Intra-pulmonary migration of a clavicle osteosynthesis pin: a case report
Kaouther Ben Amara, Sarra Zairi, Bechir Ben Radhia, Mahdi Abdennadher, Hazem Zribi, Adel Marghli

TL;DR
A 61-year-old man had a Kirschner pin from a clavicle fracture migrate into his lung 25 years after treatment, highlighting the long-term risks of such implants.
Contribution
This case report highlights the rare but serious complication of intra-pulmonary migration of a clavicle osteosynthesis pin.
Findings
A Kirschner pin used for clavicle fracture fixation migrated into the lung 25 years post-surgery.
Long-term follow-up is essential for patients with osteosynthesis pins to prevent life-threatening complications.
Abstract
Fractures of the clavicle are common injuries, which often require reduction and internal fixation. Although Kirschner pins have been commonly used to treat these fractures with good results, migration of these devices may result in severe internal lesions. We report herein the case of 61-year-old man, who presented for intrapulmonary migration of a Kirschner pin, 25 years after closed reduction and fixation of a clavicle fracture. Migration of an osteosynthesis pin can be lethal. Patients with osteosynthesis pins, should have a regular follow, until the removal of the wires.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
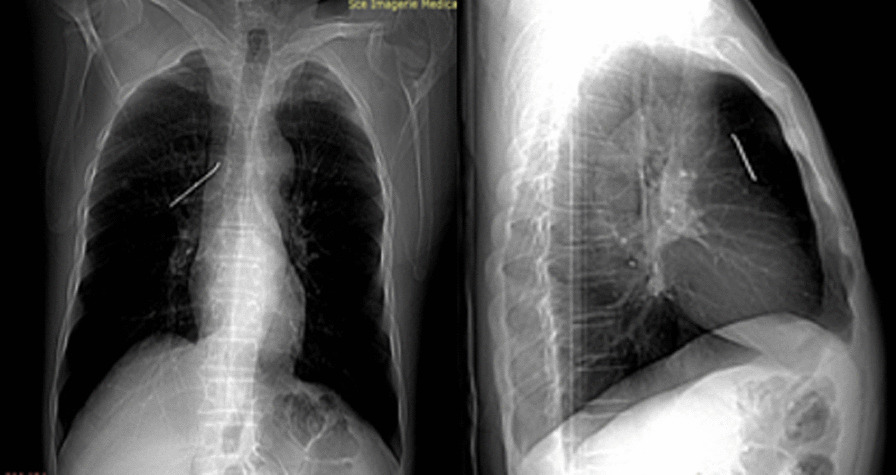 Figure 1
Figure 1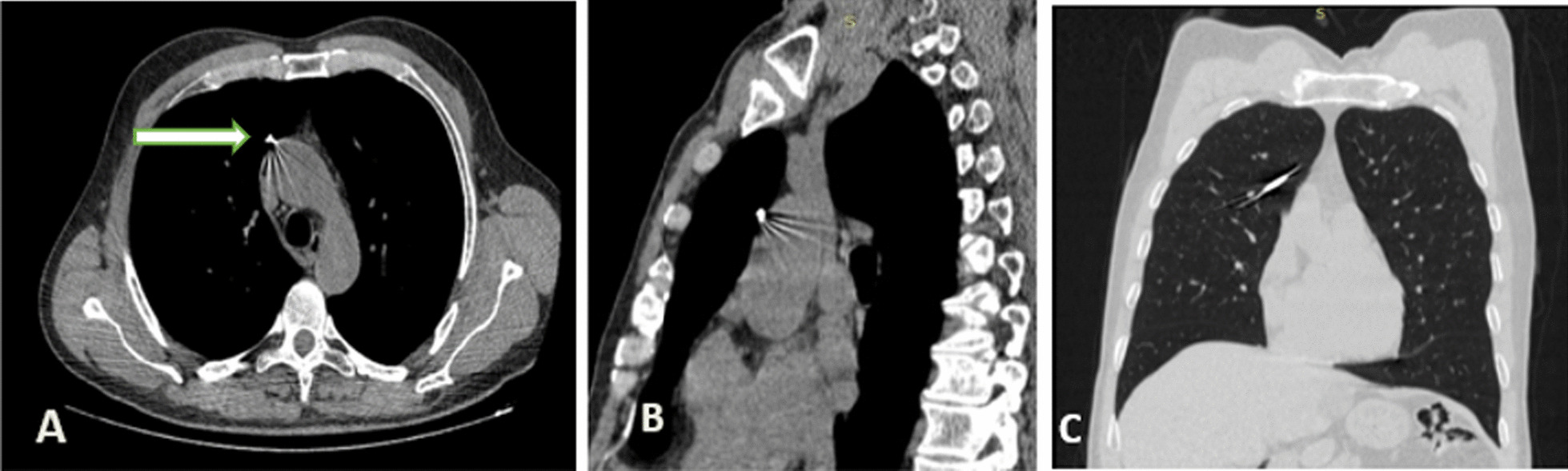 Figure 2
Figure 2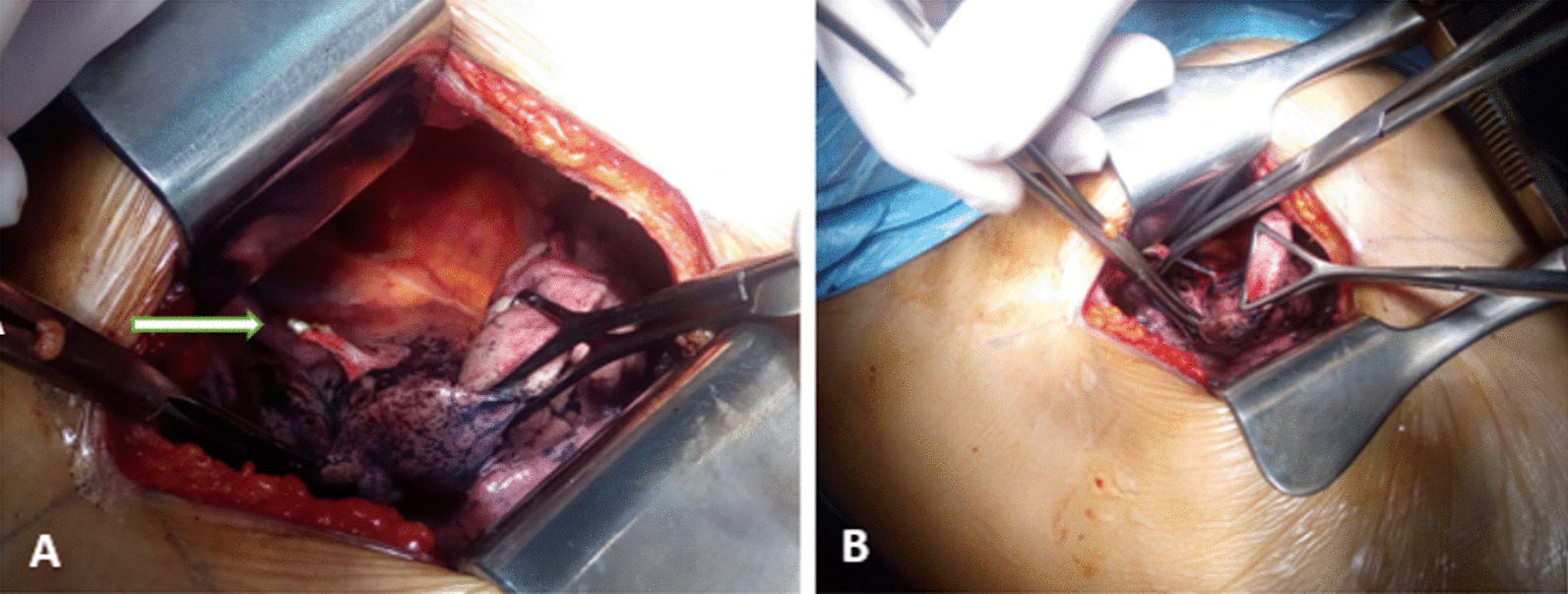 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder and Clavicle Injuries · Trauma Management and Diagnosis · Shoulder Injury and Treatment
Background
