Analysis of health risk factors for older adults living alone in China and establishment and evaluation of a nomogram prediction model
Kexin Chen, Jiangwei Qiu, Wenlong Wang, Qi Hu, Hui Qiao

TL;DR
This study examines health risk factors for older adults living alone in China and builds a model to predict their health outcomes.
Contribution
The paper introduces a nomogram prediction model for health risks among older adults living alone in China.
Findings
Gender, income, Mandarin listening, and medical insurance affect self-rated health of older adults living alone.
Age and income influence physiological health, while income and Internet use impact mental health.
The nomogram model showed moderate predictive ability with a C-Statistic of 0.645.
Abstract
To understand the health status of older adults living alone in China and analyze the influencing factors, so as to provide reference for improving the health status of older adults living alone. Based on CGSS data from China General Social Survey (2017), the influencing factors of health status of older adults living alone were analyzed by unconditional Logistic regression, and the R software was used to develop a nomogram for predicting the risk of self-assessed unhealthy adverse outcomes. Gender, annual income, mandarin listening level and participation in medical insurance were the influencing factors of self-rated health of older adults living alone. Age and annual income are the influencing factors of physiological health. Annual income and Internet use were influential factors for mental health. C-Statistic of nomogram prediction model was 0.645. The calibration curve showed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
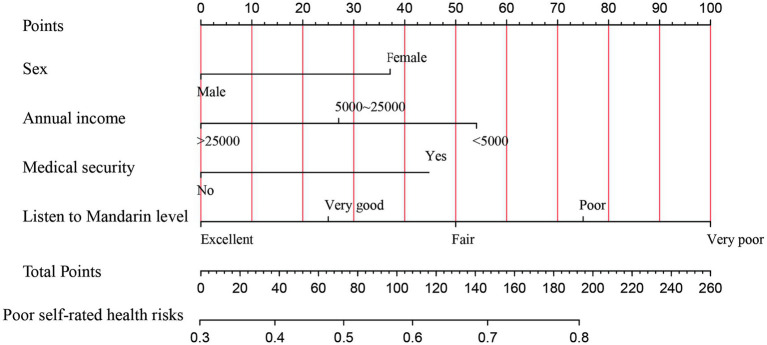 Figure 1
Figure 1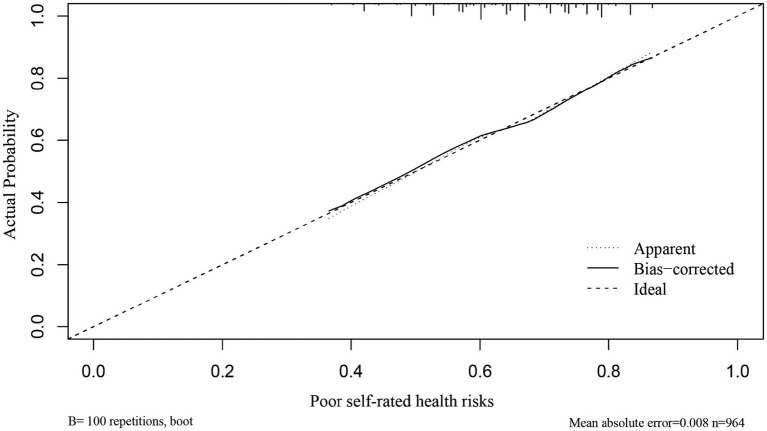 Figure 2
Figure 2| Variable | Definition |
|---|---|
| Self-rated health | Yes = 1; No = 0 |
| Physical health | Yes = 1; No = 0 |
| Mental health | Yes = 1; No = 0 |
| Age | Continuous variable |
| Sex | Male = 1; Female = 2 |
| Urban and rural | Rural residents = 1; urban resident = 2 |
| Education | Primary and below =1; Middle School to High School =2; University degree or above = 4 |
| Annual income (Yuan) | <5,000 = 1, 5,000 ~ 25,000 = 2, >25,000 = 3 |
| Participation in medical security | Yes = 1; No = 0 |
| Participation in pension insurance | Yes = 1; No = 0 |
| Internet usage | Never =1; Rarely =2; Sometimes =3; Often =4; Always =5 |
| Listening level of mandarin | Completely unintelligible =1; poor =2, average = 3; good =4; excellent =5 |
| Speaking level of mandarin | It is completely impossible to say =1; poor =2; average = 3; good =4; excellent =5 |
| Variable | Self-rated health | Physical health | Mental health | ||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
| 95% |
|
| 95%CI |
|
| 95% | |
| Age | −0.01 | 0.99 | 0.98 ~ 1.00 | −0.03 | 0.97** | 0.96 ~ 0.99 | 0.01 | 1.01 | 0.99 ~ 1.02 |
| Sex (ref = male) | 0.39 | 0.68* | 0.52 ~ 0.87 | −0.17 | 0.85 | 0.66 ~ 1.08 | −0.09 | 0.92 | 0.72 ~ 1.18 |
| Urban and rural (ref = urban resident) | 0.43 | 1.54* | 1.19 ~ 1.20 | −0.95 | 2.60** | 2.02 ~ 3.35 | −0.79 | 2.21** | 1.71 ~ 2.85 |
