherapy | Chemotherapy | Died before completing his courses of chemotherapy |
| Roohe et al. [ | 2022 | 67 | Male | Left rectus lateralis muscle | Leptomeningeal metastasis | None | None | 2 months |
| Our case | 2024 | 45 | Female | Multiple muscle metastases | Peritoneal dissemination | Chemotherapy | Chemotherapy | 17 months (alive) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Metastasis and carcinoma case studies · Gastric Cancer Management and Outcomes
Introduction
Gastric cancer ranks as the fifth most prevalent malignancy and stands as the third most frequent cause of cancer-associated mortality globally [1]. The vast majority of malignant gastric tumors are adenocarcinomas [2]. According to the Lauren classification system, gastric adenocarcinomas can be histologically classified into two subgroups: diffuse type and intestinal type. The intestinal type of gastric carcinomas is usually linked to lymphatic or hematogenous metastases. Therefore, lesions in distant areas of the body are common in this type. It primarily occurs in older male patients and has a better prognosis. On the contrary, the diffuse type usually affects younger female patients and has a worse prognosis compared to the intestinal type. Peritoneal dissemination is usual in diffuse gastric carcinomas [3]. The prognosis of patients diagnosed with gastric carcinoma hinges upon the cancer stage, ascertained by the extent of tumor invasion, lymph node involvement, and the presence or absence of metastases [4]. Gastric cancer can disseminate through multiple pathways, encompassing lymphatic and hematogenous spread, subperitoneal dissemination, direct invasion into neighboring organs, and peritoneal cavity dissemination [5]. Gastric cancer can be categorized into four stages (I-IV) according to the Japanese Classification of gastric carcinoma. Having a metastasis to areas of the body other than the regional lymph nodes or adjacent anatomical structures is classified as a distant metastasis. In such cases, the patient is considered to have stage IV gastric carcinoma [6]. The literature has scarcely reported cases of abdominal wall invasion from gastric cancer, as well as muscle metastases arising from gastric malignancy. We present a case report of a female patient exhibiting diffuse abdominal wall swelling, diagnosed as abdominal wall invasion and concurrent multiple muscle metastases originating from gastric cancer.
Case presentation
On September 20, 2022, a 45-year-old female was admitted to the surgical department of our hospital due to a painful left abdominal wall mass. The patient reported experiencing fatigue and weight loss over the previous five months. Vitals and laboratory test results were generally within normal ranges, except for a low hematocrit level (32.0%), which the patient had disclosed during admission. A thorough clinical examination revealed a sizable and tender mass in the left upper and lower quadrants of the abdomen.
A contrast-enhanced computed tomography (CT) scan of the abdomen revealed extensive swelling of multiple skeletal muscles of the back and the anterolateral abdominal wall on the left side, as well as thickening of the gastric wall and the serosa layer of the gastrointestinal tract, prompting suspicion of gastric malignancy (Figure 1a). A biopsy of the affected abdominal wall muscles and an upper gastrointestinal tract endoscopy and colonoscopy were performed. The gastroscopy unveiled a 25-mm diameter ulcer located at the body of the stomach, and a subsequent biopsy of the ulcer confirmed the existence of a poorly differentiated diffuse-type adenocarcinoma. The colonoscopy revealed no abnormalities. The muscle biopsy results demonstrated diffuse infiltration of the skeletal muscles by the recently diagnosed gastric adenocarcinoma. Additionally, the chest CT scan exhibited no pathological findings.
Contrast-enhanced abdominal computed tomography(a) The initially performed CT demonstrates diffuse thickening of the gastric wall, epiploic seeding, multisegmental serosal thickening of the gastrointestinal tract, as well as dramatic diffuse thickening of the muscles of the back (yellow arrow) and the anterolateral abdominal wall on the left side (white arrow). (b) The CT performed 16 months after the initial diagnosis, after the completion of chemotherapy, demonstrates a substantial improvement concerning primarily the abdominal wall invasion.
The patient was referred to the Oncology Department to commence treatment. Based on the CT findings, the biopsy results from the abdominal wall muscles, and the findings of the upper endoscopy, our patient received a diagnosis of stage IV gastric adenocarcinoma, according to the Japanese Classification of Gastric Carcinoma [6]. At this point, the patient's treatment plan was optimized through the selection of systemic chemotherapy as the most suitable course of action. Subsequent to chemotherapy, CT scans of the chest and abdomen demonstrated a reduction in the size of the skeletal muscle metastases and the lesions within the peritoneal cavity (Figure 1b). Seventeen months following the initial diagnosis, the patient has regained her normal weight, has returned to her previous job and is currently under surveillance and careful monitoring from her physicians.
