Association Between Baseline Echocardiographic Parameters and Acute Coronavirus Disease 2019 Infection in Hospitalized Patients
Jin Wang, Dongmei Yang, Cheng Cao

TL;DR
This study found that certain heart-related measurements are linked to a higher risk of getting COVID-19 in hospitalized patients.
Contribution
The study identifies baseline echocardiographic parameters as independent risk factors for acute COVID-19 infection.
Findings
Patients with COVID-19 had lower LVEF and higher A-wave velocity compared to those without infection.
LVEF and A-wave velocity were independent risk factors for COVID-19 infection.
Echocardiographic parameters did not change significantly during a one-month follow-up.
Abstract
Background The current study aimed to examine the association between baseline clinical and echocardiographic parameters with new-onset coronavirus disease 2019 (COVID-19) infection. Methodology We retrospectively enrolled consecutive hospitalized patients from our center during the national outbreak of the COVID-19 pandemic in China. Overall, 100 patients were enrolled, including 38 patients with COVID-19 infection. Results Compared with those without infection, patients with COVID-19 infection were more likely male (63.2% vs. 35.5%, p = 0.008), were older (59.08 vs. 52.35 years, p = 0.022), had higher heart failure (31.6% vs. 11.3%, p = 0.018) and hypertension (52.6% vs. 30.6%, p = 0.036) rates, had lower left ventricular ejection fraction (LVEF) (61.16% vs. 65.76%, p = 0.018), had higher A-wave velocity (86.84 vs. 73.63 cm/s, p = 0.003), and had and lower E/A ratio (0.85 vs…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
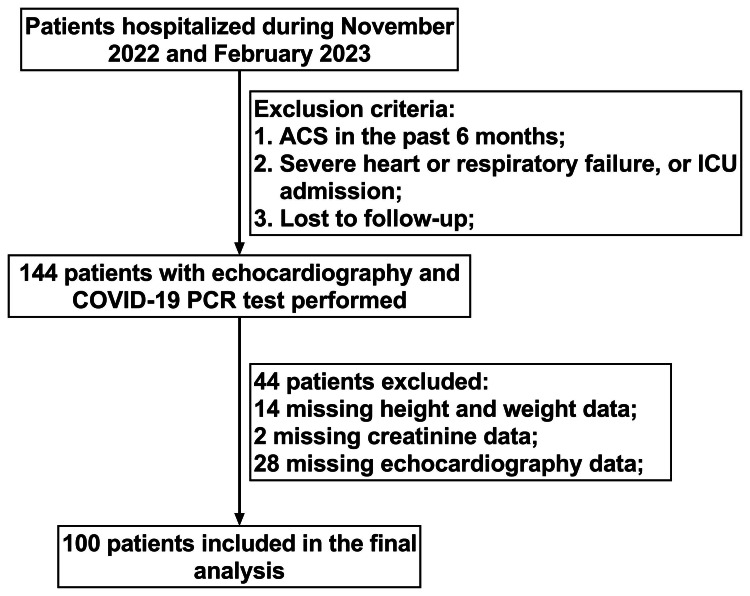 Figure 1
Figure 1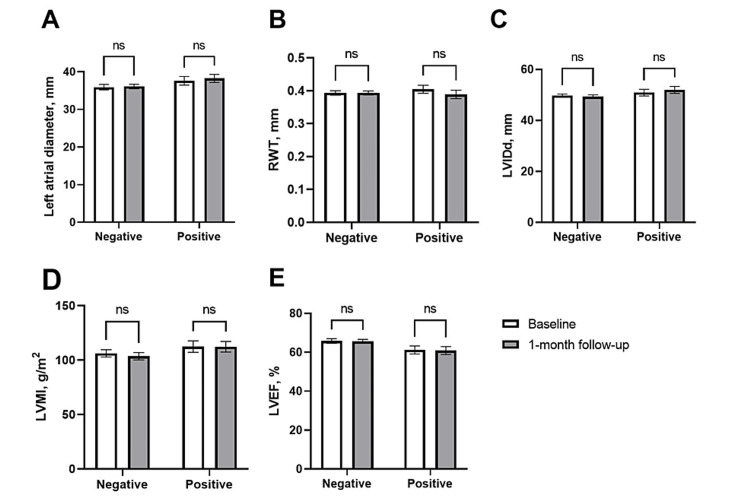 Figure 2
Figure 2| Negative, n = 62 | Positive, n = 38 | P-value | |
| Clinical characteristics | |||
| Male sex, n (%) | 22 (35.5%) | 24 (63.2%) | 0.008 |
| Age, years | 52.35 ± 1.81 | 59.08 ± 2.22 | 0.022 |
| Body mass index, kg/m2 | 23.47 (22.62, 24.33) | 23.63 (22.02, 25.24) | 0.749 |
| Systolic blood pressure, mmHg | 122.32 ± 1.86 | 126.76 ± 2.91 | 0.181 |
| Diastolic blood pressure, mmHg | 79.24 ± 1.39 | 79.00 ± 1.74 | 0.914 |
| Heart rate, beat/min | 82.18 (79.02, 85.33) | 87.29 (82.44, 92.14) | 0.108 |
| Estimated GFR, mL/min/1.73 m2 | 113.40 (101.26, 125.54) | 97.02 (79.44, 114.59) | 0.246 |
| Fasting blood glucose, mg/dl | 114.82 (102.77, 126.86) | 103.22 (94.79, 111.64) | 0.445 |
| Atrial fibrillation, n (%) | 4 (6.5%) | 3 (7.9%) | 1.000 |
| Heart failure, n (%) | 7 (11.3%) | 12 (31.6%) | 0.018 |
