Post-thyroidectomy Depression and Associated Factors in Saudi Arabia
Shaima A Althoubaiti, Amirah S Alharthi, Reham M Al Kahtani, Mayar A Algrni, Amal G Alshorm, Mohammad Eid M Mahfouz

TL;DR
This study finds that many Saudi patients experience depression after thyroid surgery, with factors like education level and surgery duration playing a role.
Contribution
The study identifies specific factors associated with post-thyroidectomy depression in Saudi Arabia.
Findings
80.92% of participants experienced depression after thyroidectomy, with mild and moderate cases being most common.
Females and those who had total thyroidectomy showed higher rates of depression symptoms.
Educational level and surgery time were significant predictors of post-surgery depression.
Abstract
Background Thyroidectomy is a common surgical procedure used to treat thyroid gland illnesses. The surgery has many outcomes, and one of them may show an association with depression. This study aims to assess the factors associated with depression after thyroidectomy in Saudi Arabia. Methodology A cross-sectional study was conducted among 414 Saudi participants. The target population included patients more than 18 years old and who had undergone thyroidectomy, whereas patients 18 years or younger were excluded. The data were collected between December 2023 and January 2024 using an electronic self-administered questionnaire that included demographics, clinical characteristics, and the nine-item Patient Health Questionnaire. The questionnaire was distributed randomly throughout social media, and patient consent was obtained. The descriptive and inferential analyses were performed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
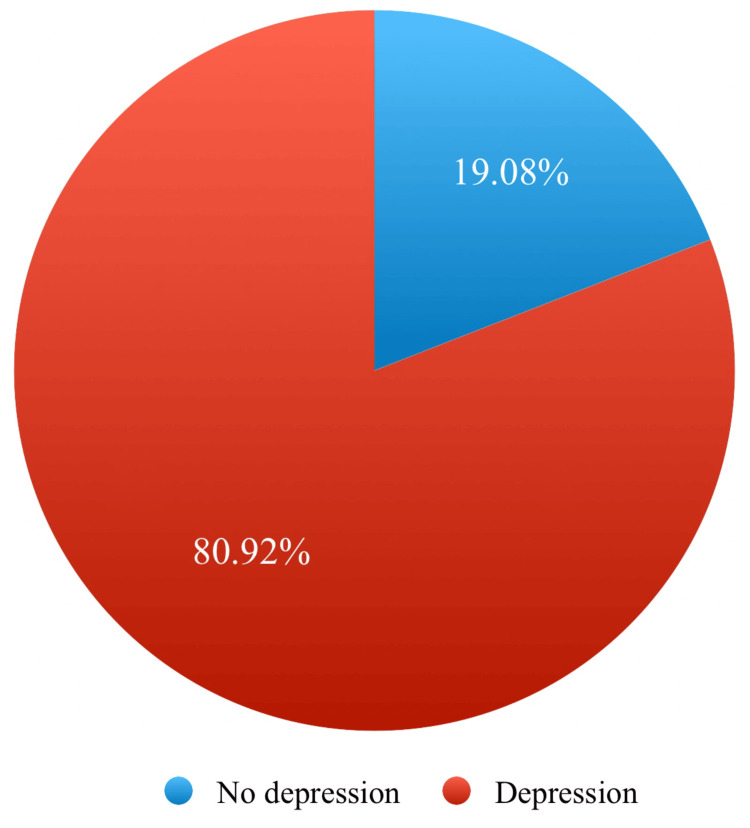 Figure 1
Figure 1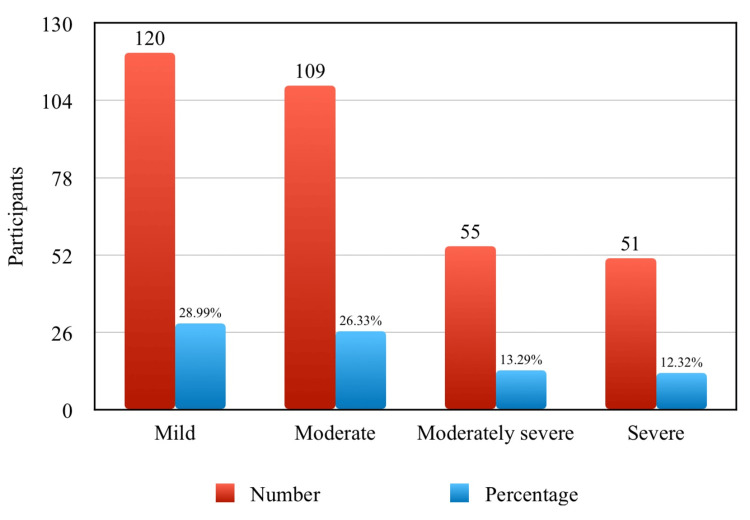 Figure 2
Figure 2| Characteristics | Categories | Frequency (n) | Percent (%) |
| Age (year) | 19–30 | 200 | 48.31% |
| 31–50 | 167 | 40.34% | |
| Above 50 | 47 | 11.35% | |
| Gender | Female | 306 | 73.91% |
| Male | 108 | 26.09% | |
| Regions | Western | 143 | 34.54% |
| Eastern | 74 | 17.87% | |
| South | 56 | 13.53% | |
| North | 34 | 8.21% | |
| Central | 107 | 25.85% | |
| Education | Less than high school education | 41 | 9.90% |
| High school education | 83 | 20.05% | |
| University education | 228 | 55.07% | |
| Postgraduate | 62 | 14.98% | |
| Area of work | Broker for securities and commodities | 10 | 2.42% |
| Environmental management and waste service | 2 | 0.48% | |
| Legal services | 22 | 5.31% | |
| Manufacturing and production | 11 | 2.66% | |
| Organization and association department | 10 | 2.42% | |
| Otherwise | 290 | 70.05% | |
| Personal services | 11 | 2.66% | |
| Public or private transportation | 16 | 3.86% | |
| Social service | 21 | 5.07% | |
| Real estate | 21 | 5.07% |
| Symptoms | Not at all, n (%) | Several days, n (%) | More than half the day, n (%) | Nearly every day, n (%) |
