Dapagliflozin versus sacubitril–valsartan for heart failure with mildly reduced or preserved ejection fraction
Ronen Arbel, Abed N. Azab, Mansi Oberoi, Enis Aboalhasan, Artyom Star, Khaled Elhaj, Fouad Khalil, Hilmi Alnsasra

TL;DR
This study compares the cost-effectiveness of two drugs for heart failure patients with mildly reduced or preserved ejection fraction.
Contribution
The study provides a novel cost-per-outcome analysis comparing dapagliflozin and sacubitril–valsartan for heart failure treatment.
Findings
Dapagliflozin had a lower cost-per-outcome than sacubitril–valsartan for preventing heart failure hospitalizations and cardiovascular death.
The cost needed to treat for all-cause mortality was also lower with dapagliflozin.
Scenario analyses were used to adjust for differences in study populations.
Abstract
Heart failure with preserved ejection fraction (HFpEF) is associated with an increased risk of heart failure (HF) hospitalizations and cardiovascular death (CVD). Both dapagliflozin and sacubitril–valsartan have recently shown convincing reductions in the combined risk of CVD and HF hospitalizations in patients with HF and mildly reduced ejection fraction (HFmrEF) or HFpEF. We aimed to investigate the cost-per-outcome implications of dapagliflozin vs sacubitril–valsartan in the treatment of HFmrEF or HFpEF patients. We compared the annualized cost needed to treat (CNT) to prevent the composite outcome of total HF hospitalizations and CVD with dapagliflozin or sacubitril–valsartan. The CNT was estimated by multiplying the annualized number needed to treat (aNNT) by the annual cost of therapy. The aNNT was calculated based on data collected from the DELIVER trial for dapagliflozin and a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
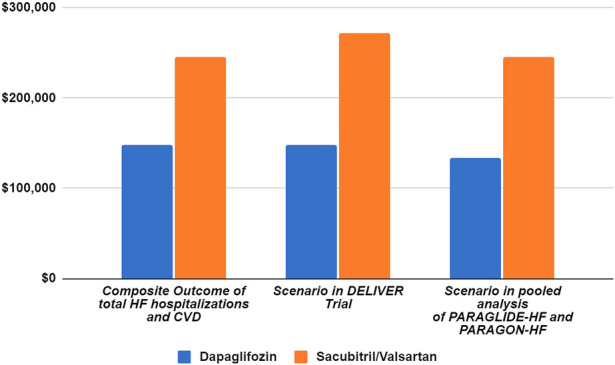 FIGURE 1
FIGURE 1| Deliver N = 6,263 | Paragon-HF N = 4,822 | Paraglide-HF N = 466 | ||||
|---|---|---|---|---|---|---|
| Dapagliflozin (N = 3,131) | Placebo (N = 3,132) | Sacubitril–valsartan (N = 2,407) | Valsartan (N = 2,389) | Sacubitril–valsartan (N = 233) | Valsartan (N = 233) | |
|
| 71.8 ± 9.6 | 71.5 ± 9.5 | 72.7 ± 8.3 | 72.8 ± 8.5 | 71.0 (61.0-78.0) | 72.0 (62.0-79.0) |
|
| 1,364 (43.6) | 1,383 (44.2) | 1,241 (51.6) | 1,238 (51.8) | 121 (51.9) | 121 (51.9) |
|
| ||||||
|
| 630 (20.1) | 644 (20.6) | 297 (12.3) | 310 (13.0) | 3 (1.3) | 3 (1.3) |
|
| 81 (2.6) | 78 (2.5) | 52 (2.2) | 50 (2.1) | 50 (21.5) | 52 (22.3) |
|
| 2,214 (70.7) | 2,225 (71.0) | 1,963 (81.6) | 1,944 (81.4) | 176 (75.5) | 176 (75.5) |
|
| ||||||
|
| 2,225 (71.0) | 2,399 (76.6) | 1,866 (77.5) | 1,840 (77.0) | 102 (43.8) | 101 (43.3) |
|
| 807 (25.8) | 724 (23.1) | 458 (19.0) | 474 (19.8) | 117 (50.2) | 112 (48.1) |
|
| 10 (0.3) | 8 (0.3) | 8 (0.3) | 11 (0.5) | 4 (1.7) | 10 (4.3) |
|
| 54.0 ± 8.6 | 54.3 ± 8.9 | 57.6 ± 7.8 | 57.5 ± 8.0 | 55.2 ± 8.06 | 55.7 ± 8.07 |
|
| 1401 (44.7) | 1405 (44.9) | 1046 (43.5) | 1016 (42.5) | 107 (45.9) | 119 (51.1) |
|
| 2,755 (88.0) | 2,798 (89.3) | 2,304 (95.7) | 2,280 (95.4) | 228 (97.9) | 219 (94.0) |
|
| 61 ± 19 | 61 ± 19 | 63 ± 19 | 62 ± 19 | 47.4 (36.4-62.2) | 51.1 (39.4-64.8) |
|
| ||||||
| Parameter | Dapagliflozin | Sacubitril–valsartan |
|---|---|---|
| Number of patients in the control arm | 3,132 | 2,622 |
| Follow-up (years) | 2.3 | 2.8 |