Discussion
Abdominal wall masses can manifest as the chief concern in patients seeking care at the emergency department or can be serendipitously identified through incidental imaging procedures. Research indicates that the predominant sources of abdominal wall masses include desmoid tumors, sarcomas, metastatic growths, lipomas, and endometriomas, with a substantial portion (approximately 58%) exhibiting benign characteristics [7]. When dealing with extensive abdominal wall conditions, such as the one presented in our scenario, the diagnostic strategy necessitates a comprehensive understanding of the patient's medical history [8]. In their investigation, Li et al. delineated a diagnostic methodology for discerning abdominal wall masses by categorizing them into three distinct classes: primary neoplasms, secondary malignancies, and neoplasm-mimicking lesions [9]. Primary neoplasms encompass entities like lipomas, liposarcomas, fibroblastic and vascular tumors, nerve sheath tumors, and undifferentiated sarcomas. Secondary neoplasms relate to instances of metastases and lymphomas. Abdominal wall infiltration by secondary growths occurs through mechanisms of metastasis, direct encroachment, and implantation from remote locations. Additionally, tumor-like formations include hernias, endometriosis, hematoma, and abscesses. According to the guidelines established by the American College of Radiology (ACR) Appropriateness Criteria for evaluating abdominal wall masses, diagnostic modalities such as ultrasound, contrast-enhanced CT, and MRI are deemed suitable techniques for visualization [10].
The invasion of the abdominal wall by gastric cancer in patients is an exceedingly uncommon occurrence. As far as current understanding extends, only a handful of instances have been documented in the available literature (Table 1). The prevailing trend in the reported cases involves the implementation of an aggressive surgical strategy, characterized by comprehensive gastrectomy and simultaneous en bloc removal of the infiltrated adjacent organs.
Table 1: Reported cases of abdominal wall invasion in patients with gastric cancer [11-17]
<table><tbody><tr><td rowspan="1" colspan="1">Authors</td><td rowspan="1" colspan="1">Year</td><td rowspan="1" colspan="1">Age</td><td rowspan="1" colspan="1">Sex</td><td rowspan="1" colspan="1">Other sites of metastasis</td><td rowspan="1" colspan="1">Treatment</td><td rowspan="1" colspan="1">Survival</td></tr><tr><td rowspan="1" colspan="1">Chu et al. [<xref>11</xref>]</td><td rowspan="1" colspan="1">1995</td><td rowspan="1" colspan="1"> 61</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Many adjacent organs</td><td rowspan="1" colspan="1">Gastrectomy, resection of affected organs</td><td rowspan="1" colspan="1">6 months (alive)</td></tr><tr><td rowspan="1" colspan="1">Katsumoto et al. [<xref>12</xref>]</td><td rowspan="1" colspan="1">2007</td><td rowspan="1" colspan="1"> 68</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Abdominal tumors</td><td rowspan="1" colspan="1">Distal gastrectomy, systemic chemotherapy</td><td rowspan="1" colspan="1">Not Available</td></tr><tr><td rowspan="1" colspan="1">Carlomagno et al. [<xref>13</xref>]</td><td rowspan="1" colspan="1">2015</td><td rowspan="1" colspan="1"> 81</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Transverse mesocolon</td><td rowspan="1" colspan="1">Gastrectomy, transverse colon and abdominal wall resection</td><td rowspan="1" colspan="1">Died 20 days post-operation</td></tr><tr><td rowspan="1" colspan="1">Cho et al. [<xref>14</xref>]</td><td rowspan="1" colspan="1">2015</td><td rowspan="1" colspan="1"> 71</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Gastrectomy, partial resection of abdominal wall</td><td rowspan="1" colspan="1">Died 3 months post-operation</td></tr><tr><td rowspan="1" colspan="1">Misumi et al. [<xref>15</xref>]</td><td rowspan="1" colspan="1">2019</td><td rowspan="1" colspan="1"> 76</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Distal gastrectomy, repeated extractions of abdominal wall masses</td><td rowspan="1" colspan="1">1 year and 6 months post operation (alive)</td></tr><tr><td rowspan="1" colspan="1">Nakamura et al. [<xref>16</xref>]</td><td rowspan="1" colspan="1">2021</td><td rowspan="1" colspan="1"> 