The Villain Who Saved the Day: The Paradoxical Value of Amiodarone in Managing Recurrent Ventricular Tachycardia Secondary to Amiodarone-Induced Thyroiditis
Rakan M Alotaibi, Khaled M Abdullah, Cheng Ken Ong, Vetton Chee Kay Lee, Jing W Goh

TL;DR
A patient with amiodarone-induced thyroiditis experienced dangerous heart rhythms but was successfully treated with amiodarone.
Contribution
Demonstrates the paradoxical effectiveness of amiodarone in managing arrhythmias caused by its own side effects.
Findings
Amiodarone-induced thyrotoxicosis can lead to life-threatening arrhythmias.
Amiodarone was successfully used to control arrhythmias in a patient with amiodarone-induced thyroiditis.
Abstract
Thyroiditis is a rare and serious complication for patients taking amiodarone. It can manifest with symptoms of hyperthyroidism and serious life-threatening arrhythmias. We present a case of a patient with amiodarone-induced thyrotoxicosis presenting with an electrical storm in which rhythm control was achieved with the utilization of amiodarone.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
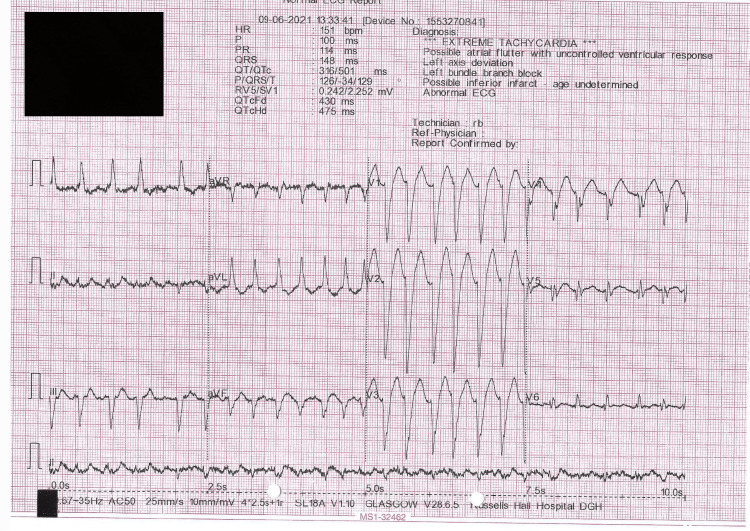 Figure 1
Figure 1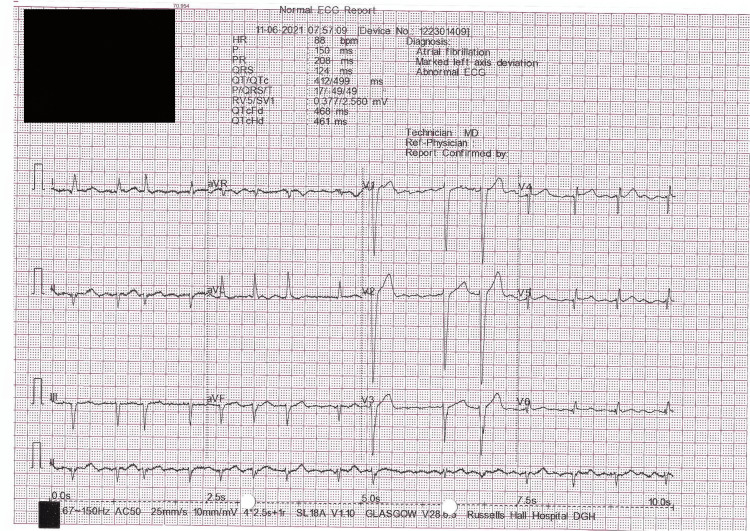 Figure 2
Figure 2| Test (unit) | Results (four months ago) | Results (Upon Admission) | Reference Range |
| TSH (mU/L) | 0.68 | < 0.01↓ | 0.4-4 |
| FT4 (pmol/L) | - | 53.1 ↑ | 10-28 |
| FT3 (pmol/L) | - | 6.8 | 4.6-9.7 |
| WBC Count (K/uL) | 8.4 | 9.0 | 4.5-11 |
| Hemoglobin (g/L) | 140 | 156 | Male: 138-172 Female: 121-151 |
| Platelets (x10^9/L) | 319 | 276 | 150-450 |
| Sodium (mmol/L) | 139 | 140 | 136-145 |
| Potassium (mmol/L) | 4.6 | 4.8 | 3.6-5.2 |
| GFR (mL/min) | >90 | >90 | >60 |
| CRP (mg/L) | - | 8.0 | 0-5 |
| Troponin (ng/L) | - | 22.0 | 0-14 |
| Magnesium (mmol/L) | 0.85 | 0.9 | 0.65-1.05 |
| Features | Type 1 AIT | Type 2 AIT |
| ↑ T4 and T3 Mechanism | Excessive synthesis | Excessive release (destructive thyroiditis) |
| Goiter | Often multinodular or diffuse | Often absent or small |
| Underlying Thyroid Disease | Usually latent Grave’s Disease | Usually absent |
| Thyroglobulin | ↑ | ↓ (relatively) |
| 24-hour Radioiodine Uptake | Detectable | No uptake |
| CFDS | ↑ vascularity | ↓ vascularity |
| Management | Thionamides + Surgery | Glucocorticoids + Surgery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac electrophysiology and arrhythmias · Ion channel regulation and function · Cardiac Arrhythmias and Treatments
Introduction