| Patient-years of therapy in the control arm | 7,203.6 | 7,341.6 |
| Number of events in the control arm | 1,057 | 1,181 |
| Annualized event rate in the control arm (%) | 14.67 | 16.09 |
| Number of patients in the intervention arm | 3,131 | 2,640 |
| Patient-years of therapy in intervention arm | 7,201.3 | 7,392 |
| Annualized event rate in the intervention arm, % (95% CI) | 11.30 (9.83%–13.06%) | 13.83 (12.06%–15.76%) |
| Annualized absolute event rate reduction, % (95% CI) | 3.37 (1.61%–4.84%) | 2.25 (0.32%–4.02%) |
| Annualized number needed to treat (95% CI) | 30 (21–62) | 44 (25–311) |
| Annual drug cost (US) | $ 4,951.57 | $ 5,576.06 |
| Cost needed to treat to prevent one event (95% CI) | $ 148,547.13 ($ 103,983–$ 306,997.39) | $ 245,346.77 ($ 139,401.58–$ 1,734,155.60) |
| Dapagliflozin | Sacubitril–valsartan | |
|---|---|---|
| Annualized event rate in the control arm (%) | 7.30 | 5.11 |
| Annualized event rate in the intervention arm, % (95% CI) | 6.86 (6.06%–7.81%) | 4.85 (4.19%–5.62%) |
| Annualized absolute event rate reduction, % (95% CI) | 0.44 (0%–1.24%) | 0.26 (0%–0.92%) |
| Annualized number needed to treat (95% CI) | 228 (81–∞) | 392 (109–∞) |
| All-cause mortality (95% CI) | $ 1,128,958.15 ($ 401,077.24–∞) | $ 2,185,816.71 ($ 607,790.87–∞) |
| Annualized absolute risk | CNT for dapagliflozin | CNT for sacubitril–valsartan | |
|---|---|---|---|
| Simulation of the annualized event rate in the RCT control group | 14.67% (As in DELIVER) | Base case: $ 148,547.13 ($ 103,983–$ 306,997.39) | $ 273,226.94 ($ 150,553.62–$ 1,901,436.46) |
| 16.09% (as in pooled PARAGLIDE-HF and PARAGON-HF) | $ 133,692.39 ($ 94,079.83–$ 282,239.49) | Base case: $ 245,346.77 ($ 139,401.58–$ 1,734,155.60) |
| Price estimate | US (low estimate) | US (high estimate) | ||
|---|---|---|---|---|
| Treatment | Dapagliflozin | Sacubitril–valsartan | Dapagliflozin | Sacubitril–valsartan |
| Annual cost | $ 3,301.05 | $ 3,717.38 | $ 6,602.09 | $ 7,434.74 |
| Annual budget | $ 735,000,000 | |||
| CNT (95% CI) | $ 99,031.42 ($ 69,321.99 - $ 204,664.94) | $ 163,565 ($ 92,934 - $ 1,156,104) | $ 198,062.83 ($ 138,643.98 - $ 409,329.86) | $ 327,129 ($ 185,869 - $ 2,312,707) |
| Prevented events within the budget, N (95% CI) | 7,421 (3,591–10,602) | 4,498 (635–7,908) | 3,710 (1,795–5,301) | 2,246 (317–3,954) |
| Dapagliflozin | Sacubitril–valsartan | |||
|---|---|---|---|---|
| Rate ratio | Event rate (100 patient-years) | Rate ratio | Event rate (100 patient-years) | |
| aAR in the control arm | 14.67% | 15.30% | 16.09% | 16.80% |
| aAR in the intervention arm | 11.30% | 11.80% | 13.83% | 14.50% |
| aARR | 3.37% | 3.50% | 2.25% | 2.30% |
| aNNT | 30 | 29 | 44 | 43 |
| CNT | $ 148,547.13 | $ 143,595.53 | $ 245,346.77 | $ 239,770.71 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Heart Failure Treatment and Management · Cardiovascular Function and Risk Factors
1 Introduction
Nearly half of all cases of heart failure (HF) in the United States are caused by HF with a preserved ejection fraction (HFpEF) (Tsao et al., 2023). By 2030, HF is expected to account for 69.8 billion dollars of the annual healthcare cost in the United States (Tsao et al., 2023). As the population ages, it is predicted that HFpEF will continue to become a more important public health issue (Tsao et al., 2023).