| Coronary heart disease, n (%) | 12 (19.4%) | 8 (21.1%) | 1.000 |
| Hypertension, n (%) | 19 (30.6%) | 20 (52.6%) | 0.036 |
| Diabetes, n (%) | 9 (14.5%) | 10 (26.3%) | 0.190 |
| Current smoking, n (%) | 11 (17.7%) | 5 (13.2%) | 0.589 |
| Current alcohol consumption, n (%) | 11 (17.7%) | 5 (13.2%) | 0.589 |
| Echocardiography | |||
| Left atrial diameter, mm | 35.92 ± 0.73 | 37.61 ± 1.15 | 0.197 |
| RWT, mm | 0.39 (0.38, 0.41) | 0.40 (0.38, 0.43) | 0.288 |
| LVIDd, mm | 49.73 (48.53, 50.92) | 50.92 (48.25, 53.60) | 0.957 |
| LVMI, g/m2 | 106.26 (99.55, 112.97) | 112.44 (101.76, 123.13) | 0.452 |
| LVEF, % | 65.76 (63.38, 68.14) | 61.16 (57.01, 65.31) | 0.018 |
| E-wave velocity, cm/s | 71.23 (66.18, 76.27) | 69.68 (62.09, 77.28) | 0.469 |
| A-wave velocity, cm/s | 73.63 ± 2.43 | 86.84 ± 3.78 | 0.003 |
| e’ septal, cm/s | 7.53 (6.94, 8.13) | 6.77 (6.09, 7.45) | 0.081 |
| E/A ratio | 1.04 (0.93, 1.14) | 0.85 (0.74, 0.96) | 0.015 |
| E/e’ ratio | 10.26 (9.07, 11.44) | 10.99 (9.45, 12.53) | 0.350 |
| Stroke volume index, mL/m2 | 45.78 (43.55, 48.00) | 43.43 (40.42, 46.43) | 0.087 |
| Cardiac index, L/min/m2 | 3.60 (3.42, 3.78) | 3.76 (3.42, 4.10) | 0.943 |
| Univariate analysis | Multivariate analysis | |||
| Variable | Odds ratio (95% CI) | P-value | Odds ratio (95% CI) | P-value |
| Male sex | 3.12 (1.35-7.22) | 0.008 | 2.42 (0.98-5.98) | 0.057 |
| Age, years | 1.04 (1.00-1.07) | 0.026 | - | |
| Atrial fibrillation | 1.24 (0.26-5.88) | 0.784 | Not selected | |
| Heart failure | 3.63 (1.28-10.28) | 0.015 | - | |
| Coronary heart disease | 1.11 (0.41-3.03) | 0.837 | Not selected | |
| Hypertension | 2.52 (1.09-5.80) | 0.030 | - | |
| Diabetes | 2.10 (0.77-5.78) | 0.149 | Not selected | |
| Left atrial diameter, mm | 1.04 (0.98-1.11) | 0.198 | Not selected | |
| RWT, mm | 19.39 (0.03-14589.26) | 0.380 | Not selected | |
| LVIDd, mm | 1.03 (0.97-1.10) | 0.356 | Not selected | |
| LVMI, g/m2 | 1.01 (0.99-1.02) | 0.301 | Not selected | |
| LVEF, % | 0.96 (0.93-1.00) | 0.049 | 0.96 (0.91-1.00) | 0.041 |
| E wave velocity, cm/s | 1.00 (0.98-1.02) | 0.721 | Not selected | |
| A wave velocity, cm/s | 1.03 (1.01-1.05) | 0.004 | 1.04 (1.01-1.06) | 0.003 |
| e’ septal, cm/s | 0.85 (0.71-1.03) | 0.105 | Not selected | |
| E/A ratio | 0.26 (0.08-0.86) | 0.028 | - | |
| E/e’ ratio | 1.03 (0.95-1.13) | 0.453 | Not selected | |
| Stroke volume index, ml/m2 | 0.97 (0.93-1.02) | 0.203 | Not selected | |
| Cardiac index, L/min/m2 | 1.25 (0.78-2.03) | 0.358 | Not selected | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Long-Term Effects of COVID-19 · COVID-19 and healthcare impacts
Introduction