Amiodarone, a type III antiarrhythmic, is approved for the treatment of ventricular and supraventricular tachyarrhythmias [1]. Side effects are numerous, including both hypothyroidism and hyperthyroidism [2]. Although both are possible complications of amiodarone, the primary focus of this discussion will revolve around hyperthyroidism, particularly relating to arrhythmogenesis with overt thyroid dysfunction and the value of considering amiodarone in patients presenting with tachyarrhythmias associated with amiodarone-induced thyrotoxicosis (AIT). Approximately 14%-18% of patients on amiodarone may experience both thyrotoxicosis and hypothyroidism [3]. AIT is seen more commonly in regions with an iodine deficiency [4]. Conversely, amiodarone-induced hypothyroidism is seen in areas with sufficient iodine intake [5].
AIT can result either from increased synthesis of thyroid hormones (type I) or excess hormone release due to destructive thyroiditis (type II) [6]. In practice, both subtypes may clinically overlap, posing a considerable challenge for physicians to differentiate. Thus, management may include a combination of prednisone and antithyroid therapy [6,7]. Although mild AIT may subside spontaneously in 20% of patients [8], early recognition and management are critical as these patients were found to have a high incidence of mortality and morbidity [9].
Case presentation
A 46-year-old gentleman presented to the emergency department due to four intracardiac defibrillator (ICD) shocks within the last 24 hours while conscious and asymptomatic. On further questioning, he reported experiencing hot flashes for the past two months and has been on amiodarone since 2018 for recurrent ventricular arrhythmias. Vital signs were significant for tachycardia ranging from 140 to 150 beats per minute. On physical examination, he was alert, distressed, and mildly breathless with no lid lag or goiter. He had pansystolic murmurs at the apex with an irregularly irregular rhythm with no bilateral pedal edema. His lungs were clear to auscultation bilaterally. ICD interrogation confirmed episodes of atrial fibrillation and non-sustained ventricular tachycardia (VT), for which appropriate shocks were delivered. He had regular three-monthly cardiology outpatient follow-up with ICD analysis for arrhythmias which were normal before this admission.
The patient has a past medical history of chronic congestive heart failure (New York Heart Association class IV, American College of Cardiology stage D) secondary to Becker Muscular Dystrophy. His latest echocardiogram performed one month before this admission showed severely impaired left ventricular function with an estimated left ventricular ejection fraction of 10%-15% as well as moderate to severe mitral regurgitation. He had a primary prevention subcutaneous ICD implanted in 2013. His regular medications include amiodarone, bisoprolol, rivaroxaban, furosemide, ramipril, and ivabradine.