There is well-established evidence that sodium–glucose transporter 2 inhibitors (SGLT2Is) and angiotensin receptor/neprilysin inhibitors (ARNIs) are effective treatments for HF with a reduced ejection fraction (HFrEF) (McMurray et al., 2014; 2019; Packer et al., 2020). However, in HFpEF patients, spironolactone and sacubitril–valsartan have only shown marginal benefits (Pitt et al., 2014; McMurray et al., 2020). Recently, dapagliflozin demonstrated the most convincing reduction in adverse outcomes in HFpEF patients (Solomon et al., 2022).
Dapagliflozin in the heart failure with mildly reduced or preserved ejection (DELIVER) trial randomly assigned 6,263 patients with HF and left ventricular ejection fraction (LVEF) ≥ 40% to receive either dapagliflozin or placebo (Solomon et al., 2022). Dapagliflozin demonstrated a significant reduction in the risk of worsening HF or cardiovascular death (CVD) (Solomon et al., 2022).
The prospective comparison of ARNI with ARB [angiotensin receptor blockers] global outcomes in HF with the preserved ejection fraction (PARAGON-HF) trial randomly assigned 4,796 patients with symptomatic HF and LVEF ≥45% to receive either sacubitril–valsartan or valsartan alone (Solomon et al., 2019). The sacubitril–valsartan regimen demonstrated a non-statistically significant reduction in death from cardiovascular causes or hospitalization for HF, compared to the placebo (Solomon et al., 2019). However, a re-analysis of the results of this trial suggested a statistically significant difference (Felker et al., 2021).
Similarly, the Prospective comparison of ARNI with ARB Given following stabiLization In DEcompensated HFpEF (PARAGLIDE-HF) trial randomly assigned 466 patients with LVEF ≥ 40% stabilized after a worsening HF event to receive either sacubitril–valsartan or valsartan alone (Mentz et al., 2023). The sacubitril–valsartan regimen led to a statistically significant reduction in pro-B-type natriuretic peptide and a potential clinical benefit compared with valsartan, with fewer cardiovascular and renal events (Mentz et al., 2023).
The recent pooled analysis of all participants in the PARAGLIDE-HF and PARAGON-HF trials showed a significant reduction in the composite of total worsening HF events and CVD with sacubitril–valsartan compared to valsartan alone (Vaduganathan et al., 2023).
Although both dapagliflozin and sacubitril–valsartan can be attractive therapeutic options for patients with HFmrEF or HFpEF, a key aspect of treatment plans remains the associated cost. A recent study from our group compared dapagliflozin with the sacubitril–valsartan regimen in HFrEF patients and identified a monetary benefit for dapagliflozin over sacubitril–valsartan (Arbel et al., 2021). The aim of the present study is to compare the cost-per-outcome implications of prescribing dapagliflozin versus sacubitril–valsartan to prevent HF events and CVD in patients with HFmrEF or HFpEF.
2 Methods
2.1 Data sources for drug efficacy
Outcome data for dapagliflozin and sacubitril–valsartan were extracted from the DELIVER trial and pooled analysis of the PARAGLIDE-HF and PARAGON-HF trials, respectively (Solomon et al., 2022; Vaduganathan et al., 2023).
