Early Impressions and Adoption of the AtriAmp for Managing Arrhythmias Following Congenital Heart Surgery
Scott M. Leopold, Diane H. Brown, Xiao Zhang, Xuan T. Nguyen, Awni M. Al-Subu, Krisjon R. Olson

TL;DR
This paper explores early experiences with AtriAmp, a new device for managing arrhythmias in pediatric patients after heart surgery.
Contribution
The study provides insights into the early adoption and impact of AtriAmp on clinical workflow and diagnosis in the PICU.
Findings
AtriAmp accelerated diagnosis and treatment of arrhythmias in post-operative patients.
Providers reported increased confidence in arrhythmia diagnosis accuracy with AtriAmp.
The device improved education on post-operative arrhythmias by reducing reliance on consultations.
Abstract
AtriAmp is a new medical device that displays a continuous real-time atrial electrogram on telemetry using temporary atrial pacing leads. Our objective was to evaluate early adoption of this device into patient care, understand how it affected clinical workflow, and identify unforeseen benefits or limitations. Qualitative study using inductive analysis of semi-structured interviews to identify dominant themes Single center, tertiary, academic 21-bed mixed pediatric intensive care unit (PICU) PICU multidisciplinary team members (Pediatric intensivists, PICU Nurse Practitioners, PICU nurses and Pediatric Cardiologists) who were early adopters of the AtriAmp (n=14) Three prominent themes emerged from qualitative analysis of the early adopters’ experiences. (1) Accelerated time from arrhythmia event to diagnosis, treatment, and determination of treatment effectiveness; (2) Increased…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
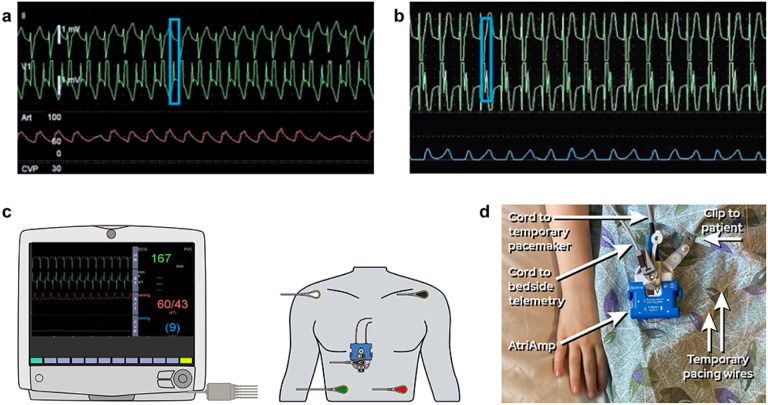 Figure 1
Figure 1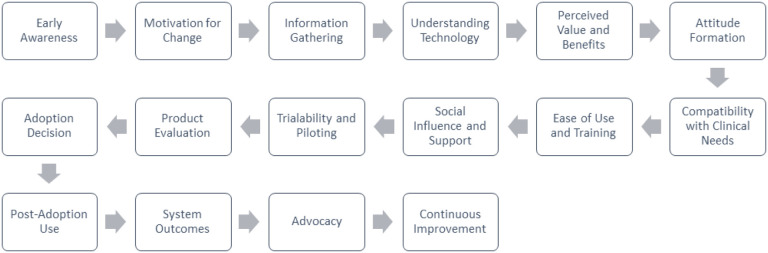 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Cardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments
Introduction
Advances in postoperative cardiac surgical care in the PICU have depended, in part, on medical technologies used to continuously monitor critically ill patients. Despite calls to do so, few studies focus on how and why technological advances are sustained within the PICU[1, 2]. With postoperative arrhythmias, no significant technological advances have occurred over the last few decades until recently[3–9]. AtriAmp (Atrility Medical, Madison, WI, USA) is a novel single-use device with continuous real-time and retrospective atrial electrogram monitoring capacity. This device has the potential to revolutionize the care of postoperative arrhythmias and decrease morbidity in these patients[10–16].
New technologies, however, can face significant barriers to adoption within the PICU. Diffusion of innovation theory suggests that adoption of new technologies follows a predictable pattern, with early adopters leading implementation[17, 18]. Thus, integral to the assessment of a new device like AtriAmp is understanding how early adopters perceive the device. This qualitative research aimed to evaluate adoption of AtriAmp into patient care, understand how it affected clinical workflow, and identify unforeseen benefits or limitations[19].
Methods
We performed a qualitative study using grounded theory methods. We used an inductive analytical approach to evaluate how the AtriAmp affected patient care and workflows within a PICU with about 140 postoperative cardiac surgery admissions per year. Participants, whose interviews are the source data, were drawn from all levels of patient care including PICU nurses, PICU nurse practitioners (NP), pediatric intensivists, and pediatric cardiologists. A total sample of early adopters, defined as all of those on the multidisciplinary team who reported using the device within six months of its introduction, were interviewed and concepts that emerged during analysis were further developed to elaborate concepts under study. This iterative approach allows for the generation of explanatory models regarding adoption of the device grounded in empirical data about its use in pediatric intensive care. We continued to recruit participants and conduct interviews until no further early adopters could be identified.
