Outcomes of Minimally Invasive Adrenalectomy for Large Adrenal Masses: A Multi-Centre Experience in Saudi Arabia
Raed A. Azhar, Omar Buksh, Abdullah M Almalki, Rabea Akram, Hani Alzahrani, Abdullah Al-Gadheeb, Qusay Mandoorah, Adel A Alammari

TL;DR
This study shows that minimally invasive surgery can safely remove large adrenal tumors in Saudi patients, with good outcomes compared to traditional open surgery.
Contribution
The paper provides real-world evidence from Saudi Arabia demonstrating the safety and efficacy of minimally invasive adrenalectomy for large adrenal masses.
Findings
Minimally invasive adrenalectomy was successfully used for adrenal masses up to 21 cm in size.
Robotic surgery had lower blood loss and shorter hospital stays compared to laparoscopic surgery.
No disease recurrence was observed in patients during a mean follow-up of 58 months.
Abstract
Introduction Advancements in radiological imaging technology have increased the discovery of adrenal incidentalomas. Large adrenal tumors (LATs) are not common, and the likelihood of malignancy increases with tumor size. LATs were defined as tumors larger than four centimeters (cm) with various pathologic diagnoses. Traditionally, open adrenalectomy was considered the gold standard for LATs, but with recent advancements in minimally invasive surgery (MIS), optimum perioperative and long-term outcomes are achievable by the MIS approach. The findings presented in this paper show that even large adrenal masses measuring up to 21 centimeters can be safely removed using a minimally invasive approach. Methodology After Institutional Review Board (IRB) approval, we reviewed medical records of adult patients who had adrenalectomies at two Saudi Arabian centers from January 2013 to February…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
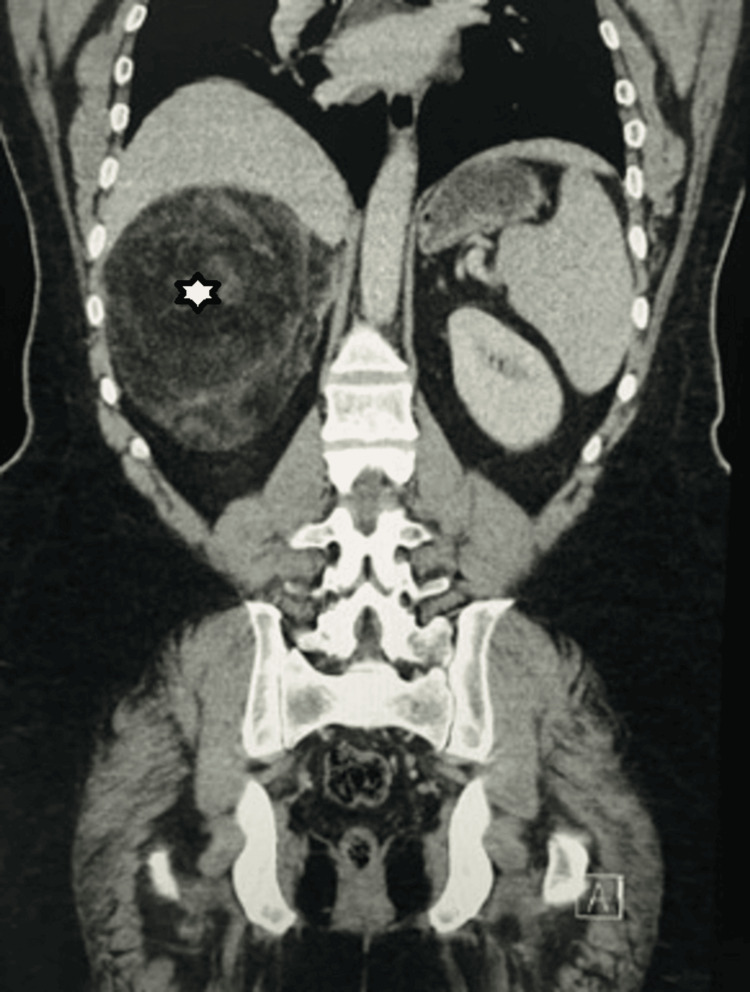 Figure 1
Figure 1 Figure 2
Figure 2| Variable | Value |
| Sex: (n) (%): | |
| Males | Males = 15 (42.5%) |
| Females | Females = 20 (57.1%) |
| Mean age in years ± Standard deviation | 41.7 ± 14.9 |
| Mean weight in kilograms ± Standard deviation | 88.1 ± 40.5 |
| Mean height in centimeters ± Standard deviation | 148.1 ± 34.2 |
| Mean body mass index in kilograms/m2 ± Standard deviation | 26.9 ± 6 |
| Mean tumor size in centimeters ± Standard deviation | 8 ± 4.6 |
| Comorbidity (n) (%): | |
| Hypertension | 15 (42.9%) |
| Diabetes | 4 (11.4%) |
| Smokers (n) (%) | 0 (0%) |
| Past history of malignancy (n) (%) | 5 (12.5%) |
| History of cardiovascular disease (n) (%) | 2 (5%) |
| Hypertensive/hypotensive crises | 0 |
| Presentation (n) (%): | |
| Incidental | 15 (42.9%) |
| Hypertension | 6 (17.1%) |
| Adrenal gland disorder | 4 (11.4%) |
| Flank pain | 4 (11.4%) |
| Palpitation | 3 (6.6%) |
| Other | 3 (8.6%) |
| Involvement (n) (%): | |
| Left | 14 (40%) |
| Right | 17 (48.6%) |
| Bilateral | 4 (11.4%) |
| Endocrine Functioning status (n) (%): | |
| Functional | 13 (37.1%) |
| Nonfunctional | 22 (62.9%) |
| Procedure (n) (%): | |
| Unilateral laparoscopy | 25 (62.5%) |
