Prevalence of Preterm Birth and Perinatal Outcomes in a Tertiary Hospital in Malaysia
Zahirrah Begam Mohamed Rasheed, Jesrine Hong, Hannuun Yaacob, Siti Zawiah Omar

TL;DR
This study examines preterm birth rates and outcomes at a Malaysian hospital from 2015 to 2019, finding inconsistent trends and high risks for preterm infants.
Contribution
The study provides new insights into preterm birth trends and perinatal outcomes in a Malaysian tertiary hospital over a five-year period.
Findings
Preterm birth rates decreased by 6% from 2015 to 2016 but showed inconsistent trends afterward.
Preterm infants born between 22+1 and 33+6 weeks had higher neonatal mortality risks compared to late preterm babies.
NICU admission and mortality rates were elevated for preterm infants with specific birth weights and delivery methods.
Abstract
Background Preterm birth (PTB) is defined as neonates that are born alive >22 weeks of gestation and <37 weeks of gestation. Because of the immaturity of different organ systems, 14.84 million newborns worldwide are born prematurely, which is the largest contributing factor to mortality and morbidity. Although studies have been conducted in this field, the magnitude of PTB is a major issue in most developing countries including Malaysia. Objective To assess the prevalence of PTB and the perinatal outcome among women delivered in a tertiary university hospital in Malaysia. Methods This was a cross-sectional study evaluating all singleton live births weighing>500g and delivered at >22+1 weeks of gestation between January 2015 and December 2019 in Universiti Malaya Medical Centre (UMMC), Kuala Lumpur, Malaysia. Data were collected from the hospital's recorded birth registry. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
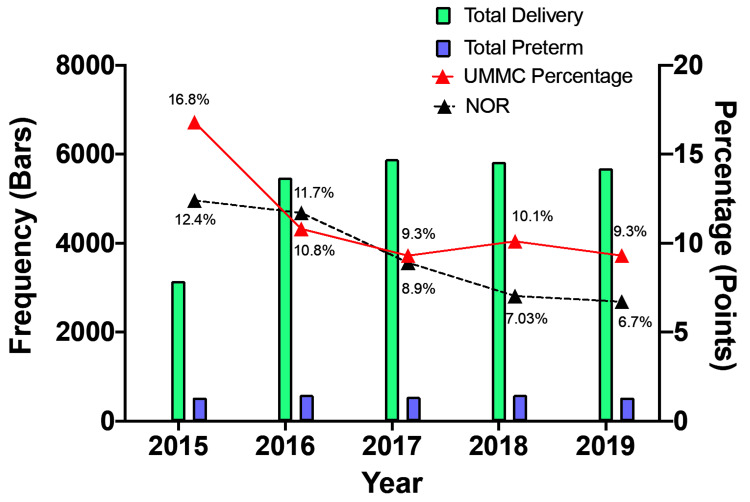 Figure 1
Figure 1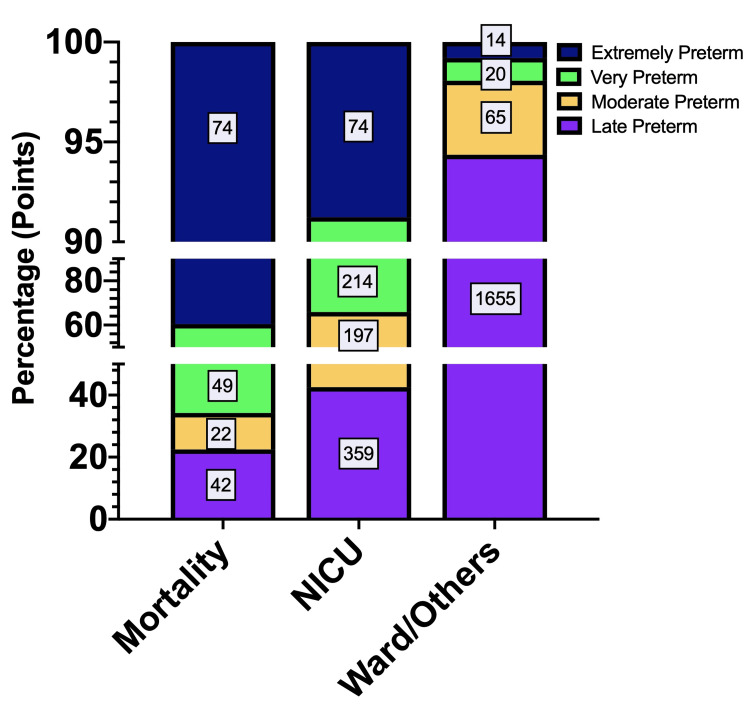 Figure 2
Figure 2| Variables | Category | Frequency (N) | Percentage (%) |
| Ethnicity | Malay | 1,635 | 58.7 |
| Chinese | 466 | 16.7 | |
| Indian | 357 | 12.8 | |
| Others | 327 | 11.7 | |
| Mode of delivery | SVD | 1,236 | 44.4 |
| Caesarean delivery | 1,338 | 48.0 | |
| aAssisted vaginal delivery | 142 | 5.1 | |
| bOthers | 69 | 2.5 | |
| Sex | Male | 1,524 | 54.7 |
| Female | 1,251 | 44.9 | |
| Ambiguous | 10 | 0.4 | |
| Birthweight | 500-2,000g | 886 | 31.8 |
| 2,001-3,000g | 1,560 | 56.0 | |
| 3,001-5,500g | 339 | 12.2 | |
| Baby’s postdelivery status | Neonatal mortality | 187 | 6.7 |
| NICU | 844 | 30.3 | |
| cWard/others | 1,754 | 63.0 | |
| Preterm severity | Extremely preterm | 162 | 5.8 |
| Very preterm | 283 | 10.2 | |
| Moderately preterm | 284 | 10.2 | |
| Late preterm | 2,056 | 73.8 |
| Perinatal Outcomes | Variables | B | Exp(B) | Sig. | 95% CI | ||
| Lower Bound | Upper Bound | ||||||
| NICU | Sex | <0.001 | |||||
| Boy | 2.484 | 11.995 | 0.004 | 2.197 | 65.490 | ||
| Girl | 2.267 | 9.651 | 0.009 | 1.769 | 52.647 | ||