| Education | 0.40 | 1.49** | 1.21 ~ 1.84 | 0.62 | 1.85** | 1.50 ~ 2.30 | 0.46 | 1.58** | 1.28 ~ 1.96 |
| Annual income (Yuan) | 0.41 | 1.51** | 1.29 ~ 1.76 | 0.74 | 2.10** | 1.80 ~ 2.47 | 0.67 | 1.96** | 1.67 ~ 2.30 |
| Participation in medical security (ref = no) | −0.44 | 0.65* | 0.44 ~ 0.95 | −0.29 | 0.75 | 0.51 ~ 1.10 | −0.26 | 0.77 | 0.52 ~ 1.14 |
| Participation in pension insurance (ref = no) | 0.13 | 1.14 | 0.84 ~ 1.56 | 0.21 | 1.24 | 0.93 ~ 1.26 | 0.26 | 1.30 | 0.97 ~ 1.74 |
| Internet usage | 0.02 | 1.02 | 0.98 ~ 1.07 | 0.33 | 1.39** | 1.24 ~ 1.57 | 0.32 | 1.38** | 1.22 ~ 1.56 |
| Listening level of mandarin | 0.38 | 1.47** | 1.29 ~ 1.66 | 0.36 | 1.43** | 1.28 ~ 1.61 | 0.30 | 1.36** | 1.21 ~ 1.52 |
| Speaking level of mandarin | 0.26 | 1.30** | 1.18 ~ 1.44 | 0.32 | 1.37** | 1.24 ~ 1.52 | 0.28 | 1.32** | 1.19 ~ 1.46 |
| Variable | Self-rated health | Physical health | Mental health | ||||||
|---|---|---|---|---|---|---|---|---|---|
|
| OR | 95% |
| OR | 95%CI |
| OR | 95%CI | |
| Age | −0.03 | 0.97** | 0.96 ~ 0.99 | ||||||
| Sex (ref = male) | 0.41 | 1.51** | 1.14 ~ 1.20 | ||||||
| Urban and rural (ref = urban resident) | 0.13 | 1.14 | 0.76 ~ 1.71 | −0.34 | 0.71 | 0.49 ~ 1.05 | −0.18 | 0.83 | 0.57 ~ 1.22 |
| Education | 0.01 | 1.00 | 0.76 ~ 1.33 | −0.15 | 0.86 | 0.64 ~ 1.16 | −0.24 | 0.79 | 0.59 ~ 1.01 |
| Annual income (Yuan) | 0.35 | 1.42** | 1.13 ~ 1.78 | 0.60 | 1.82** | 1.47 ~ 2.27 | 0.56 | 1.76** | 1.42 ~ 2.18 |
| Participation in medical security (ref = no) | −0.52 | 0.60** | 0.39 ~ 0.91 | ||||||
| Participation in pension insurance (ref = no) | 0.10 | 1.10 | 0.96 ~ 1.27 | 0.20 | 1.23** | 1.06 ~ 1.42 | |||
| Internet usage | 0.29 | 1.33** | 1.12 ~ 1.59 | 0.14 | 1.16 | 0.97 ~ 1.37 | 0.14 | 1.14 | 0.97 ~ 1.35 |
| Listening level of mandarin | 0.02 | 1.02 | 0.86 ~ 1.20 | −0.05 | 0.95 | 0.80 ~ 1.12 | −0.05 | 0.95 | 0.81 ~ 1.12 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth disparities and outcomes · Intergenerational Family Dynamics and Caregiving · Cardiovascular Health and Risk Factors
Introduction
China, as a populous nation, is currently grappling with the profound challenges posed by its aging population. According to the Blue Book on Aging: China Aging Research Report 2022 released by the Chinese Gerontological Society, by the end of 2021, China’s population aged 60 and above reached 267 million, accounting for 18.9% of the total population (1). The fourth survey on the living conditions of urban and rural older adults in China reveals that the number of empty-nest older adults exceeds 100 million, with some major cities and rural areas having a proportion exceeding 70% (2). The transition to smaller family sizes and a preference for traditional care models contribute to a significant increase in the number of isolated older individuals lacking robust social support networks (3). In this context, China, in pursuit of the development goals for achieving Universal Health Coverage (UHC), has prioritized the enhancement of older adults health management (4). This demographic shift towards an aging society necessitates a comprehensive examination of the health and well-being of older adults individuals, particularly those who live alone (5). It is crucial to identify and mitigate health risks among older individuals living alone, providing them with appropriate medical services and support.