| Little interest or pleasure in doing things | 117 (28.26%) | 159 (38.41%) | 74 (17.87%) | 64 (15.46%) |
| Feeling down, depressed, or hopeless | 84 (20.29%) | 185 (44.69%) | 92 (22.22%) | 53 (12.80%) |
| Trouble falling or staying asleep, or sleeping too much | 88 (21.26%) | 131 (31.64%) | 106 (25.60%) | 89 (21.50%) |
| Feeling tired or having little energy | 70 (16.91%) | 126 (30.43%) | 114 (27.54%) | 104 (25.12) |
| Poor appetite or overeating | 109 (26.33%) | 140 (33.82%) | 81 (19.57%) | 84 (20.29%) |
| Feeling bad about yourself—or that you are a failure or have let yourself or your family down | 164 (39.61) | 120 (28.99%) | 59 (14.25%) | 71 (17.15%) |
| Trouble concentrating on things, such as reading the newspaper or watching television | 144 (34.78%) | 129 (31.16%) | 74 (17.87%) | 67 (16.18%) |
| Moving or speaking so slowly that other people could have noticed or the opposite—being so fidgety or restless that you have been moving around a lot more than usual | 196 (47.34%) | 111 (26.81%) | 58 (14.01%) | 49 (11.84%) |
| Thoughts that you would be better off dead or of hurting yourself in some way | 244 (58.94%) | 80 (19.32%) | 54 (13.04%) | 36 (8.70%) |
| Factors | Category | Depression status | P-value | |
| No depression, n (%) | Depression, n (%) | |||
| Age (year) | 19–30 | 43 (10.39%) | 157 (37.92%) | 0.493 |
| 31–50 | 28 (6.76%) | 139 (33.57%) | ||
| Over 50 | 8 (1.93%) | 39 (9.42%) | ||
| Gender | Female | 53 (12.80%) | 253 (61.11%) | 0.426 |
| Male | 26 (6.28%) | 82 (19.81%) | ||
| Region | Central region | 15 (3.62%) | 92 (22.22%) | 0.364 |
| Eastern province | 16 (3.86%) | 58 (14.00%) | ||
| Southern area | 12 (2.90%) | 44 (10.62%) | ||
| Northern area | 5 (1.21%) | 29 (7.00%) | ||
| Western region | 31 (7.49%) | 112 (27.05%) | ||
| Education | High school education | 14 (3.38%) | 69 (16.67%) | 0.009 |
| Less than secondary | 5 (1.21%) | 36 (8.70%) | ||
| Postgraduate | 13 (3.14%) | 49 (11.84%) | ||
| University education | 47 (11.35%) | 181 (43.72%) | ||
| Area of work | A broker for securities and commodities | 3 (0.72%) | 7 (1.69%) | 0.059 |
| Environmental management and waste service | 1 (0.24%) | 1 (0.24%) | ||
| Legal services | 6 (1.45%) | 16 (3.86%) | ||
| Manufacturing or production | 1 (0.24%) | 10 (2.42%) | ||
| Organization and associations department | 1 (0.24%) | 9 (2.17%) | ||
| Otherwise | 57 (13.77%) | 233 (46.28%) | ||
| Personal services | 11 (2.65%) | |||
| Public or private transportation | 4 (0.97%) | 12 (2.90%) | ||
| Real estate | 3 (0.72%) | 18 (4.35%) | ||
| Social service | 3 (0.72%) | 18 (4.35%) | ||
| Family history of depression | No | 49 (11.84%) | 135 (32.61%) | 0.325 |
| Yes | 30 (7.25%) | 200 (48.31%) | ||
| Factors | Category | Depression status | P-value | |
| No depression, n (%) | Depression, n (%) | |||
| Type of disease | Benign reasons | 66 (15.94%) | 224 (54.11%) | 0.168 |