| Bilateral laparoscopy | 4 (10%) |
| Robotic | 6 (15%) |
| Final diagnosis (n) (%): | |
| Myolipoma | 8 (22.9%) |
| Adenoma | 8 (22.9%) |
| Pheochromocytoma | 6 (17.1%) |
| Metastatic lesion | 3 (8.6%) |
| Cyst | 2 (5.7%) |
| Benign lesion | 3 (8.6%) |
| Other | 5 (14.3%) |
| Variable | Unilateral Lap | Bilateral Lap | Robotic | p-value |
| Operative room time in minutes ± Standard deviation | 202.3 ± 96.0 | 321 ± 64 | 183.3 ± 10.3 | 0.03 |
| Estimated blood loss in milliliters ± Standard deviation | 214 ± 386.3 | 76.3 ± 33 | 80 ± 34.6 | 0.58 |
| Length of stay in days ± Standard deviation | 9.4 ± 6.3 | 6.5 ± 3.8 | 5.5 ± 1.9 | 0.21 |
| Variable | Tumor size < 7 cm | Tumor size > 7 cm | p-value |
| Operative room time in minutes ± Standard deviation | 197.5 ± 79.3 | 241.3 ± 105.1 | 0.17 |
| Estimated blood loss in milliliters ± Standard deviation | 130.9 ± 238.1 | 238.1 ± 430.5 | 0.35 |
| Length of stay in days ± Standard deviation | 8.1 ± 6.1 | 10.1 ± 6.7 | 0.38 |
| Variable | Left | Right | Bilateral | p-value |
| Operative room time in minutes ± Standard deviation | 202.2 ± 81 | 198 ± 90.4 | 321 ± 64.0 | 0.03 |
| Estimated blood loss in millileters ± Standard deviation | 98.9 ± 131.6 | 251.8 ± 442.9 | 76.3 ± 33 | 0.36 |
| Length of stay in days ± Standard deviation | 10.6 ± 8.2 | 7.9 ± 4.7 | 6.5 ± 3.9 | 0.37 |
| Author | Year of publication | Surgical technique | Number of patients | Mean age in years ± Standard deviation | Gender (Male/Female) (n) | Laterality (Right/Left/Bilateral) (n) | Mean Body mass index in Kg/m2 ± Standard deviation | Mean size in centimeters ± Standard deviation | Estimated blood loss in milliliters ± Standard deviation | Operation room time in minutes ± Standard deviation | Conversion to open (n) | Length of stay in days ± Standard deviation |
| Hobart et al., [ | 2000 | Laparoscopy | 14 | 57.1 | 6/8 | 8/6/0 | 31.4 | 8 | 400 | 205 | 2 | 2.4 |
| Henry et al., [ | 2002 | laparoscopy | 19 | 57.3 | 4/15 | 10/9/0 | Not mentioned | 7.1 | Not mentioned | 150 | 2 | Not mentioned |
| Naya et al., [ | 2005 | Laparoscopy | 16 | 48.1 ± 15.6 | 12/4 | 5/11/0 | 24.1 ± 3.2 | Not mentioned | 212 ± 165 | 175 ± 82 | 0 | Not mentioned |
| Bhat et al., [ | 2007 | Laparoscopy | 10 | 42.8 ± 10.65 | 5/5 | 4/5/1 | Not mentioned | 8 cm ± 1.47 | 116.5 | 157 | 2 | 4.1 |
| Agcaoglu et al., [ | 2012 | Laparoscopy | 38 | 52.5 ± 2.3 | 18/20 | 13/25/0 | 30.2 ± 0.9 | 6.2 ± 0.3 | 166.6 ± 51.2 | 187.2 ± 8.3 | 4 | 1.9 ± 0.1 |
| Robotic surgery | 24 | 52.4 ± 2.9 | 10/14 | 9/16/0 | 27.1 ± 0.8 | 6.5 ± 0.4 | 83.6 ± 59.4 | 159.4 (± 13.4) | 1 | 1.4 ± 0.2 | ||
| Ragavan et al., [ | 2020 | Robotic surgery | 38 | 46.5 ± 11.3 | 21/17 | 22/16/0 | Not mentioned | 5.94 ± 3.2 | 54.4 ± 16.8 | 89.6 ± 8.1 | 0 | 2.7 ± 2.0 |
| Our study | 2023 | Laparoscopy | 29 | 42.5 ± 16.2 | 12/17 | 12/13/4 | 27.5 ± 6.3 | 7.8 ± 4.4 | 189.3 ± 354.6 | 220.1 ± 98.7 | 1 | 9.5 ± 6.7 |
| Robotic Surgery | 6 | 38.0 ± 3.5 | 3/3 | 5/1 | 24.0 ± 2.4 | 8.9 ± 6.2 | 80.0 ± 34.6 | 188.3 ± 10.3 | 0 | 5.5 ± 1.9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStructural Analysis of Composite Materials · Architecture and Computational Design · Hygrothermal properties of building materials