Older individuals living alone, separated from their children or other family members, confront numerous challenges, including inconveniences, difficulties, and safety hazards in home-based care (6, 7). A cohort study showed that living alone increases the risk of hypertension in older adults in China (7). Moreover, research has illuminated that living alone, compared to cohabiting with family, is significantly associated with higher levels of depression (8). Previous research has proposed encouraging older individuals living alone to engage in social activities as a means to improve sleep quality, alleviate anxiety, and address the loneliness associated with solitary living (9). Research has shown that older individuals living alone are more susceptible to environmental risks, such as falls, compared to those cohabiting with others (10). Devoid of robust social relationships and assistance, these isolated older adults are susceptible to malnutrition, accidents, self-neglect, untreated medical conditions, and other health threats (11–13).
Former research on the health status of solitary older adults in home-based care has centered largely on disparate regions (7), community care models (14) and support systems (15). While most of these studies addressed disease factors and nutritional status, they devoted less consideration to the connections between the health conditions of solitary seniors and elements like mandarin proficiency, digital literacy, health insurance coverage, and pension benefits, overlooking some critical information. Yet these factors may be key determinants impacting the welfare of this vulnerable group. Research has indicated that digital inclusion and cultural capital contribute to improving residents’ health conditions (16). Digital health literacy is beneficial for enabling older adults to access medical services, participate in social activities, and enhance their quality of life (17). Previous studies have proposed that health insurance and pension assistance can reduce catastrophic health expenditures among older adults (18).
While earlier studies have firmly established connections between physical and mental well-being and factors like income security, insurance coverage, and technical literacy in the general older adults populace, (19–21) targeted investigations into how these relationships distinctly manifest among solitary older adults have been lacking. This study aims to analyze key social determinants impacting the health outcomes of this cohort by delineating the physiological and psychological health challenges and empirical insights into self-rated health faced by solitary older adults. Meanwhile, transforming the intricate regression equations into visualized plots enhances the interoperability of the predictive models, aiding home care workers in appraising solitary seniors. By proactively comprehending the multifaceted risks solitary older adults confront, concrete steps can be taken to prevent deterioration in health and quality of life as this population swells.