2.2 Outcome measures
The primary outcome was the cost needed to treat (CNT) to prevent one event of the composite outcome of total HF hospitalizations and CVD. CNT was also estimated for the prevention of one event of all-cause mortality. The analysis was performed from the perspective of healthcare payers in the United States.
2.3 Cost needed to treat analysis
The number of preventable hospitalizations for HF and CVD achievable with dapagliflozin or sacubitril–valsartan was estimated by dividing the predefined maximum available budget by the CNT to prevent one event. The budget limit, $735 million, was set as the United States’ threshold suggested by the Institute for Clinical and Economic Review (ICER) (Institute for Clinical and Economic Review, 2023). The CNT was calculated by multiplying the aNNT by the annual treatment cost (Mayne et al., 2006). Drug costs were calculated as 75% of the US National Average Drug Acquisition Cost (NADAC), extracted in July 2023 (Medicaid.gov, 2023).
2.4 Annualized number needed to treat analysis
The aNNT was calculated as one divided by the annualized absolute risk reduction (aARR), the absolute difference between the annualized absolute risk (aAR) in the control and treatment arms. The aAR of treatments was calculated by dividing the number of events in each study arm by patient-years of treatment (Mayne et al., 2006).
2.5 Scenario analysis
To evaluate the robustness of CNT results and mitigate differences between the baseline risk of the randomized controlled trial (RCT) populations, we performed one-way sensitivity analysis on parameters that may affect the NNT and CNT figures (Mendes et al., 2017): the risk of events in the control arm of the RCTs and the annual costs of the compared interventions.
2.6 Sensitivity analysis
To mitigate the differences in the risk of HF events in the RCTs, we simulated the effect of each drug while using each of the other drug control arms’ event rates. For the sensitivity analysis of the cost of therapy, we used the full NADAC price as the upper bound and 50% of the NADAC price as the lower bound, as recommended for use in US cost-effectiveness analyses (Levy et al., 2018).
3 Results
3.1 Patient populations
A total of 11,525 patients were included in the DELIVER and pooled analysis of the PARAGLIDE-HF and PARAGON-HF trials. The baseline characteristics of both trial participants are detailed in Table 1. The median follow-up time was longer in the pooled analysis of PARAGLIDE-HF and PARAGON-HF (2.8 years) compared to that of DELIVER (2.3 years).
3.2 Annualized number needed to treat and cost needed to treat
The step-by-step calculations of the aNNT and CNT are outlined in Table 2. The annual drug costs are 5,576.06 for sacubitril–valsartan. The CNT to prevent one event of total worsening HF events and CVD (composite outcome) was 103,982.99–306,997.39) for dapagliflozin and 139,401.58–1,734,155.60) for sacubitril–valsartan (Figure 1).
Scenario analysis of cost needed to treat based on the DELIVER and pooled analysis of PARAGLIDE-HF and PARAGON-HF trials.
The CNT results of all-cause mortality are given in Table 3. Dapagliflozin had a lower CNT compared to a sacubitril–valsartan regimen to prevent one event of all-cause mortality: 401,077.24–∞) vs 607,790.87–∞).
3.3 Scenario analysis
Table 4 details the results of the sensitivity analysis performed by simulating the use of different annualized event rates in the control arm, according to the event rates in each of the trials.
3.4 Sensitivity analysis
Table 5 and Figure 1 detail the results of the sensitivity analysis with different prices from the United States. If the annual predefined budget of $735 million was allocated entirely for the prevention of total HF hospitalizations and CVD, a higher number of events would be prevented using dapagliflozin (3,710 events, [95% CI: 1,795–5,301]), as compared to sacubitril–valsartan (2,246 events, [95% CI: 317–3,954] when utilizing the US high-cost estimate. We performed an additional sensitivity analysis using the reported event rate per 100 patient-years in the original studies, yielding similar CNT values to those derived from the reported rate ratio (Table 6).
4 Discussion
In this cost–benefit study, leveraging data from the DELIVER, PARAGLIDE-HF, and PARAGON-HF trials, we demonstrated that dapagliflozin provides a better monetary value compared to sacubitril–valsartan for preventing the composite outcome of total worsening HF events and CVD and all-cause mortality as an individual outcome among patients with HFpEF.