70</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Transverse colon</td><td rowspan="1" colspan="1">Gastrectomy, transverse colon and abdominal wall resection, chemotherapy</td><td rowspan="1" colspan="1">6 months post operation (alive)</td></tr><tr><td rowspan="1" colspan="1">Fukui et al. [<xref>17</xref>]</td><td rowspan="1" colspan="1">2021</td><td rowspan="1" colspan="1"> 75</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Port site metastasis, left gluteal subcutaneous metastasis</td><td rowspan="1" colspan="1">Laparoscopic total gastrectomy, mass resection, radiotherapy </td><td rowspan="1" colspan="1">78 months post gastrectomy (alive)</td></tr><tr><td rowspan="1" colspan="1">This study</td><td rowspan="1" colspan="1">2024</td><td rowspan="1" colspan="1"> 45</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Multiple muscle metastases, peritoneal dissemination </td><td rowspan="1" colspan="1">Systemic chemotherapy</td><td rowspan="1" colspan="1">17 months (alive)</td></tr></tbody></table>McNeer et al. emerged as early contributors to the notion that individuals afflicted with locally advanced gastric cancer necessitate interventions beyond gastrectomy to optimize their life expectancy [18]. A study encompassing 281 patients diagnosed with gastric cancer coupled with invasions into adjacent anatomical structures unveiled that survival rates could be extended by excising not only the stomach but also the invaded organs. This survival benefit was contingent upon the absence of peritoneal cavity dissemination or extensive nodal engagement [19]. In contrast to these typical scenarios, our presented case diverges due to the infiltration of numerous muscles by the primary gastric carcinoma. While the norm features anterior abdominal wall involvement, primarily concerning the rectus abdominis muscle, our instance deviates as it encompasses not only abdominal wall muscles but also back muscles within the patient's widespread swelling. This unique presentation led to the diagnosis of multiple muscle metastases.
The occurrence of skeletal muscle metastasis has been ascertained to be approximately 0.03% to 0.16% [20]. It remains challenging to elucidate the rarity of metastasis to muscle, especially considering that skeletal muscles constitute more than half of the body's total mass, as noted by Oba et al. [21]. The authors proposed several factors contributing to this rarity, including the continuous blood circulation, the potential clearance of malignant cells through muscle contractions, and the impediments posed to tumor cell proliferation by factors such as lactic acid, proteases, and muscle pH.
Haygood et al. conducted a comprehensive review encompassing 264 cases of patients afflicted with skeletal muscle metastases [22]. Their analysis divulged that the majority of these cases originated in the lungs, with only one instance stemming from the stomach as the primary source. In a separate study, Herring et al. chronicled 15 patients who exhibited skeletal muscle metastases over a 16-year period, alongside an examination of 52 additional cases documented in the literature [23]. Within their cohort, a solitary patient displayed a gastrointestinal tract primary tumor, while once again, 53% of cases were traced back to pulmonary origins. Upon scrutinizing the literature, Herring et al. discovered that 23% of all cases featuring skeletal muscle metastases had their origins in the gastrointestinal tract, and notably, only five out of the 52 cases featured multiple muscle metastatic lesions.
Despite CT scans often being the initial means of identifying muscle metastases, MRI stands out as a more adept modality for detecting these anomalies. Upon recognizing a mass within skeletal muscle, biopsy becomes imperative for accurate diagnosis [23].
Since 2000, a total of 22 instances involving muscle metastases originating from gastric cancer have been documented (Table 2). It remains plausible for muscle metastases to serve as the primary clinical indication of an occult primary lesion, either with or without concurrent metastases elsewhere. In individuals with a known malignancy history, the emergence of a painful mass should prompt clinicians' suspicion, with the patient's medical background pivotal in the final diagnosis determination [20].