Since December 2019, the coronavirus disease 2019 (COVID-19) pandemic has significantly impacted human life. Detrimental prognosis in COVID-19 involves patient demographics and cardiovascular risk factors and diseases, such as older age, high blood pressure, and heart failure [1-3]. Cardiac injury is common in patients with COVID-19 infection and contributes to poor outcomes [4]. Transthoracic echocardiography is widely used, and early studies showed that clinical and subclinical cardiac impairment analyzed by echocardiography was common in COVID-19 patients [5-10]. These studies were mainly performed among patients who were already infected with or recovered from COVID-19 [8-11]. However, the differences in baseline clinical and echocardiographic parameters between patients infected and not infected with COVID-19 remain unclear, especially for the Omicron variant. After the outbreak of the COVID-19 pandemic, China strongly controlled the disease, with restrictions gradually relaxed in November 2022 [12,13]. Following this, the number of patients infected with COVID-19 increased sharply and contributed to the nationwide outbreak of the COVID-19 pandemic (the Omicron variant wave) in China [12,13]. During this period, people were exposed to COVID-19 at the same time and most patients were infected with COVID-19 for the first time. In this study, we sought to determine the association between baseline clinical and echocardiographic parameters with acute COVID-19 infection among hospitalized patients in our center during this national outbreak.
Materials and methods
We retrospectively enrolled consecutive patients hospitalized in our center from November 2022 to February 2023. This was the nationwide outbreak period of COVID-19 infection in China, during which most people were infected with COVID-19 for the first time [12,13]. The inclusion criteria were (1) patients aged 18 years and older; (2) patients for whom echocardiography was performed; and (3) patients for whom the COVID-19 test was performed by polymerase chain reaction assay. The exclusion criteria were (1) patients with acute coronary syndrome in the past six months before enrollment; (2) patients with severe heart failure (patients with New York Heart Association grade IV), respiratory failure (patients with respiratory support), or those admitted to the intensive care unit; and (3) patients lost to follow-up. The flow chart of the study is shown in Figure 1. The study was performed in accordance with the Declaration of Helsinki and was approved by the hospital ethics committee (approval number: 2023-RE-085).