| Malignant causes | 13 (3.14%) | 111 (26.81%) | ||
| Type of surgery | Complete thyroidectomy | 40 (9.66%) | 177 (42.75%) | 0.231 |
| Excision of a part of the thyroid gland | 39 (9.42%) | 158 (38.16%) | ||
| Surgery time | 4 months ago | 18 (4.35%) | 39 (9.42%) | 0.021 |
| After 6 months to a year | 9 (2.17%) | 36 (8.70%) | ||
| From 4 to 6 months | 5 (1.21%) | 38 (9.18%) | ||
| From 1 to 2 years | 8 (1.93%) | 71 (17.15%) | ||
| More than 2 years | 39 (9.42%) | 151 (36.47%) | ||
| Complication | Yes | 24 (5.80%) | 216 (52.17%) | 0.26 |
| No | 55 (13.29%) | 119 (28.74%) | ||
| Duration of complications | Ongoing | 10 (2.42%) | 97 (23.43%) | 0.055 |
| Temporary | 16 (3.86%) | 147 (35.51%) | ||
| No complications | 53 (12.80%) | 91 (21.98%) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid and Parathyroid Surgery · Thyroid Cancer Diagnosis and Treatment
Introduction
Thyroidectomy is a well-known procedure that removes the whole thyroid gland or a part of the gland in cases of thyroid illness that do not respond to medical treatment [1]. The thyroid gland has the following three components: the isthmus, which connects the two lobes below the cricoid cartilage; and the right and left lobes, which are located anterolateral to the larynx and trachea [2]. Therefore, thyroidectomy has many types, namely, total thyroidectomy (removal of all thyroid tissue), lobectomy (removing an entire lobe), and subtotal thyroidectomy (removing the gland and leaving >1 g of thyroid gland tissue) [1]. Nowadays, total thyroidectomy is the most common surgical procedure used to treat thyroid conditions [3].
Thyroidectomy can be indicated in both benign and malignant conditions such as thyroid cancer, thyroid nodules, Graves’ disease, and goiter with compression symptoms [4]. The complications of thyroidectomy can be transient, such as hypocalcemia, hoarseness, hematoma, and infection, or can be permanent, such as hypothyroidism, hypoparathyroidism, and unilateral vocal cord paralysis [5]. Hypocalcemia is a common and serious complication of total thyroidectomy, whereas hypothyroidism is seen as an expected outcome [6,7].
The outcome of thyroidectomy can be influenced by the type of surgery performed and the surgeon’s experience, with a more skilled surgeon linked to a better outcome, and total thyroid removal is associated with a higher risk of complication [8,9]. The quality of life after a thyroidectomy significantly improves compared to before the procedure [10]. According to statistics, patients may experience some psychological symptoms, such as depression, anxiety, and other issues, that could negatively impact their quality of life, especially within the first year after surgery [11,12].
Due to limited data in this field, in this study, we aim to highlight the assessment of the factors associated with depression after thyroidectomy in Saudi Arabia.