Given this patient’s history of severe congestive heart failure, the risk of VT significantly increases especially in the setting of other possible triggers. The possible etiologies of ventricular arrhythmia in this patient likely include anemia, dehydration, hyperthyroidism, electrolyte abnormalities, or toxins. Other causes may also include ischemia, pulmonary embolism, or anxiety.
On admission, EKG (Figure 1) showed regular broad complex VT with a heart rate of 151 beats per minute and a wide QRS complex of 148ms. Table 1 displays the blood results on admission and four months ago. Endocrinology was subsequently consulted in view of a deranged thyroid function test on admission suggesting hyperthyroidism. Further workup revealed that both anti-TSH receptor antibodies and anti-thyroid peroxidase antibodies (TPO) were negative. The thyroid isotope scan conducted showed no uptake of the tracer within the thyroid gland. Thus, the findings were more consistent with type 2 AIT.
EKG on PresentationEKG: Electrocardiogram.
The patient was started on intravenous magnesium, propylthiouracil and prednisolone as advised by the endocrinology team. He was started on intravenous amiodarone (150 mg administered intravenously over 10 minutes, followed by continuous intravenous infusion rate of 1 mg/min for six hours, then at an infusion rate of 0.5 mg/min for an additional 18 hours). His Amiodarone therapy of 200 mg orally once daily was then continued to control the risk of life-threatening ventricular arrhythmias. The patient reverted to rate-controlled atrial fibrillation (Figure 2) from day 3 of treatment and had a successful discharge home. His Amiodarone home dose is not changed after discharge.
EKG prior dischargeEKG: Electrocardiogram
The patient was advised to follow up with the cardiology and endocrinology clinics after hospital discharge. Following discussion and shared decision making with the patient, the endocrinologist has recommended the patient to be on propylthiouracil and prednisolone for AIT. The cardiologist advised the continuation of amiodarone as it was the most effective in achieving rhythm control for this patient compared to other antiarrhythmic agents.
Following three months from his previous discharge, the patient reported no symptoms of thyrotoxicosis and his thyroid levels had normalized. Thus, prednisolone was tapered and subsequently discontinued six months after his hospital discharge. He continued to be on propylthiouracil as he was not deemed suitable for thyroidectomy due to his severe heart failure.
Discussion
We report a 46-year-old gentleman who presented with ICD shocks while being hemodynamically stable, with a known medical history of Becker Muscular Dystrophy who has been on amiodarone, workup was consistent with AIT type 2. Studies have generally outlined two subtypes of AIT which are summarized in Table 2 [6].
Ventricular arrhythmias are serious and a potentially fatal consequence of AIT. In a retrospective study, the incidence of AIT was associated with a 2.7-fold increased risk of adverse cardiovascular events including myocardial infarction, heart failure, and ventricular arrhythmias when compared to euthyroid patients on amiodarone [10]. Moreover, an electrical storm is possible in patients with thyrotoxicosis and is defined, in patients with ICD, as three appropriate VT detections in 24 hours, treated by pacing, shock, or eventually untreated but closely monitored [11]. In our case, the patient sustained four ICD shocks within the last 24 hours and thus meets the definition of an electrical storm. Because the initial cause of thyrotoxicosis and arrhythmogenesis can be linked to amiodarone, physicians may consider an alternative management option to amiodarone for rhythm control when suspecting AIT.
In our case, the patient sustained four ICD shocks within the last 24 hours and thus meets the definition of an electrical storm. Because the initial cause of thyrotoxicosis and arrhythmogenesis can be linked to amiodarone, physicians may consider an alternative management option to amiodarone for rhythm control when suspecting AIT. However, in our case, it was deemed to continue Amiodarone in the setting of AIT given it is the first-line treatment for VT and continuing amiodarone is beneficial in such a case as the patient was receiving ICD shocks. Furthermore, Amiodarone remains the only guideline-recommended therapy for secondary VT with either ischemic or non-ischemic cardiomyopathy [12]. The use of other antiarrhythmic such as flecainide and propafenone are contraindicated in patients with structural heart disease including left ventricular dysfunction as it was associated with ventricular proarrhythmia [13,14].
