Post-surgical inflammatory neuropathy after anterior cruciate ligament repair: a case report
Lisa Y. Sun, Andrew T. Gray, Matthias R. Braehler

TL;DR
A patient developed post-surgical inflammatory neuropathy after an ACL repair, highlighting a rare but important cause of nerve damage following surgery.
Contribution
This case report highlights post-surgical inflammatory neuropathy as a potentially under-recognized cause of perioperative neuropathy.
Findings
The patient developed sciatic nerve-related neuropathy after anterior cruciate ligament surgery.
The diagnosis of post-surgical inflammatory neuropathy was made after ruling out other causes.
The patient improved with conservative management, suggesting potential for corticosteroid therapy in similar cases.
Abstract
Unanticipated symptoms of peripheral nerve damage following surgery are distressing to both the patient and their clinical team, including surgeons, anesthesiologists, and neurologists. The causes that are commonly considered for perioperative neuropathy can include surgical trauma, positioning-related injury, or injury related to a regional anesthetic technique. However, these cases often do not have a clear etiology and can occur without any apparent periprocedural anomalies. Postoperative inflammatory neuropathy is a more recently described, and potentially underrecognized cause of perioperative neuropathy which may improve with corticosteroid therapy. Therefore, it is an important etiology to consider early in the evaluation of perioperative neuropathy. An otherwise healthy patient presented for left anterior cruciate ligament reconstruction. He underwent femoral and sciatic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
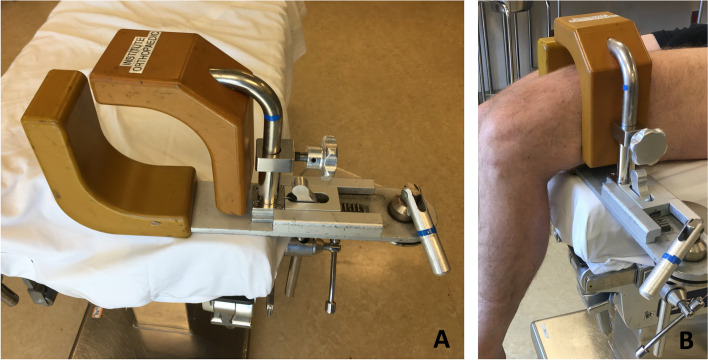 Figure 1
Figure 1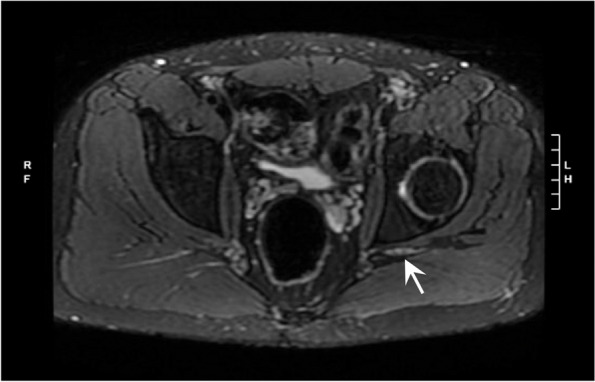 Figure 2
Figure 2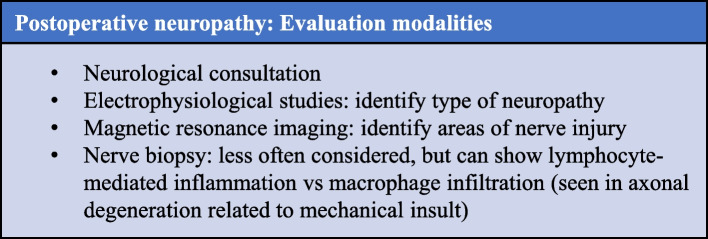 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Nerve Disorders · Orthopedic Surgery and Rehabilitation · Shoulder Injury and Treatment
Background
Post-surgical neuropathies are usually attributed to mechanical injuries (such as nerve compression, stretch, contusion, or transection), local anesthetic toxicity, and ischemia. However, they can also occur in the setting of post-surgical nerve inflammation, which has only recently been better characterized in the literature (Staff NP et al. 2010) and can present as focal, multifocal, or diffuse neuropathy. These inflammatory neuropathies can occur temporally and spatially distant from the surgical time and site. There are a limited number of case reports of post-surgical inflammatory neuropathies, all with varying presentations (Staff NP et al. 2010; Rattananan et al. 2014; Ahn et al. 2011; Cetiz 2017; Warner and Warner 2014; Laughlin et al. 2014). Our case demonstrates the utility of a thorough evaluation of postoperative neuropathy, which resulted in the diagnosis of post-surgical inflammatory neuropathy.