Materials and methods
Study design, setting, and participants
This observational, cross-sectional study was conducted among 414 people to assess the prevalence of depression after thyroidectomy and the associated factors in the Saudi Arabian population from December 2023 to January 2024. The target population included patients aged more than 18 years who had undergone thyroidectomy, either or total removal of the gland, whereas patients 18 years of age or younger who had not undergone thyroidectomy were excluded.
Sample size
We calculated the sample size using the following formula: n = z^2^ p(1-p)/M^2^, where n is the number of samples, z is the level of confidence (95%), P is the population proportion (50%), and M is the margin of error (0.05). The calculated sample was 384, but we increased the sample size to 414, for more representation and to improve the accuracy and reliability of the study findings.
Data collection
An electronic, self-administered Arabic online questionnaire was developed using Google Forms. To ensure a diverse representation of participants from various regions, the questionnaire was randomly distributed through social media platforms such as Telegram and WhatsApp. The questionnaire was developed after conducting extensive literature reviews by researchers and doctor consultations and comprised the following three parts: the first part contained informed consent and demographic data (age, gender, region, educational level, occupation); the second focused on clinical factors (family history of depression, type of disease, type of surgery, time of surgery, complications, duration of complications); and the third part was a self-administered depression assessment scale known as the nine-item Patient Health Questionnaire (PHQ-9), which consists of nine questions designed to screen for depression symptoms. Each question is scored from 0 (not at all) to 3 (nearly every day), with a minimum score of 0 to a maximum score of 27; a higher score indicates more severe symptoms. We used the Arabic version [13].
Data analysis
The data were entered into Microsoft Excel 2019 (Microsoft Corp., Redmond, WA, USA), and then the data were analyzed using SPSS software version 27(IBM Corp., Armonk, NY, USA). Frequency and percentages were used to demonstrate categorical variables. Continuous variables were presented using the mean and standard deviation. To test for the presence of an association between categorical variables, a chi-square test was utilized, and the statistical significance level was set at 5%.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee of Taif University (application number: 45-087). Consent was obtained electronically from all participants after we explained the study’s aim. Confidentiality measures such as strict access to researchers only and anonymity were implemented for all collected data to ensure the privacy and confidentiality of participants’ information.
Results
Demographic characteristics
A total of 414 participants were included in this study. Regarding age, most participants (48.31%) were between the ages of 19 and 30 years. Regarding gender, 73.91% of participants were female, while 26.09% were male. The participants were from various regions, with the highest percentage (34.54%) from the Western region and the lowest percentage (8.21%) from the North region. For educational level, the majority of participants (55.07%) had a university education. Regarding the area of work, the largest group (70.05%) consisted of participants who worked in various other fields not specified (Table 1).
Patient health survey
Table 2 shows the detailed assessment of participants’ depression based on the PHQ-9. Some of the most common items were feeling tired or having little energy (83.81%), feeling down or hopeless (79.71), having trouble falling or staying asleep, or sleeping too much (78.74).
Prevalence of depression
Based on the results of the PHQ-9 survey, a significant proportion of patients experienced depression after thyroid surgery (Figure 1).
Prevalence of depression among study participants (N = 414).
Prevalence of depression severity
Most participants suffering from depression had a mild degree (28.99%), while a severe degree of depression was observed in only 12.32% (Figure 2).
Depression severity among study participants (N = 414).
Associations between different demographic factors and depression status
Education level was the only factor that showed a significant difference in depression after thyroid surgery. On the other hand, the area of work and a family history of depression showed no significant difference in depression status (Table 3).
Associations between different clinical factors and depression status
Surgery time was the only factor that showed a significant difference in depression after thyroid surgery. On the other hand, type of disease, type of surgery, and complications showed no significant difference in depression status (Table 4).
Discussion
Thyroidectomy is one of the most common procedures worldwide, and one of its consequences is the risk of developing postoperative depression symptoms. A few studies have been conducted to determine the prevalence of post-thyroidectomy depression. One study from South Korea showed a low prevalence, while our study showed a higher prevalence. This could be because we screened patients according to the PHQ-9 and we covered depression status from mild to severe symptoms, while the other study investigated patients for major depressive disorder diagnosed by psychiatrists [11].
Most study participants who underwent thyroidectomy were female and had more severe depression symptoms than males, which may be due to the higher prevalence of thyroid diseases in females than males, similar to this study which showed a higher prevalence of thyroid disease in females [14].