Introduction
Due to recent advancements in imaging technology, there has been an increase in the discovery of adrenal incidentalomas. However, large adrenal tumors (LATs) are not common, the incidence of which ranges from 8.6% to 38.6% [1-2]. The likelihood of malignancy increases with increasing tumor size [3-4]. It is crucial to accurately assess the nature and origin of LATs before surgery to determine the appropriate surgical approach [5-6]. LATs are defined as tumors >5-10cm in diameter, with a consensus of ~5cm [7-8].
Ever since Gagner et al. first introduced the concept in 1991, the minimally invasive surgery (MIS) approach for treating various adrenal lesions has gained significant popularity [9]. In comparison to the traditional open surgical technique, laparoscopic adrenalectomy has been shown to have reduced perioperative complications and mortality rates, along with shorter hospital stays and improved cosmetic outcomes. This has led to an increasing preference for the MIS approach among surgeons and patients alike.
Typically, due to concerns about incomplete resection and the possibility of local invasion, an open surgical approach is recommended for LATs [10]. In addition, the MIS approach for large adrenal masses has not gained worldwide acceptance for adrenalectomy due to its drawbacks, such as higher cost and limited accessibility. Nevertheless, the current standard of care favors an open approach for tumors larger than five cm, as minimally invasive procedures are considered contraindicated in such cases. Gryn et al. found that tumors >5cm in size are associated with unfavorable surgical outcomes, positive margins, and complications [10]. However, with rapid improvements in MIS techniques such as robotic and laparoscopic approaches, LATs are being increasingly resected using MIS, with acceptable and safe outcomes [8].
In this paper, we demonstrate our experience with using MIS as a surgical approach for large adrenal masses, and that even LATs reaching 21 cm can be safely resected with the MIS approach with acceptable blood loss, length of stay (LOS), operative room time (ORT), and optimum oncological outcomes.
Materials and methods
Following the approval from the Institutional Review Board (IRB) (Approval number: 2021-02), we conducted a retrospective review of the medical records of adult patients who underwent adrenalectomies at two tertiary centers in Saudi Arabia (in King Faisal Specialist Hospital and Research Centre Jeddah and King Abdulaziz University Hospital Jeddah) between the period January 1, 2013, and February 30, 2023. Our inclusion criteria consisted of adult patients over the age of 18, who underwent laparoscopic or robotic adrenalectomy, for adrenal lesions measuring five centimeters or more. Pediatric patients and those who underwent open adrenalectomies were excluded from the study. Thirty-five patients met the inclusion criteria.