Materials and methods
Data source and variable definition
The data is from the 2017 Chinese General Social Survey (CGSS) released by Renmin University of China. The 2017 survey data as the latest data for the project. CGSS is the first large-scale, comprehensive, continuous national social survey project in China. The survey samples were selected through multi-stage stratified sampling, covering 28 provinces, autonomous regions and municipalities in China. It is highly representative of the national population with high data quality (22). According to research needs, the target group in this study was set as “solitary older adults aged 60 and above.” After excluding missing values and extreme outliers, the effective total sample size included for analysis was 1,015. The database contains variables including gender, income, internet use, health status, participation in health insurance, and participation in pension insurance.
The dependent variable is the health status of solitary older adults. Based on the WHO’s definition of health from physical, mental and social perspectives as “a state of complete well-being,” the health conditions of solitary older adults were comprehensively examined from three aspects: self-rated health, physical health, and mental health (23). The questionnaire items “How do you rate your current physical health?,” “How often did your health issues affect your work or other regular activities in the past 4 weeks?,” and “How often did you feel depressed or despair in the past 4 weeks?” were used to measure self-rated health, physical health, and mental health of solitary older adults, respectively. The above three items were measured using a 5-point Likert scale. Self-rated health, physical health, and mental health were assigned as binary classification variables. Specifically, self-rated health (very healthy and relatively healthy were assigned 1, general, relatively unhealthy and very unhealthy were assigned 0); physical health and mental health (never and rarely were assigned 1, sometimes, often and always were assigned 0). The independent variables encompassed facets such as gender, age, educational attainment, insurance coverage, internet usage, and competency in mandarin reading and listening comprehension. Table 1 shows the variable assignment table.
Statistical analyses
Statistical analysis was performed using SPSS 20.0 and R software (version 4.1.1). Quantitative data were described, and count data were expressed as frequency or percentage. Logistic regression analysis was used to analyze influencing factors of the health status of solitary older adults, with a test level of α = 0.05. Based on the results of multivariate logistic regression analysis, a nomogram predicting the risk of poor self-rated health was constructed using the Nomogram function in the rms package of R software. Internal validation was performed using the Bootstrap method with 1,500 resampling, and the C-statistic was calculated and a calibration curve plotted to examine the calibration of the influencing factors model, that is, the consistency between the actual probability of occurrence and the predicted probability of outcomes.
Logistic regression is a widely used method in binary classification problems, and its output is probability, which can be directly interpreted as the likelihood of an event occurring. The probit model is also a viable option, but its output is a probability density function and requires more technical interpretation. In contrast, logistic regression is more intuitive and easy to understand. The tobit model is typically used to deal with truncated data, i.e., where there is a lower or upper bound on the dependent variable. In the health-related variables I studied, there was no such truncation problem. Therefore, logistic regression was used for statistical analysis.
Results
Descriptive statistics of the solitary older adults
This study included a total of 1,015 solitary older adults. The oldest was 102 years old and the youngest 60 years old, with an average age of (74.75 ± 8.79) years. There were 463 females (45.6%) and 552 males (54.4%). Regarding marital status, 251 (24.7%) were married and 764 (75.3%) were divorced/widowed/unmarried. In terms of education level, 601 (59.2%) had primary school education or below, 352 (34.7%) had middle school (secondary school) or high school education, and 62 (6.1%) had college degree or above. Regarding household registration status, 521 (51.3%) had rural hukou and 494 (48.7%) had non-rural hukou. For social security programs, 895 (88.2%) participated in basic urban health insurance, new rural cooperative medical care or free medical care (abbreviated as health insurance participation), 120 (11.8%) did not participate; 777 (76.6%) participated in urban or rural basic pension insurance (abbreviated as pension insurance participation), 238 (23.4%) did not participate. For self-rated health, 659 (64.9%) rated themselves as unhealthy and 356 (35.1%) as healthy. For physical health, 479 (47.2%) rated themselves as unhealthy and 536 (52.8%) as healthy. For mental health, 428 (42.2%) rated themselves as unhealthy and 587 (57.8%) as healthy.