Case presentation
A 25-year-old, 99 kg, otherwise healthy male presented for left anterior cruciate ligament reconstruction with patellar tendon autograft. The patient received femoral and sciatic ultrasound-guided peripheral nerve blocks with 0.5% ropivacaine (25 ml per site). The blocks were uneventful, with no paresthesia and no high pressure noted during manual injection. The patient received general anesthesia with a supraglottic airway. The patient was positioned supine with the operative leg slightly elevated in a thigh holder and flexed 90° at the knee (Fig. 1). The tourniquet was inflated to 250 mmHg for 32 min. No posterior work, such as a hamstring harvest, was performed.Fig. 1A Thigh holder. B Depiction of leg position within thigh holder. The padding and thigh tourniquet used on an actual patient’s leg in a thigh holder is not shown
The patient developed shock-like pain, tingling, and numbness in the plantar aspect of his foot as well as numbness along the left lateral leg on postoperative day (POD) 2, with no motor deficits on exam. His neuropathic pain worsened over the following weeks. He did not endorse systemic inflammatory symptoms, such as fevers or chills. Neurologic consultation on POD 23 identified decreased sensation to light touch, vibration, and pinprick in the sciatic territory; reduced toe flexion and extension (3/5 according to the Medical Research Council scale); reduced foot dorsiflexion and plantar flexion (4/5); and absent left Achilles reflex. Electromyography showed decreased motor nerve conduction responses for the left peroneal and tibial nerves and absent responses for the left sural and superficial peroneal nerves. These results suggested a sciatic neuropathy, without evidence of radiculopathy, likely due to perioperative inflammatory sciatic neuritis. Conservative management and close follow-up were recommended.
The patient was also seen by pain management specialists, and other possible diagnoses were considered, including radiculopathy and complex regional pain syndrome. Magnetic resonance (MR) imaging of the lumbar spine on POD 42 showed left L5-S1 disk extrusion with nerve compression but left L5, S1 foraminal steroid epidural injections were performed without relief. The patient’s hyperesthesia led to the consideration of complex regional pain syndrome, although no vasomotor or sudomotor symptoms were noted. On POD 52, a lumbar sympathetic nerve block (0.25% bupivacaine) along with a distal ankle block (1% lidocaine with 0.375% bupivacaine) were performed, and they provided significant pain relief. Ongoing diagnostic uncertainty prompted MR neurogram from the lumbar spine to the foot on POD 67, which showed neuritis in the sciatic nerve distribution starting in the pelvis (above the level of surgery, thigh holder, tourniquet, and nerve blocks). This was consistent with a diagnosis of post-surgical inflammatory neuropathy (Fig. 2). At this time, the patient was experiencing improved pain control after adjustment of a variety of neuropathic and narcotic pain medications over his postoperative course. He also had improved function and weight-bearing on the operative extremity with ongoing physical therapy. On 1-year follow-up, the patient had significant improvement with near resolution of symptoms, with a pain regimen consisting of duloxetine and diclofenac.Fig. 2. Magnetic resonance neurogram showing asymmetric T2 hyperintensity and enlargement of the left sciatic nerve
Discussion
This case report describes the clinical course, evaluation, and diagnosis of post-surgical inflammatory sciatic neuropathy, in a patient without any known risk factors. As is common in the setting of postoperative neuropathy, this patient experienced evolving symptoms, multi-disciplinary consultations, a broad differential diagnosis, and a variety of therapies for pain management. His final diagnosis of post-surgical inflammatory neuropathy was ultimately supported by imaging studies and the exclusion of other etiologies, as there are no known markers for this condition. His course improved with conservative management, but consideration for immunosuppressive treatment may have been given to a more severe or worsening clinical course.