Prior to surgery, all patients underwent various imaging studies, including ultrasound, abdominal cross-sectional (CT) scan, magnetic resonance imaging (MRI), and metaiodobenzylguanidine (MIBG) scintigraphy for suspected adrenal pheochromocytoma, to assess the location, size, and functional characteristics of the mass. Functional masses were identified through serum levels of aldosterone and cortisol, as well as urinary levels of metanephrines. Patients diagnosed with pheochromocytoma received a two-week treatment with oral adrenergic blockers, and intraoperative monitoring was performed to ensure hemodynamic stability. We thoroughly examined the perioperative data of the patients, which encompassed factors such as age, gender, body mass index (BMI), comorbidities, smoking status, history of malignancy, presentation of the mass, functionality of the mass, size and laterality of the mass, pathology of the mass, modality of surgery, operative time, blood loss and if blood transfusion was required intra-operatively or postoperatively, intra-operative complications, length of hospital stay, duration of follow-up, and recurrence rates. The data was collected and then analyzed using SPSS-23 (IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.), with a p-value of less than 0.05 considered statistically significant. All patients provided informed consent for the surgeries after a comprehensive explanation of the associated risks and benefits. Follow-up appointments were scheduled for patients diagnosed with malignant disease at 3, 6, and 12 months post-surgery, during which cross-sectional (CT) scans were conducted. Annual CT scans of the chest, abdomen, and pelvis were done afterward yearly for a presumed follow-up period of 60 months.
Results
The final study included a total of 35 patients, out of which 29 underwent laparoscopic surgery while six underwent robotic surgery. The mean age of those who underwent laparoscopic surgery was higher than those who underwent robotic surgery (p=0.5). The majority of laparoscopic cases were females, while the gender ratio was equal in robotic cases. The body mass index (BMI) of laparoscopic cases was higher but without statistical significance. None of the patients in the robotic surgery group were diabetic. The operation room time (ORT), estimated blood loss (EBL), and length of stay in the hospital (LOS) were all noted to be higher for laparoscopic cases than robotic cases but without statistical significance. Mean tumor size was higher in the robotic technique, with a mean size of 8.9± 6.2 cm but without statistical significance, with the largest tumor size of 21 cm. Details of the baseline demographics have been depicted in (Table 1).
Analysis of the means of the operative variables revealed that robotic procedures had the shortest time in the operation room (ORT) at 183.3±10.3 minutes, while bilateral laparoscopic procedures had the longest at 321±64 minutes. This difference in ORT was statistically significant (p=0.03). Unilateral laparoscopic surgeries had the highest mean blood loss at 214±386.3 ml, while both robotic and bilateral laparoscopic procedures had a lower mean blood loss. Bilateral laparoscopies had a slightly lower mean blood loss (76.3±33 ml) compared to robotic surgeries (80±34.6 ml), but this difference was not statistically significant (p=0.58). Robotic surgeries had the shortest mean hospital stay at 5.5±1.9 days, while unilateral laparoscopic surgeries had the longest mean hospital stay at 9.4±6.3 days. However, these differences were not statistically significant (p=0.25). Details of the comparison drawn between the operative and post-operative variables have been depicted in (Table 2).
Table 2: A comparison of the means of operative and post-operative variables based on surgical technique using the one-way ANOVA test P-value < 0.05 is considered as significant.
In terms of complications, the overall recurrence rate was low, with a peri-operative complication being reported in two cases only, which was in the unilateral laparoscopy group. A similar trend was noted in the same arm for conversion to open surgery due to aortic injury. With regards to cases needing blood transfusions, nine cases of unilateral laparoscopy required blood transfusions. The mean follow up period was 58 months, with a range from one to five years, and none of the 35 patients included in the study experienced any recurrence of their adrenal disease. When the data was sub-grouped and analyzed based on tumor size greater than or less than seven cm in the greatest dimension, results showed that all parameters (mean ORT, EBL, and LOS) were lower for tumor size <7 cm but without statistical significance. Further details on the data are in (Table 3).