| Undetermined* | - | - | - | - | - | ||
| Gestational age | <0.001 | ||||||
| Extremely preterm | -1.300 | 0.273 | <0.001 | 0.158 | 0.469 | ||
| Very preterm | -0.171 | 0.843 | 0.519 | 0.501 | 1.417 | ||
| Moderate preterm | 0.322 | 1.380 | 0.288 | 0.761 | 2.501 | ||
| Late preterm* | - | - | - | - | - | ||
| Mode of delivery | <0.001 | ||||||
| SVD | -0.054 | 0.948 | 0.905 | 0.394 | 2.278 | ||
| LSCS | 2.191 | 8.943 | <0.001 | 3.583 | 22.318 | ||
| Assisted device | 0.489 | 1.631 | 0.368 | 0.562 | 4.731 | ||
| Others* | - | - | - | - | - | ||
| Birthweight | <0.001 | ||||||
| <2 kg | 0.230 | 1.258 | 0.643 | 0.476 | 3.323 | ||
| 2-3 kg | 1.184 | 3.268 | 0.025 | 1.163 | 9.186 | ||
| 4-5.5 kg* | - | - | - | - | - | ||
| Ward/Others | Sex | <0.001 | |||||
| Boy | 1.237 | 3.444 | 0.267 | 0.387 | 30.621 | ||
| Girl | 1.431 | 4.182 | 0.199 | 0.471 | 37.172 | ||
| Undetermined* | - | - | - | - | - | ||
| Gestational age | <0.001 | ||||||
| Extremely preterm | -3.222 | 0.040 | <0.001 | 0.019 | 0.083 | ||
| Very preterm | -2.854 | 0.058 | <0.001 | 0.029 | 0.113 | ||
| Moderate preterm | -1.691 | 0.184 | <0.001 | 0.097 | 0.348 | ||
| Late preterm* | - | - | - | - | - | ||
| Mode of delivery | <0.001 | ||||||
| SVD | -0.0251 | 0.778 | 0.626 | 0.283 | 2.134 | ||
| LSCS | 0.752 | 2.122 | 0.158 | 0.747 | 6.027 | ||
| Assisted device | -0.0440 | 0.644 | 0.477 | 0.191 | 2.169 | ||
| Others* | - | - | - | - | - | ||
| Birthweight | <0.001 | ||||||
| <2 kg | -2.961 | 0.052 | <0.001 | 0.021 | 0.127 | ||
| 2-3 kg | 0.369 | 1.446 | 0.447 | 0.559 | 3.741 | ||
| 4-5.5 kg* | - | - | - | - | - | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Global Maternal and Child Health · Infant Development and Preterm Care
Introduction
Preterm birth (PTB) is defined as the birth of a live infant before 37 completed weeks of gestation [1]. Globally, around 15 million neonates are born preterm each year, with the worldwide PTB rate ranging from 4% to 16%, although this is higher in low- and middle-income countries [2]. As the leading cause of under-five mortality, PTB has been the focus of the World Health Organization (WHO) through the Sustainable Development Goals (SDG) and Millennium Development Goals (MDG). As pregnancy complications are related to various aetiologies and underlying factors, PTB can be divided into spontaneous or medically indicated PTB [3].
In Malaysia, both the public and private sectors provide maternity care from conception to delivery. In the public sector, the primary care level provides pre-conceptional and antenatal care services, through which screening-indicated high-risk mothers are referred to district or state hospitals for further management. According to National Obstetrics Registry (NOR) data, Malaysia demonstrated a decreasing birth incidence trend from 2016 to 2017 [4] and an increase from 2018 to 2020 [5]. These incidence data were captured from various hospitals nationwide.