Flowchart of the study.ACS = acute coronary syndrome; ICU = intensive care unit; COVID-19 = coronavirus disease 2019; PCR = polymerase chain reaction
Clinical data were obtained from the hospital’s electronic medical system. Body mass index (BMI) was calculated using weight (kg) divided by the square of height (m). The modified Modification of Diet in Renal Disease formula was used to evaluate the estimated glomerular filtration rate [14].
Transthoracic echocardiography was conducted in accordance with the recommendations of previous studies [15]. Images were taken from standardized views and measured by a single experienced sonographer blinded to patients’ clinical data. Relative wall thickness (RWT) and left ventricular mass index (LVMI) were evaluated, as described previously [16]. Stroke volume index and cardiac index were calculated by indexed stroke volume and cardiac output to body surface area, respectively. Body surface area was calculated, as described previously [16]. Echocardiography date from around 1 month after enrollment were collected.
The continuous variables were presented as mean ± standard error (SE) or median value ± interquartile range and were analyzed using the t-test or Mann-Whitney U test, as appropriate. The categorical variables were presented as numbers (%) and were analyzed with the chi-square test. The logistic regression model was applied to explore the associations of baseline clinical and echocardiographic parameters with acute COVID-19 infection. A two-way analysis of variance with the post-hoc test was applied to compare echocardiographic parameters in the enrollment and one-month follow-up period. Statistical analysis was performed using SPSS version 27 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 9 (GraphPad Software, San Diego, CA, USA). A two-sided p-value <0.05 was considered significant.
Results
A total of 100 patients were enrolled in the final analysis, including 38 patients with COVID-19 infection (Table 1). Compared with those in the negative group, patients with COVID-19 infection were more likely to be male (63.2% vs. 35.5%, p = 0.008), were older (59.08 vs. 52.35 years, p = 0.022), and had higher heart failure (31.6% vs. 11.3%, p = 0.018) and hypertension (52.6% vs. 30.6%, p = 0.036) rates. Furthermore, patients with COVID-19 infection had lower left ventricular ejection fraction (LVEF) (61.16% vs. 65.76%, p = 0.018), higher A-wave velocity (86.84 vs. 73.63 cm/s, p = 0.003), and lower E/A ratio (0.85 vs 1.04, p = 0.015) compared with patients in the negative group. Moreover, there were no statistically significant differences in lower septal e’-wave velocity (6.77 vs. 7.53 cm/s, p = 0.081) and lower stroke volume index (43.43 vs. 45.78 mL/m^2^, p = 0.087) in patients with COVID-19 infection than those in the negative group. On the other hand, no statistically significant differences in other clinical and echocardiographic parameters were observed between the two groups.
Table 2 presents the association between both baseline clinical and echocardiographic characteristics with acute COVID-19 infection. On univariate logistic regression, male sex (odds ratio (OR) = 3.12, 95% confidence interval (CI) = 1.35 to 7.22, p = 0.008), age (OR = 1.04, 95% CI = 1.00 to 1.07, p = 0.026), heart failure (OR = 3.63, 95% CI = 1.28 to 10.28, p = 0.015), hypertension (OR = 2.52, 95% CI = 1.09 to 5.80, p = 0.030), LVEF (OR = 0.96, 95% CI = 0.93 to 1.00, p = 0.049), A-wave velocity (OR = 1.03, 95% CI = 1.01 to 1.05, p = 0.004), and E/A ratio (OR = 0.26, 95% CI = 0.08 to 0.86, p = 0.028) were associated with acute COVID-19 infection. On multivariate logistic regression, only LVEF (OR = 0.96, 95% CI = 0.91 to 1.00, p = 0.041) and A-wave velocity (OR = 1.04, 95% CI = 1.01 to 1.06, p = 0.003) remained significantly associated with acute COVID-19 infection, while male sex (OR = 2.42, 95% CI = 0.98 to 5.98, p = 0.057) was not statistically significant associate with acute COVID-19 infection.