As the population ages, the escalating prominence of HFpEF as a pivotal public health concern is anticipated (Tsao et al., 2023). This is associated with a cost that is estimated to reach $69.8 billion in annual healthcare spending by 2030 (Clark and Velazquez, 2020).
The DELIVER trial randomized patients with HFmrEF or HFpEF to either dapagliflozin or placebo. Over a median of 2.3 years, a statistically significant reduction in the primary composite outcome of HF hospitalization or CVD was found with dapagliflozin compared to the placebo (Solomon et al., 2022). The PARAGON-HF trial included patients with a similar clinical profile and randomized them to receive sacubitril–valsartan or valsartan alone. The trial narrowly missed statistical significance for its primary endpoint of a composite of total hospitalizations for HF and death from cardiovascular causes (Solomon et al., 2019). Similarly, the PARAGLIDE-HF trial showed that sacubitril–valsartan led to a greater reduction in plasma NT-proBNP levels compared to valsartan alone. However, the trial was not adequately powered to assess clinical outcomes (Mentz et al., 2023). Hence, Vaduganathan et al. (2023) performed a pooled analysis of PARAGLIDE-HF and PARAGON-HF trials; compared with valsartan, sacubitril–valsartan significantly reduced worsening HF events and CVD in the pooled analysis of all participants (Vaduganathan et al., 2023).
The 2023 Focused Update of the 2021 European Society of Cardiology (ESC) and 2022 American Heart Association/American College of Cardiology/Heart Failure Society of America (AHA/ACC/HFSA) guidelines for HF provide a Class 1 and Class 2a recommendation for SGLT2Is and Class 2b for ARNI for patients with HFmrEF and HFpEF (Heidenreich et al., 2022; McDonagh et al., 2023).
A recent meta-analysis of 13 studies with a total of 29,875 HF patients with LVEF >40% demonstrated that a quadruple-agent combination of SGLT2I, ARNI, beta blocker, and a mineralocorticoid receptor antagonist provides the largest reduction in the risk of CVD and HF hospitalization, largely attributed to the effect of the triple combination of SGLT2I, ARNI, and mineralocorticoid receptor antagonist. The benefit was more pronounced in HFmrEF patients (Zafeiropoulos et al., 2023). A combined SGLT2I and sacubitril–valsartan regimen has been approved and recommended for HFrEF (McDonagh et al., 2021), but its practice is not well-established for HFpEF patients. The high cost is likely to be a major limitation, serving as a barrier to prescribing the conjunctive regimen for HF patients (Luo et al., 2020).
Variances in the pharmacological mechanisms of action of dapagliflozin and sacubitril–valsartan may influence the reported differences in their clinical outcomes. The basic pharmacodynamic effect of SGLT2Is is the inhibition of SGLT2 in the proximal tubule of the nephron, leading to decreased glucose reabsorption into the blood and thus inducing a hypoglycemic effect (Vallon and Verma, 2021; Packer, 2022; 2023). However, these medications exert numerous other pharmacological properties that may contribute to their therapeutic benefits (Mustroph et al., 2018; Byrne et al., 2020; Quagliariello et al., 2021; Vallon and Verma, 2021; Koufakis et al., 2022; Packer, 2022; 2023). For example, dapagliflozin has been suggested to suppress neurohormonal activation, improve systolic function, and decrease the incidence of cardiac arrhythmias in patients with HF (Koufakis et al., 2022). Similarly, empagliflozin has been shown to inhibit the function of Ca^2+^/calmodulin-dependent kinase II, leading to improved myocardial contractility and a reduction of arrhythmias among HF patients (Mustroph et al., 2018). Additionally, empagliflozin was reported to inhibit the activity of the nucleotide-binding domain-like receptor protein 3 (NLRP3)-associated cellular pathways, resulting in a significant increase in left ventricular fractional shortening and ejection fraction and an overall improvement in cardiac function (Byrne et al., 2020; Quagliariello et al., 2021). It is worth noting in this regard that many natural compounds, such as resveratrol, possess some of the pharmacological properties of gliflozins, including potent inhibition of the NLRP3 inflammasome (Cocetta et al., 2021) and, therefore, may become a useful adjuvant treatment of cardiovascular disease (Sung and Dyck, 2015; Bonnefont-Rousselot, 2016; Raj et al., 2021) and other disorders (Cocetta et al., 2021; Amini et al., 2023). As for ARNI, these medications not only confer the regular, well-established pharmacological outcomes of angiotensin receptor blockers (such as valsartan) but also combine the therapeutic effects deriving from the inhibition of the enzyme neprilysin by sacubitril (Hubers and Brown, 2016; Velazquez et al., 2019; Pascual-Figal et al., 2021; Abdin et al., 2022). Neprilysin degrades atrial and brain natriuretic peptides, bradykinin, and other vasoactive peptides; its inhibition by sacubitril leads to a prominent vasodilatory effect and additional positive renal and cardiovascular outcomes (Hubers and Brown, 2016; Velazquez et al., 2019; Pascual-Figal et al., 2021; Abdin et al., 2022).