A study by Sutan et al. on epidemiological PTB data from 2011 to 2015 revealed an increase in the PTB rate and risk factors associated with this outcome [6]. The data from the Sutan et al. study were gathered from a single-centred tertiary hospital that performs 15-20% of the overall in-vitro fertilisation procedures in Malaysia. These intriguing data demonstrate the importance of epidemiological studies involving various centred population research to identify the risk factors contributing to PTB, as well as the development of effective prevention interventions in the Malaysian population setting. Therefore, the current study provides evidence of the prevalence of PTB and neonatal outcomes of preterm infants born at Universiti Malaya Medical Centre (UMMC). UMMC is one of the main tertiary referral centres located in Kuala Lumpur and is a government-funded teaching hospital with an annual birth rate of between 4,000 and 5,000. Epidemiological data were gathered from the labour room admission records and the neonatal intensive care unit (NICU) admission records.
Materials and methods
Study design and setting
A hospital-based descriptive cross-sectional study was conducted using information obtained from delivery records between January 2015 and December 2019. The chosen centre was UMMC, a tertiary government-funded hospital with nearly 5,000 annual deliveries. It is located in Kuala Lumpur, a city with a total population of eight million. As a teaching hospital for Universiti Malaya (UM) and a provider of referral-level obstetrics and neonatal care services, UMCC is one of the busiest maternity centres and handles many high-risk pregnancies, including PTB.
Data collection
Data were collected once ethical approval was granted by the Medical Research Ethics Committee of UMMC (MREC ID: 20201124-9238). All mothers who had had single live births at UMMC from January 2015 until December 2019 were identified using birth registration records held at UMMC. The information collected included gestational age at delivery, ethnicity, mode of delivery, sex of the infant, birth weight, and postdelivery status of the infant. Gestational age was calculated using the date of the last menstrual period (LMP) and first-trimester dating scan [7]. Defined as a birth occurring at a gestation of less than 37 completed weeks, PTB was further characterised as extremely preterm (22+0-27+6 weeks), very preterm (28+0-31+6 weeks), moderately preterm (33+0-36+6 weeks), and late preterm (33+0-36+6 weeks) [3].
All singleton birth data were collected, although only live births above 22+0 weeks and above 500 grams were recorded. Any live births below 22+0 weeks of gestation and below 500 grams were considered miscarriages [8] and then excluded. Multiple-pregnancy data were also excluded. A total of 2,787 PTB cases were recorded, but two cases were dropped during the subsequent analysis as the mode of delivery and birth weight data were missing.