Univariate logistic regression analysis of health status of solitary older adults
Table 2 reports with self-rated health, physical health, and mental health of solitary older adults as dependent variables, and gender, household registration status, education level, annual income, health insurance participation, pension insurance participation, internet use, mandarin listening comprehension level, and mandarin speaking level as independent variables logistic regression analysis was performed. The results showed that gender, household registration status, education level, annual income, health insurance participation, mandarin listening comprehension level, and mandarin speaking level may be influencing factors for self-rated health of solitary older adults. Age, household registration status, education level, annual income, internet use, mandarin listening comprehension level, and mandarin speaking level may be influencing factors for physical health of solitary older adults. Household registration status, education level, annual income, internet use, mandarin listening comprehension level, and mandarin speaking level may be influencing factors for mental health of solitary older adults (p < 0.05).
Multivariate logistic regression analysis of health status of solitary older adults
Table 3 reports with self-rated health, physical health, and mental health of solitary older adults as dependent variables, and statistically significant indicators from univariate logistic regression analysis as independent variables, multivariate logistic regression analysis was performed. The results showed that gender, annual income, mandarin listening comprehension level, and health insurance participation were independent influencing factors for self-rated health of solitary older adults. Age and annual income were independent influencing factors for physical health of solitary older adults. Annual income and internet use were independent influencing factors for mental health of solitary older adults (p < 0.05).
Nomogram model building for risk of self-rated unhealthy in solitary older adults
Based on the results of multivariate logistic regression analysis, a nomogram model for the risk of self-rated unhealthy was constructed using R software. The nomogram results show that each factor’s value corresponds to the “points” in the first row, and the total points are calculated by adding up the points for each factor. The total points then correspond to the “Risk of Self-Rated Unhealthy” in the last row. If a solitary older adult is female, has an annual income less than 5,000 yuan or between 5,000–25,000 yuan, is uninsured, and has poor mandarin listening comprehension, the corresponding points increase. As the total score from adding up the points for each factor increases, the risk of that solitary older adult self-rating as unhealthy also increases (see Figure 1).
Nomogram model for the risk of self-rated unhealthy in solitary older adults. The different categories of each variable correspond to points on the nomogram axis. The score (points) for each variable can be obtained by drawing a vertical line upwards from the point. The total score (total points) is calculated by adding up the scores for each variable. The total score corresponds to a point on the risk axis for poor outcome, which represents the risk of self-rated unhealthy for the solitary older adult.
Validation of the nomogram model for self-rated unhealthy risk in solitary older adults
The C-index and calibration curves were used to evaluate the nomogram model. A C-index value closer to 1 indicates stronger predictive ability of the model. Internal validation via bootstrapping with 1,500 resamples was performed for this nomogram model (C-index = 0.645). The goodness of fit test gave χ^2^ = 58.09, p < 0.001, indicating that the established nomogram model has good accuracy, discrimination, and risk prediction capability (see Figure 2).
Calibration curve for the nomogram model predicting the risk of self-rated unhealthy in solitary older adults. The diagonal line represents the ideal curve, indicating agreement between actual and predicted values. The dotted line represents the original curve, and the solid line represents the calibrated curve. The closer to the ideal curve, the better the model’s predictive ability.
Discussion
The results of this study show that solitary older adults have poor health conditions. Among the 1,015 solitary older adults, 64.9% (659 people) rated their current physical health as unhealthy, while 35.1% (356 people) self-rated as healthy. For physical health, 47.2% of solitary older adults (479 people) self-rated as unhealthy and 52.8% (536 people) as physically healthy. For mental health, 42.2% of solitary older adults (428 people) self-rated as mentally unhealthy and 57.8% (587 people) as mentally healthy.