The incidence of post-surgical inflammatory neuropathy is unclear, and it may be under-appreciated (Staff NP et al. 2010). The cause of this condition is likely multifactorial, and given its heterogeneous presentation in prior case reports, it may encompass multiple different entities. It is thought to be an immunological response to stress, such as surgery. Based on a retrospective study (Staff NP et al. 2010), additional possible risk factors may include diabetes mellitus, tobacco use, cancer, and infection; in this case, the patient did not have any of these suggested risk factors. Given the rarity of this condition, more case reports and studies would be useful to further elucidate predisposing factors. This condition should be included in the differential diagnosis for post-surgical neuropathy, particularly when there is no clear mechanical insult to explain the neuropathy.
Evaluation of postoperative nerve injury includes neurological consultation, as well as consideration of ancillary testing (Fig. 3). Electrophysiological studies can be useful for defining the type of neuropathy. MR imaging can help to identify areas of nerve injury. Nerve biopsy is less often considered, but it can show lymphocyte-mediated inflammation (as opposed to macrophage infiltration, which is seen in axonal degeneration related to mechanical insult) (Staff NP et al. 2010; Rattananan et al. 2014; Ahn et al. 2011).Fig. 3. Evaluation modalities for postoperative neuropathy
The optimal treatment and management of inflammatory neuropathy is yet to be determined. Some cases have improved with conservative management, as with this patient. Other cases of inflammatory neuropathy have improved with immunotherapy, including intravenous immunoglobulin and steroids (such as methylprednisolone and prednisone) (Staff NP et al. 2010; Rattananan et al. 2014; Ahn et al. 2011; Cetiz 2017; Warner and Warner 2014; Laughlin et al. 2014). Although this treatment has only been reported in retrospective studies and case reports, it does suggest that early consideration and prompt diagnosis of this entity is important so that suppression of the immune response can be considered. For this reason, it is important for anesthesiologists and surgeons to be aware of this condition when confronted with a case of post-surgical neuropathy. Future prospective studies would be helpful to demonstrate the true incidence of post-surgical inflammatory neuropathy, predisposing risk factors, effectiveness of immunotherapy, and prophylactic role of steroids pre- or intra-operatively.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahn KS Kopp SL Watson JC Scott KP Trousdale RT Hebl JR Postsurgical inflammatory neuropathy Reg Anesth Pain Med.20113640340510.1097/AAP.0b 013e 31821 e 650321654554 · doi ↗ · pubmed ↗
- 2Cetiz A Post-surgical focal inflammatory neuropathy of the sciatic nerve Acta Neurol Belg.201711793193310.1007/s 13760-017-0805-828612270 · doi ↗ · pubmed ↗
- 3Laughlin RS Dyck PJ Watson JC Ipsilateral inflammatory neuropathy after hip surgery Mayo Clin Proc.20148945446110.1016/j.mayocp.2013.10.02724398433 · doi ↗ · pubmed ↗
- 4Rattananan W Thaisetthawatkul P Dyck PJ Postsurgical inflammatory neuropathy: a report of five cases J Neurol Sci.201433713714010.1016/j.jns.2013.11.03524332011 · doi ↗ · pubmed ↗
- 5Staff NP Engelstad J Klein CJ Amrami KK Spinner RJ Dyck PJ Post-surgical inflammatory neuropathy Brain.20101332866288010.1093/brain/awq 25220846945 · doi ↗ · pubmed ↗
- 6Warner ME Warner MA Inflammatory neuropathy: a potentially treatable etiology for a subset of perioperative neuropathies Mayo Clin Proc.20148943443610.1016/j.mayocp.2014.02.00124613034 · doi ↗ · pubmed ↗