Data analysis
Data were entered into Excel sheets and cleaned before being analysed using Statistical Product and Service Solutions (SPSS) (IBM SPSS Statistics for Windows, Armonk, NY). Descriptive statistics, such as frequencies and percentages, were used to provide an overview of the variables. Additionally, visualisation in the form of bar charts will also be included to illustrate trends and distribution. Furthermore, multinomial logistic regression analysis was conducted owing to its framework, which allows for the simultaneous examination of the effects of multiple independent variables on a categorical dependent variable with three or more categories. Given the three categories within perinatal outcomes (i.e., mortality, admission to NICU, and admission to ward/others), multinomial logistic regression was particularly well-suited for understanding the relationship between perinatal outcomes and other variables. In this multinomial regression model, mortality was selected as the reference category for the dependent variable. The independent variables include gestational age at delivery, mode of delivery, sex of the infant, and birth weight. A significance level of p<0.05 was used to determine the statistical significance of the observed relationship within the regression model.
Results
Total deliveries and prevalence of preterm births (PTBs)
The bar chart in Figure 1 illustrates the trends in total deliveries and total singleton PTB between 2015 and 2019 at UMMC. Analysis of the total deliveries at UMMC shows a fluctuating trend over the five-year period. The lowest number of deliveries was reported in 2015 (N=3,155), followed by an increase in 2016 (N=5,476) and then a further increase in 2017 (N=5,885). Subsequently, stagnant total deliveries were observed in 2018 (N=5,823), with a slight decline in 2019 (N=5,683). Despite the irregular total deliveries trend over five years, the trend in PTB from singleton pregnancies is relatively consistent, with the highest frequency reported in 2018 (N=594). Additionally, Figure 1 illustrates the trend for the ratio of total deliveries to total PTB for UMMC and NOR in red and black, respectively. In 2015, it was found that UMMC recorded the highest PTB rate at 16.9%, while NOR had a rate of 12.4%. For UMMC, subsequent years show fluctuations, with rates ranging between 9% and 10% annually from 2016 to 2019. Conversely, the PTB rate for NOR shows a declining pattern from 2016 to 2019.
Total deliveries and singleton PTBs from 2015to 2019 at UMMC. The green bar charts represent the total deliveries in UMMC, and the blue bar charts are the total PTB in UMMC. The line charts are the PTB rates for UMMC and NOR in red and black, respectively.
Demographic characteristics of PTB
The descriptive statistics for the demographic, delivery characteristic, and neonatal outcome data collected from UMMC are presented in Table 1. Between 2015 and 2019, those of Malay ethnicity (N=1,635; 58.7%) recorded the most PTB cases at UMMC, followed by those of Chinese (N=466; 16.7%), Indian (N=357; 12.8%), and other ethnicities (N=327; 11.7%). The spontaneous vaginal delivery (SVD) rates were N=1,236; 44.4%, while caesarean delivery rates were N=1,338; 48.0%. In terms of the sex of the infant, a higher PTB rate was recorded among males (N=1,524; 54.7%) compared to females (N=1,251; 44.9%). Most neonates were born weighing between 2 kg and 3 kg (N=1,560; 56.0%), whereas 31.8% (N=886) of them were born weighing less than 2 kg. Over half of the preterm neonates were admitted for special care (N=1,754; 63.0%), while 30.3% (N=844) were admitted to the NICU and 6.7% (N=187) could not be revived after birth. A large number of the neonates were born at late preterm (N=2,056; 73.8%). However, extreme preterm (N=162; 5.8%) and very preterm (N=283; 10.2%) births collectively represented a higher rate compared to moderate PTB (N=284; 10.2%).
Neonatal outcomes
Stratifying the preterm severity categories into neonatal outcomes after delivery, 40% of neonatal mortality was observed in the extremely preterm group followed by 26.2% in the very preterm group. For the NICU category, late preterm neonates showed the highest admission rate at 42.5% compared to moderate preterm and very preterm neonates at 23% and 25%, respectively. Additionally, late preterm neonates also dominate the ward/others category with 94.4% compared to other preterm neonates (Figure 2).