One investigator (D.H.B), a pediatric critical care fellow, developed the interview guide and conducted audio-taped interviews in person between August and October 2021 lasting between 4–22 minutes; approximately 6 months after the device was first used on patients in our PICU and about 4–6 months before its use became the standard for postoperative cardiac care in our PICU. Interviews employed a semi-structured format (Supplemental Digital Content 1). The guide consisted of open-ended questions with targeted probes regarding: 1) experience and training in using the device, 2) how the device affected patient care, and 3) how the device affected clinical workflows. No repeat interviews were performed, and all participants spoke English. All interviews were transcribed verbatim.
Four members of the research team performed open, axial, and inductive coding of the interview transcripts. First, 3 authors (S.M.L., K.R.O, X.Z.) independently reviewed each transcript and open-coded for providers experiences and perspectives on early adoption (open-coding). The 3 authors met in person at regular intervals to review transcripts and codes, examine coding differences in coding and interpretation, and proximity to thematic saturation. This team included two pediatric critical care fellows (S.M.L. and D.B.) one medical anthropologist (K.R.O.), a graduate student in sociology (X.N.) a clinical research scientist in pediatric cardiology (X.Z.), and a pediatric intensivist (A.A.) whose backgrounds allowed diversity in interpretation of the data. We selected themes based on their prevalence and consistency in the data and a final schema describing early adoption practices (selective coding). We also performed member checking, in which study results were shared with study participants and their input was considered in the final analysis. NVivo 11 was used by K.R.O. to annotate transcripts, codes, and memos.
The University of Wisconsin-Madison institutional review board approval was obtained, and procedures were followed in accordance with the ethical standards of the institutional committee on human experimentation and with the Helsinki Declaration of 1975 (IRB2020–1146, approved on February 2, 2020, study title “Arrhythmia Identification using the AtriAmp”. Informed consent was obtained from all participants.
Results
We approached 14 providers who self-identified as early adopters of Atri-Amp, all of whom provided informed consent, and participated in a semi-structured interview (Table 1).
Overall, the early adopters of the AtriAmp cited early adoption due to the device’s simplicity and fidelity, highlighting: 1) a reduction in time between arrhythmia event and diagnosis and/or treatment, 2) improved accuracy in arrhythmia diagnosis, 3) improved familiarity and education of atrial electrograms and postoperative arrhythmias and 4) some technical but easily overcome challenges. Exemplary quotations illustrative of these themes can be found in Table 2.
Faster arrhythmia diagnosis and quicker time to treatment
Participants described adopting the AtriAmp because it eliminated the cumbersome intermediate steps of acquiring an atrial electrogram. In doing so, it improved diagnostic efficiency while also avoiding episodes of hypotension that can occur due to delays in atrial electrogram acquisition. Once a treatment was started, the AtriAmp also allowed for better identification of treatment success or failure. Figure 1 demonstrates what the AtriAmp signal looks like in line with the surface electrogram on bedside telemetry and illustrates how the AtriAmp is connected to the patient and bedside monitor.
More confident and accurate arrhythmia diagnosis
Early adopters we interviewed tended to view arrythmias within the broader context of their experience rather than being narrowly wedded to conventional biomarkers. They reported that through its continuous collection of atrial signals which are available for review both retrospectively and in real-time, the AtriAmp improves diagnostic accuracy. Those arrhythmia events that are episodic are still caught and can be reviewed, which may have been lost by the prior standard of care. Participants described that they were able to avoid diagnostic uncertainty, unnecessary treatments for wrong diagnoses, and iatrogenic treatments. Early adopters cited a preference for continuous rather than intermittent monitoring, and the AtriAmp is the first of its kind to provide higher fidelity continuous monitoring for postoperative arrhythmias. One pediatric intensivist went so far as to say that “it should become the new standard of care.” In line with this approach, study participants often said that Atri-Amp helped them to formulate more accurate treatment targets during a critical period. Benefits of the AtriAmp over previously used standards of care are shown in Table 3.
Increased familiarity and improving education in atrial electrograms and post-op arrhythmias
Early adopters found the AtriAmp to have significant educational value. For less experienced providers, the device’s real time monitoring creates just-in-time learning opportunities around postoperative arrhythmias. In particular, the PICU NPs cited the device’s utility in creating these opportunities. A subset of these NPs noted a discernible learning curve regarding atrial electrogram interpretation, which led them to spend more time learning about all types of postoperative arrhythmias. Early adopters considered this especially important when the tendency of providers and the health system is to default to sub-specialty consultation, where technology can fill important gaps in knowledge and patient care.