In the immediate setting, stopping the drug is unlikely to have a major impact as the drug has an elimination half-life of approximately 100 days [15]. In hemodynamically unstable patients with VT, electrical cardioversion is recommended. In stable patients with VT, it is recommended to initially manage the patient with IV amiodarone and an oral beta-blocker [12]. In our case, amiodarone was able to achieve rhythm control. However, the management’s complexity increases considerably when considering long-term treatment. One study reported on a 56 male who had been on amiodarone for atrial fibrillation and presented with type 2 AIT. The patient was managed with discontinuing amiodarone and starting propylthiouracil; however, on outpatient follow-up the thyroid function test was still in the thyrotoxic range, hence requiring adding oral prednisolone with eventual resolution [16]. Additionally, Inaba et al reported a 61-year-old male who presented with thyrotoxicosis symptoms and had been on amiodarone for VT. Eventually workup showed AIT type I with papillary thyroid cancer and multinodular goiter. Amiodarone was discontinued and methimazole was started with a reported improved thyroid function test after 5 weeks and the patient was considered for total thyroidectomy [17].
Moreover, a retrospective cohort study has demonstrated that in circumstances where patients do not respond to medical treatment, require immediate improvement, or necessitate continued amiodarone treatment, a total thyroidectomy under general anesthesia is an effective and proper treatment option [18].
Although careful clinical judgment and decision are crucial for the appropriate management of such patients, we hope this discussion will encourage further reports and studies to gather more evidence to implement standardized guidelines on the use of amiodarone in this challenging subset of patients with AIT.
Conclusions
A thorough history and physical examination can help identify patients suffering from AIT. Differentiation between the subtypes can be challenging, therefore, management options tend to overlap the two subtypes. Long-term treatment of AIT is complex due to factors further complicating treatment decisions such as considering the importance of amiodarone in the management of arrhythmias. Despite relating to the initial pathogenesis, amiodarone may have a considerable role in achieving rhythm control in such patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A practical guide for clinicians who treat patients with amiodarone: 2007 Heart Rhythm Goldschlager N Epstein AE Naccarelli GV Olshansky B Singh B Collard HR Murphy E 12501259420071776563610.1016/j.hrthm.2007.07.020 · doi ↗ · pubmed ↗
- 2Amiodarone and the thyroid Am J Med Basaria S Cooper DS 70671411820051598990010.1016/j.amjmed.2004.11.028 · doi ↗ · pubmed ↗
- 3The effects of amiodarone on the thyroid Endocrine Rev Martino E Bartalena L Bogazzi F 2402542220011129482610.1210/edrv.22.2.0427 · doi ↗ · pubmed ↗
- 4Iodine-induced hyperthyroidism: occurrence and epidemiology Thyroid Stanbury JB Ermans AE Bourdoux P 8310081998949215810.1089/thy.1998.8.83 · doi ↗ · pubmed ↗
- 5Environmental iodine intake and thyroid dysfunction during chronic amiodarone therapy Ann Intern Med Martino E Safran M Aghini-Lombardi F 28341011984642829110.7326/0003-4819-101-1-28 · doi ↗ · pubmed ↗
- 6Treatment of amiodarone-induced thyrotoxicosis, a difficult challenge: results of a prospective study J Clin Endocrinol Metab Bartalena L Brogioni S Grasso L 29302933811996876885410.1210/jcem.81.8.8768854 · doi ↗ · pubmed ↗
- 7Diagnosis and management of amiodarone-induced thyrotoxicosis: similarities and differences between North American and European thyroidologists Clin Endocrinol (Oxf) Tanda ML Piantanida E Lai A 8128186920081841054610.1111/j.1365-2265.2008.03268.x · doi ↗ · pubmed ↗
- 8Clinical experience of amiodarone-induced thyrotoxicosis over a 3-year period: role of colour-flow Doppler sonography Clin Endocrinol (Oxf) Eaton SE Euinton HA Newman CM Weetman AP Bennet WM 33385620021184924410.1046/j.0300-0664.2001.01457.x · doi ↗ · pubmed ↗