Neonatal mortality, NICU-admitted, and ward-/other-admitted preterm neonates from 2015 to 2019. The preterm neonate outcomes were categorised based on the preterm severity.
Table 2 presents the results of multinominal logistic regression analysis examining the risk of neonates being admitted to the NICU and being admitted to the ward/others versus the reference category of neonatal mortality. All factors demonstrate statistical significance (p<0.001) indicating an association with prenatal outcomes. In the first part of the multinomial regression model, male infants (aOR: 11.995, CI: 2.197-65.490), caesarean deliveries (aOR: 8.943, CI: 3.583-22.318), and those with a birth weight of between 2 kg and 3 kg (aOR: 3.268, CI: 1.163-9.186) exhibited the greatest risk of being admitted to the NICU compared to facing the risk of neonatal mortality. However, contrasting results were observed for gestational age. Babies delivered between 22+1 and 27+6 weeks of gestation had a higher risk of mortality (aOR: 0.273, CI:0.158-0.469) instead of being at risk of admission to the NICU compared to late preterm neonates.
The second part of the multinomial regression model is the risk of being admitted to wards/others versus neonatal mortality. Female babies (aOR: 4.183, CI: 0.471-37.172), caesarean deliveries (aOR: 2.122, CI: 0.747-6.027, 22.318), and those with a birth weight between 2 kg and 3 kg (aOR: 1.446, CI: 0.559-3.741) displayed the highest risk of being admitted to the ward/others as compared to neonatal mortality. Other variables were more prone to mortality than to being admitted.
Discussion
PTB is rising in most countries, with the highest burden detected in low- and middle-income countries, especially those in sub-Saharan Africa and Southeast Asia [1]; therefore, Malaysia is included. The PTB prevalence in the centre examined in this study dropped by 6% between 2015 and 2016, with an inconsistent trend recorded from 2016 to 2019. The initial drop is consistent with the falling PTB trend reported by the National Obstetrics Registry (NOR) of Malaysia. The NOR also reported a 5.5% decrease in the number of live births between 2015 and 2016, which could explain the decrease in the PTB rate [4,9].
Of the middle-income countries, Malaysia’s PTB rate indicated that it experienced the lowest prevalence, compared to the rates of 13.6% in Indonesia [10], 24.3% in Egypt, 11.1% in Brazil [2], 16.0% in Nigeria [11], and 17.0% in South Africa [12]. Differences in the study context, method of gestational age assessment, sample size, and study population may have influenced the variations among the estimated prevalence of these countries. Additionally, factors such as inadequate infrastructure, technical equipment, and resources may also impede the provision of good-quality maternal care.
According to our data, babies of Malay ethnicity were more likely to be delivered prematurely. In contrast, the findings from NOR data revealed that those of Indian ethnicity preceded Malay and Chinese ethnicities in terms of the PTB distribution in Malaysia [13]. This evidence aligns with a study by Ruey et al., demonstrating that those of Indian ethnicity had a greater rate of higher-order pregnancies than the other races in Malaysia [14]. However, multiple pregnancies were not factored into this study, which would explain the disparity in ethnicity-related PTB. Nonetheless, there is mounting evidence to demonstrate a correlation between PTB and ethnicity in the United States [15], where the PTB risk associated with race is significantly higher among Black women compared to White women, based on a large systematic review [16]. Therefore, the diverse multiracial context of Malaysia is an area to be further explored.
The infants being male, mode of delivery, and birth weight were the most significant risk factors for perinatal outcomes. Previous studies have revealed that male infants have a greater risk of PTB and neonatal morbidity compared to females, who have been shown to have better health outcomes [6,17]. Many theories have been proposed to explain this connection, with several studies suggesting that the foetus's sex with the maternal hypothalamic-pituitary-adrenal axis affects foetal development and pregnancy outcomes [18]. Increased inflammatory reactions were also demonstrated in women carrying a male foetus [19], which could suggest the predisposing effect of a higher number of morbidity outcomes in male neonates who were granted further intensive care. Neonates being delivered by caesarean were also associated with an increased risk of NICU admission, with the same finding reported elsewhere [20]. Delivery by caesarean section is indicated when there is foetal compromise or when the maternal condition would detrimentally affect both the mother and foetus. Therefore, neonates are more likely to be admitted to the NICU for further specialised care [21].