Table 3: A comparison of the means of operative and post-operative variables based on tumor size using the One-way ANOVA test P-value < 0.05 is considered as significant.
When the data was sub-grouped and analyzed based on site of tumor, results showed that ORT was the lowest for right-sided tumors and highest for bilateral tumors; these findings were statistically significant (p=0.03). Interestingly, EBL was highest for right sided tumors and lowest for bilateral tumors but without statistical significance. Another peculiar finding was that LOS was lowest for bilateral tumors and highest for left sided tumors, but again without statistical significance. Further details are demonstrated in Table 4.
Table 4: A comparison of the means of operative and post-operative variables based on laterality of tumor using the One-way ANOVA test P-value < 0.05 is considered as significant.
Discussion
Adrenal tumors are frequently discovered incidentally during abdominal radiology scans, particularly in older individuals [11]. The size of the tumor can serve as an indicator of its potential malignancy, with larger tumors having a higher likelihood of being cancerous. However, linking the size with the likelihood of malignancy is not always simple. Numerous studies involving a significant number of patients with adrenal tumors have demonstrated that around 10% or less of these cases are malignant [12,13]. As a result, opting for an open surgical approach for large adrenal tumors and reserving minimally invasive surgery for smaller masses may not always be the optimal choice.
From our perspective, it is crucial to possess expertise in laparoscopic adrenal surgery and proficiency in robotic procedures to effectively avoid complications. Various studies have documented that the reasons for converting from robotic surgery to laparoscopic or open adrenalectomy include visceral injury, challenges in achieving hemostasis, incorrect placement of robotic trocars, and prolonged duration of the operation [14]. These factors highlight the significance of having experience and skill in both laparoscopic and robotic techniques to minimize the likelihood of encountering such complications. In our study, only one case converted from laparoscopic to open surgery, which was due to aortic injury.
A literature review examined the use of minimally invasive surgery (MIS) for adrenalectomies, and six studies were analyzed [15-20] (Table 5). Four studies used laparoscopy exclusively [15-18], one used both laparoscopy and robotic techniques [19], and one used robotic surgery exclusively [20]. The number of patients in each study varied from 10 to 52, with an average age range of 42.8 to 57 years. Most studies had a similar male-to-female ratio. Tumor laterality differed among the studies. The average BMI ranged from 24.1 Kg/m2 to 31.1 Kg/m2, and the mean tumor size ranged from 5.94cm to 8cm. EBL during surgery ranged from 54.4ml to 400ml, and OR time ranged from 89.6 minutes to 205 minutes. Across all studies, eleven patients required conversion to open surgery, and LOS in the hospital ranged from 1.4 days to 4.1 days. A quick comparison between our results with the data above shows that the data obtained from previous studies aligns closely with our results, suggesting that the MIS approach can be considered a safe method for resecting LATs. The similarity between the two sets of data highlights the reliability and consistency of our findings, further supporting the notion that MIS can be a viable option for the resection of LATs.
A variety of pathological types are observed in LATs. Therefore, when diagnosing LATs clinically, it is important to consider the possibility of benign tumors first. However, there is still a significant chance that a LAT could be malignant. Previous research found that benign LATs made up 62.59% while malignant LATs made up 37.41% of the total LATs [1-2]. Our study showed that 8.57% of the 35 cases included were malignant lesions. As for the pathology results, reports of the resected LATs in our study demonstrate that myelolipoma and adenoma were the two most common entities, with each occurring in 22.9% of patients in our study. Interestingly, the largest mass excised was an adrenal myelolipoma that was 21 cm in size (Figures 1,2); the mass was excised using a robot, and no complications occurred, nor was any blood transfusion required.
CT (Computed Tomography) image showing the largest mass in our study.
Postoperative image of the largest adrenal mass in our study, a 21 cm adrenal myelolipoma that was successfully resected using a robotic approach.