Self-rated health reflects individuals’ perceptions of their own health status (24). The results of this study show that gender, annual income, mandarin comprehension level, and participation in basic urban/rural health insurance programs are factors influencing self-rated health of solitary older adults. Females had poorer self-rated health compared to males. Higher income is a protective factor for self-rated health in solitary older adults, likely because older adults with higher income have more freedom in spending on healthy aging and medical care, which facilitates adhering to healthy behavioral measures (25, 26). Solitary older adults with better mandarin comprehension had higher self-rated health, possibly due to the increasing incidence of age-related hearing impairment over the years (27). Meanwhile, the popularity of mandarin is relatively low among older adults population, and speech recognition ability also impacts cognitive function in older adults (28). The older adults living alone who were covered by medical insurance were more likely to have better self-rated health, highlighting the importance of health insurance in UHC (29, 30).
By translating the results of multivariate regression analysis into a nomogram model, we present an intuitive individualized risk assessment approach, aiding in the more precise identification of vulnerable groups that require focused attention in the context of UHC. For instance, the nomogram can be used to promptly identify solitary older adults with higher risk of self-rated unhealthy. If a female older adult has an annual income of 5,000–25,000 yuan, participates in health insurance, and has poor mandarin comprehension, her points for each variable would be 37, 27, 45, and 75, respectively, with a total score of 184. This corresponds to 0.79 on the nomogram, indicating a 79% risk of self-rated unhealthy. For solitary older adults at higher specific risks, community health workers can employ information technology to deliver targeted interventions, thereby promoting healthy aging (31).
The physical health of solitary older adults, considered as a pivotal component in the measurement of multidimensional health, serves as a prominent predictor of overall health and mortality risk (32). Previous studies show that physical health is influenced by demographic and social characteristics, lifestyle, physical health functions, social health, and economic status (33). This study indicates advanced age and low income are independent factors influencing physical health of solitary older adults, with worse physical health at older ages. Income level also determines physical health, with lower-income solitary older adults having poorer physical health. This may be attributable to the irreversible decline in bodily structure and function that accompanies the march of senescence. Household economic status impacts the proportion of medical expenses in total consumption expenditures. Insufficient income cannot ensure basic medical security (30). Coupled with higher rates of chronic diseases in solitary older adults, lack of medical support greatly reduces their physical health (34).
As solitary living becomes more prevalent among older adults in China, the emotional changes and coping abilities of older adults facing long-term isolation warrant close attention. The results of this study reveal concerning mental health conditions among solitary older adults. Their psychological well-being is associated with increased income and internet use. This may be because older adults with higher economic status can fulfill basic needs for food, shelter, and clothing, then pursue higher-level needs of healthy social and recreational activities to safeguard mental health, effectively alleviating feelings of helplessness and loneliness from loss of a spouse or children leaving home, and elevating positive emotions (7, 34). Additionally, greater income implies solitary older adults can access and utilize more medical resources, reducing mental health risks. Internet use also clearly benefits the psychological well-being of solitary older adults, aligning with findings by Zhao et al. (35). The internet provides solitary older adults platforms for communication and learning, fulfilling the need for continued socialization (20). It helps to adapt to the changes in roles after retirement, increase social activities and intra-family decision-making, and reduce psychological discomfort in older adults (36, 37).
Within the framework of UHC, we advocate for greater attention to older people living alone by providing more pension assistance and health support. Family doctors and community nurses should be encouraged to adopt informational means to deliver home-based older adults care health services, penetrate into solitary older adults, guide older adults toward proactive aging approaches, improve their health service utilization, and provide government assistance and community public health services to economically disadvantaged solitary older adults. Confronting healthy aging, medical insurance functions should be fully exercised to implement policy publicity, promoting awareness of medical insurance compensation policies among solitary older adults. Meanwhile, relevant departments could jointly carry out promotion activities on mandarin proficiency and smartphone use to enhance solitary older adults’ mandarin comprehension and health knowledge exchange abilities. This can lower barriers and fears toward medical and health information platforms, increase adoption of “Internet Plus” healthcare among solitary older adults, strengthen interpersonal communication and health knowledge learning capabilities. At the same time, easy-to-understand online health lectures could be organized, and remote chronic disease management, physical examinations, psychological counseling and other older adults care health services provided, to facilitate healthy home-based aging among solitary older adults.