Gestational age and birth weight are the most important factors in predicting the survival rates of premature infants [22] as they are more likely to experience complications. These complications are a significant factor in the direct cause of neonatal deaths, accounting for 35% of the world’s 3.1 million neonatal deaths per year [3]. A low gestational age means that the organs are immature and unprepared to support life in the extrauterine environment, thus increasing the risk of acute neonatal illnesses that would cause death [23], especially among extremely preterm and very preterm groups [24,25]. Compared to extremely preterm and very preterm infants, those of late preterm are more frequently admitted to the NICU, as seen in both this study and a recent review study [26]. As their birth weight and size are identical to those of term infants, late preterm infants are often overlooked because of their less mature physiology, limited response to the extrauterine environment, and higher risk of various morbidity, mortality, and adverse long-term outcomes [27]. Although Malaysia is demonstrating improved mortality rates because of advances in perinatal care [28], further efforts and research remain vital in reducing NICU admission and neonatal mortality rates among preterm infants.
Limitations
This study has several limitations. First, the results have a single-centre focus, but the authors believe that these data from a multi-ethnic population would be potentially generalisable to other low- and middle-income countries in the region. Misclassification of preterm severity was also possible because of the method of determining the gestational age [29]. The preterm cases reported at or referred to this hospital may not be similar to those of other tertiary hospitals as the UMMC is the main referral institution in Malaysia. Additionally, this study lacks an assessment of the comorbidities of the neonates to predict their survival, which could be added in future studies.
Conclusions
The incidence of PTB in a tertiary referral hospital in Malaysia from 2015 to 2019 fell from 2015 to 2016, but the trend was then stagnant until 2019. The highest PTB was observed in those of Malay ethnicity, while the sex of the infant, mode of delivery, and birth weight were the significant risk factors for adverse perinatal outcomes. More enhanced interventions are needed to reduce neonatal mortality and NICU admissions of preterm infants.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global burden of preterm birth Int J Gynaecol Obstet Walani SR 313315020203252459610.1002/ijgo.13195 · doi ↗ · pubmed ↗
- 2National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis Lancet Ohuma EO Moller AB Bradley E 1261127140220233780521710.1016/S 0140-6736(23)00878-4 · doi ↗ · pubmed ↗
- 3Born too soon: the global epidemiology of 15 million preterm births Reprod Health Blencowe H Cousens S Chou D 010 Suppl 1201310.1186/1742-4755-10-S 1-S 2PMC 382858524625129 · doi ↗ · pubmed ↗
- 4Small-for-gestational-age infants among uncomplicated pregnancies at term: a secondary analysis of 9 maternal-fetal medicine units network studies Am J Obstet Gynecol Mendez-Figueroa H Truong VT Pedroza C Khan AM Chauhan SP 628627215201610.1016/j.ajog.2016.06.04327372269 · doi ↗ · pubmed ↗
- 5Differential performance of first-trimester screening in predicting small-for-gestational-age neonate or fetal growth restriction Ultrasound Obstet Gynecol Crovetto F Triunfo S Crispi F Rodriguez-Sureda V Dominguez C Figueras F Gratacos E 3493564920172699023210.1002/uog.15919 · doi ↗ · pubmed ↗
- 6A 5 year trend and predictors of preterm births in single referral centre of the Greater Kuala Lumpur, Malaysia International Journal of Pregnancy and Child Birth Sutan R Mohamed NE Mahdy ZA 19620142018
- 7ISUOG practice guidelines: performance of first-trimester fetal ultrasound scan Ultrasound Obstet Gynecol Salomon LJ Alfirevic Z Bilardo CM 1021134120132328073910.1002/uog.12342 · doi ↗ · pubmed ↗
- 8Miscarriage Stat Pearls Dugas C Slane VH Treasure Island, FL Stat Pearls Publishing 2019 https://pubmed.ncbi.nlm.nih.gov/30422585/