A European health-economic analysis of the DELIVER trial found that the addition of dapagliflozin to a standard of care is very likely cost-effective for HFmrEF or HFpEF in several European countries (Booth et al., 2023). Dapagliflozin treatment was predicted to increase quality-adjusted life years (QALYs) and life-years by 0.231 and 0.354, respectively, and prolong the time spent in the best quartile of the Kansas City Cardiomyopathy Questionnaire total symptom score (KCCQ-TSS) by 4.2 months. The incremental cost-effectiveness ratios were £7,761, €9,540, and €5343/QALY in the United Kingdom, Germany, and Spain, respectively (Booth et al., 2023). Similarly, Tang and Sang. (2023) performed a cost-utility analysis based on the DELIVER study and the national statistical database. The study showed that the adjunct use of dapagliflozin to standard of care among patients with HFpEF or HFmrEF was cost-effective in China at a willingness-to-pay value of 12,652.5/QALY ([Tang and Sang, 2023](#B45)). Most recently, [Cohen et al. (2023)](#B11) performed an economic evaluation using a simulation model of US adults with HFpEF who meet the eligibility criteria of the EMPEROR-Preserved or DELIVER trials. They found that the addition of an SGLT2I to the standard of care increased quality-adjusted survival by 0.19 QALYs at an increased cost of 26,300 compared with standard of care. The resulting incremental cost-effectiveness ratio was $141,200 per QALY gained, which is of intermediate or low economic value compared with standard of care in HFpEF (Cohen et al., 2023).
There has been limited data on the cost-effectiveness of sacubitril–valsartan in patients with HFpEF. Recently, Wang et al. (2023) investigated the cost-effectiveness of sacubitril–valsartan as an alternative to valsartan in Chinese patients with HFpEF. They found the ICER for sacubitril–valsartan to be 46,610/life-year), higher than the willingness-to-pay threshold and hence not cost-effective (Wang et al., 2023). However, a recent economic evaluation using participant-level data from the PARADIGM-HF and PARAGON-HF trials (n = 13,264) found sacubitril–valsartan to be more cost-effective at lower EF ranges with a high economic value for patients with HFrEF or HFmEF (EF ≤ 50%) and at least of intermediate value to an EF ≤ 60% compared with renin–angiotensin system inhibitors. Only in those with EFs of 45% or greater did sacubitril–valsartan yield an incremental cost-effectiveness ratio of $127,172 per QALY gained (Bhatt et al., 2023).
Although a growing body of evidence supports the role of SGLT2Is and ARNI in reducing HF hospitalization and CVD among HF patients, their use is still limited in clinical practice partially due to their cost. The unaffordability of pharmacotherapy due to high cost is a major reason for nonadherence to prescribed medications (De Avila et al., 2021; Simon et al., 2021; Dusetzina et al., 2023). Our analysis attempts to provide some cost-per-outcome insight when prescribing dapagliflozin and sacubitril–valsartan. To the best of our knowledge, this is the first cost-per-outcome comparison between dapagliflozin and sacubitril–valsartan in patients with HFmrEF and HFpEF. Future studies are needed to confirm these findings.