Technical challenges and learning curves
Participants noted several technical challenges involving device set-up, positioning and placement in the bed, controlling patient interactions, and confusion with pacing through the device. Importantly, providers noted that these pearning curves did not result in any perceivable difference in the quality of care provided to the patients and that all challenges were overcome with additional practice. These issues could be averted in the future through pre-use multidisciplinary educational sessions and/or training programs. Participants described acquiring skills in rhythm management and providing education to the team in order to educate those who did not adopt AtriAmp early. These findings highlight the need for more research to determine the acceptability, scalability, and outcomes of AtriAmp use in pediatric intensive care. Here we offer insights into the practice changes that support adoption of new technologies in the PICU.
Discussion
While survival of critical illness, and particularly critical cardiac conditions, has improved dramatically we have limited data about how contributing technological innovations are disseminated and implemented in the PICU. In this study, we performed qualitative investigation into the initial impressions and issues encountered by early adopters of the AtriAmp, a new health technology device, in a pediatric intensive care unit on patients who are postoperative from cardiac surgery. In our study, the AtriAmp was overwhelmingly perceived as a significant improvement in patient care by all early adopters, regardless of their role in the PICU. When we spoke to this select group, common themes emerged around the device’s ease of use, accuracy, reliability, and educational utility.
The AtriAmp eliminated many of the cumbersome intermediate steps of acquiring an atrial electrogram following a postoperative arrhythmia event in the PICU. The providers interviewed in this study described that the new technology, by being continuously in line with the surface ECG, eliminated diagnostic difficulties with intermittent or episodic arrhythmias. In doing so, the AtriAmp accelerated the time between arrhythmia event and diagnosis, allowing for more rapid initiation of appropriate treatment and more rapid identification of whether the treatment had a beneficial effect. In addition, by using available resources more efficiently and focusing more time and energy on the patient rather than diagnosing an arrhythmia, many of pediatric intensivists described that AtriAmp created a safer and more secure environment for their patient. These findings are consistent with the literature on diffusion of innovation, which suggests that innovations that demonstrate a relative advantage, are compatible with the adopters’s need, and provide tangible results are most likely to diffuse through the population.
The AtriAmp also provided an unforeseen benefit as an educational tool for teaching about postoperative arrhythmias and in interpreting atrial ECGs. Many of the PICU NPs and PICU RNs commented on how their understanding of post-op arrhythmias and their ability to interpret atrial ECGs had improved since the introduction of the new device[19]. One of the PICU physicians also noted he was receiving more questions from the bedside RNs regarding things seen on the atrial waveform since initiation of the AtriAmp. Several providers commented on how ongoing education and review of atrial waveforms would benefit them. Learning and skill development are ongoing processes that are embedded in the PICU environment, and the use of the AtriAmp as an educational tool may have contributed to the development of new practices and habits in rhythm identification. These findings are consistent with the literature on early adopters of health technology, which suggests that these individuals often become opinion leaders and are more receptive to new technologies due to their intrinsic motivation to improve patient care and advance their own knowledge and skills[17].
Although all providers received a lecture on device setup and atrial ECG interpretation prior to the introduction of the AtriAmp, some unforeseen learning curves were encountered. The PICU RNs noted that it took some practice to get used to how to insert the temporary pacing wires into the device, and for neonates and infants, careful planning was required in positioning the device in the bed with the patient to avoid pulling on the wires or getting the patient tangled in the wires. However, all nurses were able to overcome these challenges with additional practice, and none of them felt like the device significantly interfered with their care of the patients. These findings are consistent with the literature on the adoption of new inventions in healthcare, which suggests that while new inventions may require some learning and adaptation, healthcare providers are generally receptive to new technologies that are relatively simple to learn how to use, can be easily experimented with, and demonstrate tangible improvements to patient care[20–22].
This study highlights the importance of understanding the environment in which new health technologies are introduced. Diffusion of innovation theory teaches that new healthcare technologies are most likely to be adopted if: 1) they demonstrate a relative advantage to the current standard of care, 2) they are compatible with the values and needs of the population, 3) they are relatively easy to understand and learn how to use, 4) they can be tested and experimented on and allow for adaptations, and 5) they produce tangible results[17, 18]. As demonstrated, the AtriAmp met all five of these criteria. While it is relatively unusual for new technologies to be readily adopted in the PICU, early adopters of different roles seized hold of various criterion and the learning healthcare environment created by AtriAmp. PICU RNs took more stock in the device’s simplicity and trialability, whereas the intensivists and cardiologists saw its relative advantage, compatibility with needs, and the results.
