A triad of double aortic arch, bicuspid valve, and aortic dilation: treat the right lesion!
Fabienne Dirbach, Christopher Roy, Matthias Stuber, Tobias Rutz

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
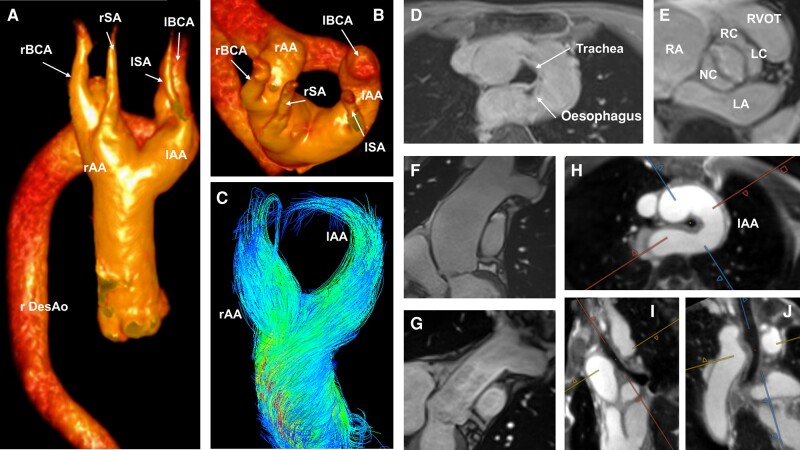 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Tracheal and airway disorders · Congenital Heart Disease Studies
In a 71-year-old, healthy patient, an enlarged mediastinum was noticed on a chest X-ray performed for persistent cough after a respiratory infection. Computed tomography (CT) revealed a double aortic arch (DAA), a congenital heart lesion deriving from non-involution of the fourth aortic arches. Cardiac magnetic resonance (CMR) with 4D flow was performed showing the DAA with relatively balanced aortic arches (flow left arch, net 20 mL/heartbeat; right arch, net 15 mL/heartbeat; Panels A to C; Supplementary material online, Movies S1 and S2), a tracheo-oesophageal compression (Panel D), and a fusion of both arches into a right descending aorta. Although the images suggested a highly symptomatic vascular ring, typically presenting with stridor, barky cough, dyspnoea, or dysphagia, the patient had never presented any of those symptoms. Cardiac magnetic resonance revealed further a bicuspid aortic valve with dilation of the ascending aorta of 52 mm (Panels E and F).
The heart team decided to surgically replace the ascending aorta at a supra-coronary level with a 28 mm Gelweave tube (Panel G) as the patient fulfilled the indications according to the European Society of Cardiology guidelines due to concomitant arterial hypertension. Owing to the absence of symptoms, the age and the balanced two aortic arches, the DAA, and the bicuspid valve, only showing mild insufficiency, remained untouched.
The post-operative course was uneventful. The patient remained asymptomatic to the DAA, although a free-running cardiac and respiratory motion-resolved 5D whole-heart suggested persistent symptomatic tracheo-oesophageal compression (Panels H–J; Supplementary material online, Movies S3 and S4). Four-dimensional flow revealed a now completely balanced DAA (15 mL/heartbeat/branch each). Due to the concomitant absence of respiratory and swallowing symptoms and a normal clinical examination, no further investigations were undertaken.
This case highlights the role of advanced CMR techniques in addition to clinical evaluation to choose the right lesion requiring treatment.
Supplementary Material
ytae156_Supplementary_Data