Table 2: Reported cases of gastric cancer patients with concurrent muscle metastases [20-21, 24-42]
<table><tbody><tr><td rowspan="1" colspan="1">Authors</td><td rowspan="1" colspan="1">Year</td><td rowspan="1" colspan="1">Age</td><td rowspan="1" colspan="1">Sex</td><td rowspan="1" colspan="1">Sites of muscle metastases</td><td rowspan="1" colspan="1">Other sites of metastases</td><td rowspan="1" colspan="1">Treatment for gastric cancer</td><td rowspan="1" colspan="1">Treatment for muscle metastases</td><td rowspan="1" colspan="1">Survival after the muscle metastasis diagnosis</td></tr><tr><td rowspan="1" colspan="1">Oba et al. [<xref>21</xref>]</td><td rowspan="1" colspan="1">2001</td><td rowspan="1" colspan="1">70</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Left lumbar muscle, left iliopsoas muscle</td><td rowspan="1" colspan="1">Brain, liver, lungs, adrenal glands</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">71 days</td></tr><tr><td rowspan="1" colspan="1">Kondo et al. [<xref>24</xref>]</td><td rowspan="1" colspan="1">2002</td><td rowspan="1" colspan="1">64</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Left gluteus maximus, left adductor magnus muscle</td><td rowspan="1" colspan="1">Abdominal wall</td><td rowspan="1" colspan="1">Total gastrectomy with splenectomy</td><td rowspan="1" colspan="1">Tumor excision of left gluteal mass, chemotherapy </td><td rowspan="1" colspan="1">13 months</td></tr><tr><td rowspan="1" colspan="1">Tuoheti et al. [<xref>20</xref>]</td><td rowspan="1" colspan="1">2004</td><td rowspan="1" colspan="1">48</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Gluteal muscle</td><td rowspan="1" colspan="1">Not available</td><td rowspan="1" colspan="1">Excision</td><td rowspan="1" colspan="1">Wide excision</td><td rowspan="1" colspan="1">6 months</td></tr><tr><td rowspan="1" colspan="1">Tuoheti et al. [<xref>20</xref>]</td><td rowspan="1" colspan="1">2004</td><td rowspan="1" colspan="1">89</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Shoulder muscle</td><td rowspan="1" colspan="1">Not available</td><td rowspan="1" colspan="1">Excision</td><td rowspan="1" colspan="1">Radiation therapy</td><td rowspan="1" colspan="1">10 months (alive)</td></tr><tr><td rowspan="1" colspan="1">Bese et al. [<xref>25</xref>]</td><td rowspan="1" colspan="1">2006</td><td rowspan="1" colspan="1">60</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Paravertebral muscle</td><td rowspan="1" colspan="1">Perigastric and lumboaortic lymph nodes</td><td rowspan="1" colspan="1">Gastrectomy, chemoradiotherapy</td><td rowspan="1" colspan="1">Palliative chemoradiotherapy</td><td rowspan="1" colspan="1">Not available</td></tr><tr><td rowspan="1" colspan="1">Souayah et al. [<xref>26</xref>]</td><td rowspan="1" colspan="1">2008</td><td rowspan="1" colspan="1">49</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Right lateral rectus muscle</td><td rowspan="1" colspan="1">Not Available</td><td rowspan="1" colspan="1">Radiotherapy</td><td rowspan="1" colspan="1">Radiotherapy</td><td rowspan="1" colspan="1">10 weeks</td></tr><tr><td rowspan="1" colspan="1">Tougeron et al. [<xref>27</xref>]</td><td rowspan="1" colspan="1">2009</td><td rowspan="1" colspan="1">71</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Deltoid muscle</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Partial gastrectomy, chemoradiotherapy</td><td rowspan="1" colspan="1">Chemoradiotherapy</td><td rowspan="1" colspan="1">13 months (alive)</td></tr><tr><td rowspan="1" colspan="1">Satonaka et al. [<xref>28</xref>]</td><td rowspan="1" colspan="1">2010</td><td rowspan="1" colspan="1">51</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Right thigh</td><td rowspan="1" colspan="1">Lungs, brain, skin</td><td rowspan="1" colspan="1">Chemotherapy, radiotherapy</td><td rowspan="1" colspan="1">Chemotherapy, radiotherapy</td><td rowspan="1" colspan="1">7 months</td></tr><tr><td rowspan="1" colspan="1">Sakuma et al. [<xref>29</xref>]</td><td rowspan="1" colspan="1">2011</td><td rowspan="1" colspan="1">64</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Gluteal muscle</td><td rowspan="1" colspan="1">Retroperitoneal and peritoneal dissemination</td><td rowspan="1" colspan="1">Total