Regularly irregular tachycardia and QRS alternans? Think twice!
João Grade Santos, Sofia Almeida, Luís Brandão

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
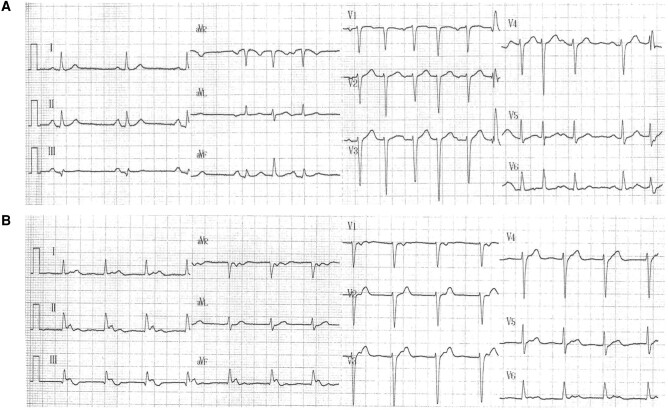 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac electrophysiology and arrhythmias · Atrial Fibrillation Management and Outcomes
ECG Challenge
A 67-year-old male, with no relevant priors, was referred to Electrophysiology (EP) evaluation after failing multiple antiarrhythmic medical therapy (beta-blockers, propafenone, and sotalol) for highly symptomatic paroxysms of tachyarrhythmia.
The patient showed two different 12-lead electrocardiograms (ECG) shown below (Panels A and B).
Additional Holter monitoring is provided in Supplementary material online, Figure S1.
Question 1: Panel A demonstrates sinus rhythm with a brief period of regularly irregular QRS alternans tachycardia with a P wave preceding only every other QRS complex (as further depicted in the Supplementary material online, Figure S1).
Panel B demonstrates a regular rhythm with narrow QRS complexes with inferior axis P waves visualized after the QRS at the initial part of the ST segment.
Which of the following could not explain the observed tachyarrhythmia?
Atrial Bigeminy with aberrancy.Ventricular Bigeminy.Atrioventricular nodal re-entrant tachycardia (AVNRT) with 2:1 retrograde block.Dual atrioventricular nodal non-reentrant tachycardia (DAVNNT).Ortodromic atrioventricular re-entrant tachycardia (AVRT).
Correct answer: e)
Explanation: In the differential diagnosis of the narrow-complex tachycardia with a P:R ratio of 1:2 and QRS alternans between narrow and wide complex one must consider either ventricular bigeminy, atrial bigeminy with the latter P-wave entailed in the preceding T wave and some degree of aberrancy, AVNRT with 2:1 retrograde block and DAVNNT also known as ‘double fire’ tachycardia (as depicted in Supplementary material online, Figure S2).^1^
An AVRT could not produce a narrow complex tachycardia with a P:R ratio of 1:2 as both atria and ventricle are part of the arrythmia circuit.
Question 2: Given the most likely diagnosis, what would be the expected findings in the EP study?
An accessory pathway.Dual nodal physiology.An atrial focus.A ventricular focus.A macro-reentrant circuit.
Correct answer: b)
Explanation: Panel A could be interpreted as nodal conduction through a fast pathway followed by simultaneous conduction through a slow and fast pathway and Panel B uniquely conduction through a slow pathway.
As such, the expected finding would be dual nodal physiology. In this patient, an EP study was conducted (see Supplementary material online, Figures S3–S5) and dual nodal physiology was identified with the presence of AH jump and induction of AVNRT. At the end of an atrial pacing drive, there was a period in which each atrial beat produced two slightly different QRS complexes, thus making the case for DAVNNT.
Question 3: Given the most likely EP study findings, what would be the most appropriate management?
Ablation of the focal arrhythmia.Ablation of the accessory pathway.Ablation of the slow pathway.Ablation of the macro-reentrant circuit.Antiarrhythmic drug therapy.
Correct answer: c)
Explanation: Dual atrioventricular nodal non-reentrant tachycardia occurs in patients with dual AV physiology in which each P wave conducts anterogradely both down the fast and slow pathways producing two distinct QRS complexes. Although this is a rare entity, it can result in tachycardia-induced cardiomyopathy and is easily treated by catheter ablation of the slow pathway.^2^ In this patient, a slow pathway ablation was performed with resolution of symptoms and electrocardiographic findings.
**
Consent: Direct written consent was obtained by the patient for this manuscript.
Funding: No funding was involved in the development of this manuscript.
Supplementary Material
ytae150_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burri H, Hoffmann J, Zimmermann M. Double fire tachycardia. Heart 2012;98:958.22543311 10.1136/heartjnl-2012-301800 · doi ↗ · pubmed ↗
- 2Lee W, Quinn FR. Dual AV nodal non-reentrant tachycardia-induced cardiomyopathy. J Electrocardiol 2022;73:55–58.35667212 10.1016/j.jelectrocard.2022.05.003 · doi ↗ · pubmed ↗