The effect of COVID-19 infection on short-term cardiac injury was determined by comparing the baseline and one-month follow-up echocardiographic parameters in patients with and without COVID-19 infection. As shown in Figure 2, there were no significant changes in echocardiographic parameters, such as left atrial diameter, left ventricular internal diameter in diastole (LVIDd), RWT, left ventricular mass index (LVMI), or LVEF in the negative and positive groups between baseline and one-month follow-up (p > 0.05 for all).
Comparison of echocardiographic parameters in patients between baseline and one-month follow-up after COVID-19.RWT = relative wall thickness; LVIDd = left ventricular internal diameter in diastole; LVMI = left ventricular mass index; LVEF = left ventricular ejection fraction; ns = non-significant
Discussion
Myocardial injury is common in COVID-19-infected patients and contributes to poor outcomes [4]. Echocardiography is a useful and widely available clinical tool to assess cardiac structure and function. Earlier studies showed that patients infected with COVID-19 were frequently associated with impaired cardiac function assessed by echocardiography [5-7,10]. Further, echocardiographic cardiac abnormality in COVID-19-infected cases was associated with adverse outcomes [6,7,17]. However, no studies compared the differences in clinical and echocardiographic parameters between acute COVID-19-infected and non-infected patients, especially for the Omicron variant. Further, few studies evaluated the association between baseline echocardiographic markers and acute COVID-19 infection. In addition, little is reported about the short-term echocardiographic changes after the Omicron variant of COVID-19 infection.
There is heterogeneity in the association between clinical parameters and the risk of COVID-19 infection. In hospitalized and community-dwelling populations in the United States, cardiovascular diseases were significantly associated with a higher odds rate of COVID-19 infection [1,2]. However, a meta-analysis including patients from China showed that cardiovascular metabolic diseases did not increase the susceptibility to COVID-19 infection [18]. In a community-dwelling population, younger adults and females were reported to have higher COVID-19 rates [1]. However, other studies demonstrated that both older age and male sex were associated with higher COVID-19 rates and poor outcomes [3,19-21]. Here, we observed that patients infected with COVID-19 were older and had higher rates of high blood pressure and heart failure. Further, we found that male gender was associated with higher odds of COVID-19 infection. Higher pulmonary cells expressing angiotensin-converting enzyme 2 (ACE2) in males than females may contribute to these sex differences because ACE2 facilitates COVID-19 invasion [22]. Differences in study population, disease severity, and differences in COVID-19 variants may contribute to the above-mentioned differences. Further studies are required to clarify the association between clinical parameters and COVID-19 infection.
Previous studies reported that COVID-19 infection was associated with acute echocardiographic cardiac dysfunction [23]. These studies were mainly conducted among patients who were already infected with or recovered from COVID-19 [8-11]. However, the association between baseline echocardiographic parameters and COVID-19 infection among hospitalized patients remains less clear, especially for the Omicron variant. In this study, we found that the left ventricular systolic and diastolic functions were relatively normal, which means mild COVID-19. Further, significantly lower LVEF and higher A-wave velocity were observed in the COVID-19-infected group compared with the controls. These differences were recorded at the onset of COVID-19 infection, which reflected a background subclinical echocardiographic cardiac dysfunction. Our study suggested that echocardiographic parameters, such as LVEF and A-wave velocity, may be used to predict future COVID-19 risk.