gastrectomy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">18 months (alive)</td></tr><tr><td rowspan="1" colspan="1">Gogou et al. [<xref>30</xref>]</td><td rowspan="1" colspan="1">2012</td><td rowspan="1" colspan="1">Not available</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Femoral muscle</td><td rowspan="1" colspan="1">No liver or lung metastases</td><td rowspan="1" colspan="1">Gastrectomy</td><td rowspan="1" colspan="1">Wide excision, radiotherapy</td><td rowspan="1" colspan="1">30 months</td></tr><tr><td rowspan="1" colspan="1">Pergolini et al. [<xref>31</xref>]</td><td rowspan="1" colspan="1">2014</td><td rowspan="1" colspan="1">67</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Adductor muscle</td><td rowspan="1" colspan="1">Widespread metastatic disease</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">74 days</td></tr><tr><td rowspan="1" colspan="1">Lourenço et al. [<xref>32</xref>]</td><td rowspan="1" colspan="1">2014</td><td rowspan="1" colspan="1">68</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Right thigh</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Not available</td></tr><tr><td rowspan="1" colspan="1">Koga et al. [<xref>33</xref>]</td><td rowspan="1" colspan="1">2015</td><td rowspan="1" colspan="1">71</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Latissimus dorsi, transverse abdominal, iliopsoas, femoral muscle</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Preoperative chemotherapy, total gastrectomy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">18 days</td></tr><tr><td rowspan="1" colspan="1">Temido et al. [<xref>34</xref>]</td><td rowspan="1" colspan="1">2017</td><td rowspan="1" colspan="1">42</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Extraocular muscle</td><td rowspan="1" colspan="1">Bone metastasis, mediastinal and abdominal ganglia</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Shortly after diagnosis</td></tr><tr><td rowspan="1" colspan="1">Kamitani et al. [<xref>35</xref>]</td><td rowspan="1" colspan="1">2018</td><td rowspan="1" colspan="1">47</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Left latissimus dorsi, paraspinal muscle, quadriceps</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Distal gastrectomy, chemotherapy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">7 months</td></tr><tr><td rowspan="1" colspan="1">Aguirre et al. [<xref>36</xref>]</td><td rowspan="1" colspan="1">2019</td><td rowspan="1" colspan="1">57</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Obturator internus, vastus lateralis, quadratus lumborum, psoas, gluteus maximus, piriformis muscle</td><td rowspan="1" colspan="1">Peritoneal carcinomatosis</td><td rowspan="1" colspan="1">Total gastrectomy, chemoradiation</td><td rowspan="1" colspan="1">Palliative radiotherapy</td><td rowspan="1" colspan="1">3 months after discharge</td></tr><tr><td rowspan="1" colspan="1">Goto et al. [<xref>37</xref>]</td><td rowspan="1" colspan="1">2019</td><td rowspan="1" colspan="1">54</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Left medial rectus muscle</td><td rowspan="1" colspan="1">Ovary and mesentery, thoracic bone marrow</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Radiotherapy</td><td rowspan="1" colspan="1">3 months</td></tr><tr><td rowspan="1" colspan="1">Korehisa et al. [<xref>38</xref>]</td><td rowspan="1" colspan="1">2021</td><td rowspan="1" colspan="1">64</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Right gluteal muscle</td><td rowspan="1" colspan="1">Peritoneal dissemination</td><td rowspan="1" colspan="1">Distal gastrectomy, chemotherapy</td><td rowspan="1" colspan="1">Chemotherapy, radiotherapy</td><td rowspan="1" colspan="1">2 months</td></tr><tr><td rowspan="1" colspan="1">Garcia et al. [<xref>39</xref>]</td><td rowspan="1" colspan="1">2021</td><td rowspan="1" colspan="1">44</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Left deltoid muscle</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">Gastrectomy, chemotherapy</td><td rowspan="1" colspan="1">Excision</td><td rowspan="1" colspan="1">Not available</td></tr><tr><td rowspan="1" colspan="1">Daneti et al. [<xref>40</xref>]</td><td rowspan="1" colspan="1">2021</td><td