While our study benefits from a nationwide data set, it is crucial to acknowledge certain limitations. This research relies on cross-sectional data, and although it identifies health risk factors among solitary older individuals, it does not delve into the complex relationships between these factors. Future research endeavors may consider adopting a longitudinal study design to comprehensively understand the evolution of health conditions among solitary older individuals over time and to identify enduring influencing factors. This approach can contribute to the development of more effective intervention measures and policies.
Conclusion
We utilized data from the China General Social Survey (CGSS) to examine health risk factors among solitary older adults in home-based care in China. The research findings indicate that gender, annual income, Mandarin language proficiency, and participation in health insurance significantly influence the self-rated health of solitary older individuals. Age and annual income emerge as factors affecting their physical health, while income and internet usage are identified as influencing factors on their psychological well-being. Furthermore, based on the results of multivariate logistic regression analysis, we constructed a line chart model for assessing the risk of self-assessed poor health. The evaluation of the model demonstrates its favorable accuracy, discriminative power, and risk prediction capability.
Data availability statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding authors.
Author contributions
KC: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. JQ: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. WW: Conceptualization, Methodology, Project administration, Writing – original draft. QH: Conceptualization, Methodology, Funding acquisition, Writing – review & editing. HQ: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang H Chen H. Aging in China: challenges and opportunities. CCDCW. (2022) 4:601–2. doi: 10.46234/ccdcw 2022.130, PMID: 35919296 PMC 9339359 · doi ↗ · pubmed ↗
- 2Jiang H Xiao S Hu H He H. Study on the measurement and influencing factors of care service demand of disabled elderly in urban and rural China. Int J Environ Res Public Health. (2022) 19. doi: 10.3390/ijerph 191711112, PMID: 36078829 PMC 9518346 · doi ↗ · pubmed ↗
- 3Holt-Lunstad J. The potential public health relevance of social isolation and loneliness: prevalence, epidemiology, and risk factors. Public Policy & Aging Report. (2018) 27:127–30. doi: 10.1093/ppar/prx 030 · doi ↗
- 4Fang G Yang D Wang L Wang Z Liang Y Yang J. Experiences and challenges of implementing universal health coverage with China's National Basic Public Health Service Program: literature review, regression analysis, and insider interviews. JMIR Public Health Surveill. (2022) 8:e 31289. doi: 10.2196/3128935867386 PMC 9356336 · doi ↗ · pubmed ↗
- 5Tu WJ Zeng X Liu Q. Aging tsunami coming: the Main finding from China's seventh National Population Census. Aging Clin Exp Res. (2022) 34:1159–63. doi: 10.1007/s 40520-021-02017-4, PMID: 34727357 · doi ↗ · pubmed ↗
- 6Ruan J Zheng W Zhuang Y. Everyday life experiences of Chinese community-dwelling oldest old who live alone at home. Int J Qual Stud Health Well Being. (2023) 18:2253937. doi: 10.1080/17482631.2023.2253937, PMID: 37667880 PMC 10481758 · doi ↗ · pubmed ↗
- 7Wang X Yuan X Xia B He Q Jie W Dai M. Living alone increases the risk of hypertension in older Chinese adults: a population-based longitudinal study. Innov Aging. (2023) 7:igad 071. doi: 10.1093/geroni/igad 071, PMID: 37502337 PMC 10370894 · doi ↗ · pubmed ↗
- 8Huang M Liu K Liang C Wang Y Guo Z. The relationship between living alone or not and depressive symptoms in older adults: a parallel mediation effect of sleep quality and anxiety. BMC Geriatr. (2023) 23:506. doi: 10.1186/s 12877-023-04161-0, PMID: 37608361 PMC 10463962 · doi ↗ · pubmed ↗