Our analysis suggests that AtriAmp could expand to standard of care in pediatric critical care units like our own. However, for technological innovations to be widely adopted amongst all PICUs, there are additional factors that must be considered and additional hurdles that may be faced[23, 24]. The additional factors are outlined in Figure 2, an adaptation of diffusion of innovation theory, more specifically for the adoption of new healthcare products and technologies. The stages of awareness, information gathering, and understanding technology remain the same, but the subsequent stages have been modified to reflect unique considerations. For example, compatibility with clinical needs, ease of use and training, and social influence are all important factors in adopting medical technologies in the PICU.
Additionally, trialability and piloting have been added as a stage to reflect the importance of testing the technology in this setting before making an adoption decision. Finally, the diagram includes the importance of continuous improvement as a final stage, as ongoing evaluation and refinement of the technology are critical for long-term success in the PICU context.
The additional hurdles are outlined in Tables 4 and 5, which list several lessons that were learned from two previously adopted and now widely used healthcare technologies, the electronic health record (EHR) and near-infrared spectroscopy (NIRS).[25–29] Other barriers to widespread adoption of AtriAmp could include the lack of established learning health system infrastructure, ambivalence toward adoption outside of academic centers, or variability in staffing across PICUs.
This study has several limitations.[30–32] Because our goal was to learn about the experiences of early adopters who are at the forefront of a new technology introduced into the PICU, we purposively recruited a total sample of individuals with the most experience with AtriAmp. Consequently, this is not a representative sample and likely does not reflect the practices of all multidisciplinary PICU teams. In contrast, the early adopters studied here reflect the small size and gendered division of our PICU. Among our early adopters, the pediatric intensivists were all were male, while the NPs and RNs were all female. Previous research has shown that new technologies can reproduce gender inequities that impact women’s participation and change in health systems[33]. This may be underrepresented in our study, where the sample reflects the current gender imbalance of many multidisciplinary teams and especially in PICU leadership[34]. Second, our results reflect self-reported practices. Because we did not observe the providers using AtriAmp, we do not know to what extent self-reported practice reflects actual practice where robust observational research is an important future direction.
Conclusions
The AtriAmp is an innovative tool that has the potential to significantly improve the management of arrhythmias following congenital cardiac surgery. The device provides valuable assistance in the management of postoperative arrhythmias, and it has the potential to significantly improve patient outcomes and enhance the quality of care in the pediatric ICU. Through qualitative research design, this study was able to identify how the AtriAmp fit into the PICU environment and why it is well set up for further dissemination in PICUs globally. Approximately 6 months after these interviews, the AtriAmp use became standard of care in these patients in our PICU. Since then, several additional PICUs and CICUs around the United States have begun experimenting with the device as well.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zimmerman JJ, Anand KJS, Meert KL, (2016) Research as a standard of care in PICU. Pediatr Crit Care Med 17:e 13–e 21. 10.1097/PCC.000000000000056226513203 PMC 5003779 · doi ↗ · pubmed ↗
- 2Gershengorn HB (2020) Early adoption of critical care interventions is unjustifiable without concomitant effectiveness study. Critical Care 24:649. 10.1186/s 13054-020-03382-833208179 PMC 7672161 · doi ↗ · pubmed ↗
- 3Drew BJ, Califf RM, Funk M, (2005) AHA Scientific Statement: Practice Standards for Electrocardiographic Monitoring in Hospital Settings. The Journal of Cardiovascular Nursing 20:76–106. 10.1097/00005082-200503000-0000315855856 · doi ↗ · pubmed ↗
- 4Bell L, Sargood T (2007) Atrial Electrograms After Cardiac Surgery. American Journal of Critical Care 16:360. 10.4037/ajcc 2007.16.4.36017595367 · doi ↗ · pubmed ↗
- 5Kern LS, Mc Rae ME, Funk M (2007) ECG Monitoring After Cardiac Surgery. AACN Advanced Critical Care 18:294–304. 10.4037/15597768-2007-300818019520 · doi ↗ · pubmed ↗
- 6Humes RA, Porter C-BJ, Puga FJ, (1989) Utility of Temporary Atrial Epicardial Electrodes in Postoperative Pediatric Cardiac Patients. Mayo Clinic Proceedings 64:516–521. 10.1016/S 0025-6196(12)65555-42725064 · doi ↗ · pubmed ↗
- 7Waldo AL, Maclean WA, Cooper TB, (1978) Use of temporarily placed epicardial atrial wire electrodes for the diagnosis and treatment of cardiac arrhythmias following open-heart surgery. J Thorac Cardiovasc Surg 76:500–505703357 · pubmed ↗
- 8Waldo AL, Henthorn RW, Plumb VJ (1984) Temporary epicardial wire electrodes in the diagnosis and treatment of arrhythmias after open heart surgery. The American Journal of Surgery 148:275–283. 10.1016/0002-9610(84)90237-X 6205603 · doi ↗ · pubmed ↗