4.1 Limitations
Our study has several limitations that warrant consideration. First, despite the similarity in patient populations across both trials, the presence of apparent differences between them poses a limitation to our analysis. We attempted to mitigate this through sensitivity analysis by simulating the effects of each drug within each RCT. Second, it is important to note that our analysis does not substitute the need for a comprehensive cost-effectiveness assessment in relation to QALY and potential cost savings associated with preventing HF hospitalization. Although such an assessment is necessary, it remains unavailable due to the recent completion of DELIVER and the pooled analysis of PARAGLIDE-HF and PARAGON-HF trials. A third limitation pertains to the reliance on aNNT estimates in our CNT figure, which has its own restrictions (Saver and Lewis, 2019). However, NNT has been found to be useful for assisting decision-making in many clinical settings (Mendes et al., 2017; Saver and Lewis, 2019) and is required by the Consolidated Standards of Reporting Trials statement to be reported in RCT publications (Moher et al., 2012). Moreover, the annualization of NNT for comparing RCTs and therapies is a method employed in previous studies (Chew et al., 2009; Fonarow et al., 2011). Lastly, our findings are based on the published results of only a limited number of HFpEF patients which may restrict the generalizability of our analysis to a broader HFpEF population.
5 Conclusion
In analyzing data from the DELIVER and the pooled analysis of PARAGLIDE-HF and PARAGON-HF trials, the CNT to prevent HF hospitalizations and CVD was lower for dapagliflozin compared to sacubitril–valsartan for HFmrEF and HFpEF patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdin A.Schulz M.Riemer U.Hadëri B.Wachter R.Laufs U. (2022). Sacubitril/valsartan in heart failure: efficacy and safety in and outside clinical trials. Esc. Heart Fail 9, 3737–3750. 10.1002/ehf 2.14097 35921043 PMC 9773772 · doi ↗ · pubmed ↗
- 2Amini P.Moazamiyanfar R.Dakkali M. S.Khani A.Jafarzadeh E.Mouludi K. (2023). Resveratrol in cancer therapy: from stimulation of genomic stability to adjuvant cancer therapy: a comprehensive review. Curr. Top. Med. Chem. 23, 629–648. 10.2174/1568026623666221014152759 36239730 · doi ↗ · pubmed ↗
- 3Arbel R.Aboalhasan E.Hammerman A.Azuri J. (2021). Dapagliflozin vs. sacubitril-valsartan for prevention of heart failure events in non-diabetic patients with reduced ejection fraction: a cost per outcome analysis. Eur. J. Prev. Cardiol. 28, 1665–1669. 10.1093/eurjpc/zwaa 136 33624086 · doi ↗ · pubmed ↗
- 4Bhatt A. S.Vaduganathan M.Claggett B. L.Fonarow G. C.Packer M.Pfeffer M. A. (2023). Health and economic evaluation of sacubitril-valsartan for heart failure management. JAMA Cardiol. 8, 1041–1048. 10.1001/jamacardio.2023.3216 37755814 PMC 10534998 · doi ↗ · pubmed ↗
- 5Bonnefont-Rousselot D. (2016). Resveratrol and cardiovascular diseases. Nutrients 8, 250. 10.3390/nu 8050250 27144581 PMC 4882663 · doi ↗ · pubmed ↗
- 6Booth D.Davis J. A.Mc Ewan P.Solomon S. D.Mc Murray J. J. V.De Boer R. A. (2023). The cost‐effectiveness of dapagliflozin in heart failure with preserved or mildly reduced ejection fraction: a European health‐economic analysis of the DELIVER trial. Eur. J. Heart Fail 25, 1386–1395. 10.1002/ejhf.2940 37344985 · doi ↗ · pubmed ↗
- 7Byrne N. J.Matsumura N.Maayah Z. H.Ferdaoussi M.Takahara S.Darwesh A. M. (2020). Empagliflozin blunts worsening cardiac dysfunction associated with reduced NLRP 3 (Nucleotide-Binding domain-like receptor protein 3) inflammasome activation in heart failure. Circ. Heart Fail 13, e 006277. 10.1161/CIRCHEARTFAILURE.119.006277 31957470 · doi ↗ · pubmed ↗
- 8Chew D. P.Huynh L. T.Liew D.Astley C.Soman A.Brieger D. (2009). Potential survival gains in the treatment of myocardial infarction. Heart 95, 1844–1850. 10.1136/hrt.2009.174276 19666459 · doi ↗ · pubmed ↗