The majority of participants who showed depression symptoms had a higher educational level, which could be explained as having a higher education exposes individuals to more stress and workload leading to depression. In contrast, a cohort study showed that a higher educational level was linked with low depression symptoms [15].
Our study revealed that post-thyroidectomy depression was more common in benign disease, in contrast to another study that found post-thyroidectomy depression was more common in thyroid cancer patients. The fact that our study included both benign and malignant diseases, while the other study only included malignant and a control group could account for the discrepancy [16].
Most participants with depression symptoms had undergone a total thyroidectomy, and, to our knowledge, this can lead to hypothyroidism as thyroid hormone has a significant impact on mental health, unlike in a partial thyroidectomy, where the remaining part mostly compensates for the deficit and has a lower risk of developing depression. Similar findings were noted in a previous study [17].
We found that the prevalence of depression increased gradually after two years of thyroidectomy. Unlike another study that showed the risk reaching up to one year postoperatively, perhaps the distinction between the two studies was that our study was applied to all of our participants who have postoperative depression, whereas the other study assessed a particular group of young adults, females, urban residents, and low-income groups [16].
A substantial number of participants had temporary complications and showed depression. Another previous analytical study showed a higher rate of temporary complications than permanent complications, which could depend on patient factors, surgeon experience, and hospital facilities [18].
Limitations
This was the first study to be conducted in Saudi Arabia and highlights major public health issues such as depression after a common surgery. The study was performed using online questionnaires rather than interviews in hospitals due to the difficulty of hospital access and setup across Saudi Arabia. However, this allowed for the coverage of a larger geographic area. In addition, we also recruited a medium-sized sample as we wanted our data to be as accurate as possible and limited to people who underwent thyroidectomy.
Conclusions
A significant prevalence of depression was noted among patients undergoing thyroidectomy, which was mostly mild. In addition, most participants were female and had more severe symptoms than males. Furthermore, total thyroidectomy had a higher prevalence of depression than partial thyroidectomy.
The associated factors, such as the educational level, showed more depression symptoms with a high educational level. The risk of developing depression persisted beyond two years after surgery. We recommend regular follow-ups with a psychiatrist for those who underwent thyroidectomy for early detection of depression and timely management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1European perspective on 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: proceedings of an interactive international symposium Thyroid Luster M Aktolun C Amendoeira I 7262920193048439410.1089/thy.2017.0129 · doi ↗ · pubmed ↗
- 2Surgical management of thyroid and parathyroid disorders Med Clin North Am Miller FR Netterville JL 2470247-59, xi 831999992797310.1016/s 0025-7125(05)70100-0 · doi ↗ · pubmed ↗
- 3Total thyroidectomy for the treatment of thyroid diseases in an endemic area South Med J Misiakos EP Liakakos T Macheras A Zachaki A Kakaviatos N Karatzas G 122412299920061719541710.1097/01.smj.0000232202.82002.c 5 · doi ↗ · pubmed ↗
- 4Thyroidectomy Biello A Kinberg EC Wirtz ED Treasure Island, FL Stat Pearls Publishing 2024 https://pubmed.ncbi.nlm.nih.gov/33085426/33085426 · pubmed ↗
- 5Factors influencing thyroidectomy complications Braz J Otorhinolaryngol Ernandes-Neto M Tagliarini JV López BE Padovani CR Marques Mde A Castilho EC Mazeto GM 636978201210.1590/S 1808-86942012000300012 PMC 944622922714849 · doi ↗ · pubmed ↗
- 6Complications of thyroid surgery: analysis of a multicentric study on 14,934 patients operated on in Italy over 5 years World J Surg Rosato L Avenia N Bernante P 2712762820041496120410.1007/s 00268-003-6903-1 · doi ↗ · pubmed ↗
- 7Hypocalcemia following thyroid surgery: incidence and prediction of outcome World J Surg Pattou F Combemale F Fabre S 718724221998960628810.1007/s 002689900459 · doi ↗ · pubmed ↗
- 8Total thyroidectomy is associated with increased risk of complications for low- and high-volume surgeons Ann Surg Oncol Hauch A Al-Qurayshi Z Randolph G Kandil E 384438522120142494323610.1245/s 10434-014-3846-8 · doi ↗ · pubmed ↗