rowspan="1" colspan="1">42</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Multiple muscle metastases</td><td rowspan="1" colspan="1">Not available</td><td rowspan="1" colspan="1">Antropyloric stenting</td><td rowspan="1" colspan="1">Supportive care</td><td rowspan="1" colspan="1">6 weeks</td></tr><tr><td rowspan="1" colspan="1">Sellami et al. [<xref>41</xref>]</td><td rowspan="1" colspan="1">2022</td><td rowspan="1" colspan="1">53</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Right superior oblique muscle</td><td rowspan="1" colspan="1">Lungs</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Died before completing his courses of chemotherapy</td></tr><tr><td rowspan="1" colspan="1">Roohe et al. [<xref>42</xref>]</td><td rowspan="1" colspan="1">2022</td><td rowspan="1" colspan="1">67</td><td rowspan="1" colspan="1">Male</td><td rowspan="1" colspan="1">Left rectus lateralis muscle</td><td rowspan="1" colspan="1">Leptomeningeal metastasis</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">None</td><td rowspan="1" colspan="1">2 months</td></tr><tr><td rowspan="1" colspan="1">Our case</td><td rowspan="1" colspan="1">2024</td><td rowspan="1" colspan="1">45</td><td rowspan="1" colspan="1">Female</td><td rowspan="1" colspan="1">Multiple muscle metastases</td><td rowspan="1" colspan="1">Peritoneal dissemination </td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">Chemotherapy</td><td rowspan="1" colspan="1">17 months (alive)</td></tr></tbody></table>Potential therapeutic avenues encompass radiotherapy, chemotherapy, or surgical excision, contingent on the clinical attributes of the muscle metastasis. For patients bearing exclusively a painful muscle metastasis without additional metastatic foci, judicious surgical removal might mitigate pain and extend life expectancy [23].
Our patient received a diagnosis of stage IV gastric cancer owing to the substantial invasion of skeletal muscles and the peritoneal dissemination of cancer cells. For individuals grappling with advanced gastric cancer or those who undergo non-curative R2 resection, systemic chemotherapy stands as the preferred therapeutic approach [43]. The anticipated survival period for patients confronting this stage of gastric cancer approximates 15 months [44]. Given the advanced stage in our case, radiotherapy and surgical excision were ruled out as feasible interventions. Our patient successfully underwent multiple rounds of chemotherapy, and as of 17 months post-diagnosis, she is presently alive and under careful monitoring.
Conclusions
Abdominal wall invasion and muscle metastases from gastric cancer are rare and difficult to diagnose. Any muscle mass should raise suspicion to clinicians and lead to a biopsy in order to establish a diagnosis. Muscle metastases may be the first presentation of an unknown malignancy, as in our case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012 Int J Cancer Ferlay J Soerjomataram I Dikshit R 086136201510.1002/ijc.2921025220842 · doi ↗ · pubmed ↗
- 2Current role of CT in imaging of the stomach Radiographics Horton KM Fishman EK 75872320031253364310.1148/rg.231025071 · doi ↗ · pubmed ↗
- 3Lauren classification and individualized chemotherapy in gastric cancer Oncol Lett Ma J Shen H Kapesa L Zeng S 295929641120162712304610.3892/ol.2016.4337 PMC 4840723 · doi ↗ · pubmed ↗
- 4State-of-the-art preoperative staging of gastric cancer by MDCT and magnetic resonance imaging World J Gastroenterol Choi JI Joo I Lee JM 454645572020142478260710.3748/wjg.v 20.i 16.4546 PMC 4000491 · doi ↗ · pubmed ↗
- 5Ligaments and lymphatic pathways in gastric adenocarcinoma Radiographics Young JJ Pahwa A Patel M 6686893920193095143810.1148/rg.2019180113 · doi ↗ · pubmed ↗
- 6Japanese classification of gastric carcinoma: 3rd English edition Gastric Cancer Japanese Gastric Cancer Association 1011121420112157374310.1007/s 10120-011-0041-5 · doi ↗ · pubmed ↗
- 7Soft-tissue masses in the abdominal wall Clin Radiol Bashir U Moskovic E Strauss D Hayes A Thway K Pope R Messiou C 03169201410.1016/j.crad.2014.06.00625064764 · doi ↗ · pubmed ↗
- 8Imaging of abdominal wall masses, masslike lesions, and diffuse processes Radiographics Ballard DH Mazaheri P Oppenheimer DC 6847064020203233008510.1148/rg.2020190170 PMC 7263290 · doi ↗ · pubmed ↗