There is inconsistency regarding the long-term echocardiographic change in COVID-19-infected patients. Early studies conducted in those infected with COVID-19 found that both left and right ventricular function were impaired during the three-month follow-up, especially in severe and moderate cases [24]. However, other studies conducted during the first and second waves showed no significant changes in long-term follow-up (four months to one year) echocardiographic parameters of left or right ventricular in COVID-19-infected patients 25,26]. One study conducted in hospitalized COVID-19 cases found no changes in one-month follow-up echocardiographic parameters in fully vaccinated patients [7]. Similarly, our study found no significant change in echocardiographic parameters during the one-month follow-up. It has been suggested that disease severity, cardiac injury during the acute phase, and vaccination status may influence the results; hence, more studies are needed.
There are several limitations of this study. First, the left ventricular global longitudinal strain (GLS) was not analyzed. It has been reported that left ventricular GLS is more sensitive and can detect subclinical cardiac dysfunction in COVID-19-infected cases, especially in the mild population [8-10]. Second, the right ventricular was not measured. It has been reported that echocardiographic right ventricular abnormality was common and correlated with poor outcomes [27-29]. Lastly, the retrospective design prevented us from determining the causal relationship between baseline clinical and echocardiographic parameters and COVID-19 infection.
Conclusions
In this single-center retrospective study, we demonstrated that patients infected with COVID-19 were older, were more likely to be male, and had higher hypertension and heart failure rates. Further, echocardiographic parameters such as LVEF and A-wave velocity were independently associated with higher odds of COVID-19 infection. Lastly, COVID-19 infection did not significantly alter echocardiographic parameters in the short-term follow-up period. To our knowledge, this is the first report to investigate the association between baseline clinical and echocardiographic parameters and COVID-19 infection in hospitalized patients in China.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Association between cardiovascular risk and coronavirus disease 2019: findings from 2021 National Health Interview Survey Ann Epidemiol Liu L May NS Sato PY Srivastava P Mc Clure LA 178220233696362110.1016/j.annepidem.2023.03.005PMC 10033151 · doi ↗ · pubmed ↗
- 2Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area JAMA Richardson S Hirsch JS Narasimhan M 2052205932320203232000310.1001/jama.2020.6775 PMC 7177629 · doi ↗ · pubmed ↗
- 3Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China JAMA Intern Med Wu C Chen X Cai Y 93494318020203216752410.1001/jamainternmed.2020.0994 PMC 7070509 · doi ↗ · pubmed ↗
- 4Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19)JAMA Cardiol Guo T Fan Y Chen M 811818520203221935610.1001/jamacardio.2020.1017 PMC 7101506 · doi ↗ · pubmed ↗
- 5Echocardiographic findings in patients with COVID-19 with myocardial injury during the Omicron variant surge Am J Cardiol Alam L Omar AM Talebi S Narula J Argulian E 16816917220223538292610.1016/j.amjcard.2022.03.008PMC 8976229 · doi ↗ · pubmed ↗
- 6Cardiologic manifestations in Omicron-type versus wild-type COVID-19: a systematic echocardiographic study J Am Heart Assoc Ghantous E Shetrit A Hochstadt A 012202310.1161/JAHA.122.027188 PMC 997364936695308 · doi ↗ · pubmed ↗
- 7Association of echocardiographic findings with in-hospital mortality of COVID-19 patients and their changes in one-month follow-up; a cohort study Arch Acad Emerg Med Mosallami Aghili SM Khoshfetrat M Asgari A Arefizadeh R Mohsenizadeh A Mousavi SH 010202210.22037/aaem.v 10i 1.1787 PMC 967670536426171 · doi ↗ · pubmed ↗
- 8Paradoxical increase in left atrial strains early after Covid-19 infection, a result of comprehensive recovery phase four-chamber strains study Int J Cardiovasc Imaging Samiei N Rahnamoun Z Kamali M Asadian S Rezaei Y Ghadrdoost B Shirkhanloo N 143714473920233716270810.1007/s 10554-023-02865-3PMC 10171154 · doi ↗ · pubmed ↗