During adrenal surgery, the size of the tumor is an important factor to consider as the adrenal capsule could potentially rupture if great care is not taken. Tumors larger than five cm with a ruptured capsule pose an oncological risk during surgery. Laparoscopic equipment has limitations in movement and access to interior parts of the abdomen, which increases the risk of capsular rupture in large tumors and obese patients. The authors believe that robotic technology can handle tumors efficiently without causing capsular rupture, and can achieve the principle of controlling the adrenal vein as a first step in surgery. One author in the study successfully excised a 21 cm giant adrenal myolipoma using robotic technology (Figure 1,2). Comparative studies have shown that robotic approaches have better outcomes than laparoscopic approaches, with shorter operative times, lower morbidity rates, and fewer conversions [21-23]. Our research involved comparing the outcomes of unilateral laparoscopy, bilateral laparoscopy, and robotic laparoscopy in terms of EBL, ORT, and LOS. The use of robotic surgery resulted in lower rates of ORT and EBL as well as a shorter hospital. However, the availability of the robot in addition to the training of the surgeon limits its use.
Regardless of the size, adrenalectomy can be challenging based on its laterality. Right-sided adrenalectomies are complicated by the retrocaval location and short adrenal vein, while left-sided adrenalectomies require more mobilization and proximity to the pancreas. Previous research has shown that right adrenalectomies have shorter operative time and less blood loss than left adrenalectomies [24]. In our study, we found that a right adrenalectomy had a shorter operative time than a left or bilateral adrenalectomy. Unexpectedly, bilateral adrenalectomies had less blood loss and a shorter hospital stay compared to left or right adrenalectomy.
Although our study is the first in Saudi Arabia and the Middle East to focus on MIS for LATs, it is limited by several factors. First, the small sample of patients limits the ability to draw any strong conclusions. Additionally, the retrospective nature of the study adds to its limitations. However, we hope that this study encourages urologists in Saudi Arabia and the Middle East to continue to perform robotic and laparoscopic MIS for LATs, thus allowing us to perform a proper clinical trial for adequate comparison in the future.
Conclusions
With MIS being increasingly performed in Saudi Arabia, MIS for LATs is considered a safe approach that yields adequate surgical outcomes when compared to the traditional open approach in terms of EBL, perioperative complications, and more importantly, disease recurrence during the follow-up period. We hope that this study, within its limitations, encourages young skilled MIS urologists in the region to perform adrenalectomies by an MIS approach, rather than immediately resorting to an open surgical approach for LATs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laparoscopic resection of large adrenal tumors JSLS Zografos GN Farfaras A Vasiliadis G 3643681420102133318910.4293/108680810 X 12924466007160 PMC 3041032 · doi ↗ · pubmed ↗
- 2The role of laparoscopic adrenalectomy for adrenal tumours of 6 cm or greater Surg Endosc Parnaby CN Chong PS Chisholm L Farrow J Connell JM O'Dwyer PJ 6176212220081807179810.1007/s 00464-007-9709-7 · doi ↗ · pubmed ↗
- 3Should laparoscopic approach be proposed for large and/or potentially malignant adrenal tumors?Langenbecks Arch Surg Henry JF Defechereux T Gramatica L Raffaelli M 36636938419991047385710.1007/s 004230050215 · doi ↗ · pubmed ↗
- 4Retrospective evaluation of the outcome of open versus laparoscopic adrenalectomy for stage I and II adrenocortical cancer Eur Urol Porpiglia F Fiori C Daffara F 8738785720102013785010.1016/j.eururo.2010.01.036 · doi ↗ · pubmed ↗
- 5Surgical management of large adrenal tumors: impact of different laparoscopic approaches and resection methods on perioperative and long-term outcomes BMC Urol Chen W Liang Y Lin W Fu GQ Ma ZW 311820182973938810.1186/s 12894-018-0349-0PMC 5941476 · doi ↗ · pubmed ↗
- 6Retroperitoneal versus transperitoneal laparoscopic adrenalectomy in adrenal tumor: a meta-analysis Surg Laparosc Endosc Percutan Tech Chen W Li F Chen D Zhu Y He C Du Y Tan W 1211272320132357950410.1097/SLE.0b 013e 3182827 b 57 · doi ↗ · pubmed ↗
- 7Laparoscopic adrenalectomy for potentially malignant adrenal tumors greater than 5 centimeters J Clin Endocrinol Metab Liao CH Chueh SC Lai MK Hsiao PJ Chen J 308030839120061672066510.1210/jc.2005-2420 · doi ↗ · pubmed ↗
- 8Clinical analysis of adrenal lesions larger than 5 cm in diameter (an analysis of 251 cases)World J Surg Oncol Zhang Z Wang L Chen J 2201720193184290510.1186/s 12957-019-1765-7PMC 6916431 · doi ↗ · pubmed ↗