Fractures of the clavicle are common injuries. Most of them are successfully managed with conservative treatment. However, osteosynthesis with internal fixation may be required in some displaced fractures to avoid nonunion or malunion with secondary poor shoulder function [1]. Although Kirschner pins (K-pins) have been commonly used to treat these fractures with good results, secondary migration of these devices may result in serious vascular or visceral injuries [1–6]. We report herein the case of an intrapulmonary K-pin migration.
Case presentation
A 61-year-old smoking man presented to our outpatient clinic for recurrent tingling right chest pain. He had no comorbidities but, reported a right clavicle fracture which warranted surgical osteosynthesis, with internal fixation with a K-pin 25 years ago. Physical examination was normal. Chest X ray showed a K-pin in the right upper lobe (Fig. 1). The patient was unaware of the need to remove the pin after consolidation; therefore, he didn’t comply with follow-up. Chest CT with contrast enhancement showed a well-consolidated clavicle. No lesion of the great vessels or pneumothorax were shown. The pin’s tip was in close contact with the ascending aorta (Fig. 2). Given the potential involvement of the mediastinum, urgent surgical removal was decided through a lateral mini thoracotomy. The pin’s tip was retrieved in the surface of the right upper lobe without significant mediastinal adherence with the ascending aorta. A pneumotomy was performed above the pin’s tip, which was grasped with an indented forceps. It was gently mobilized laterally and then carefully pulled out, without secondary bleeding (Fig. 3). The parenchyma was tested for air leak. After thorough washing, the pneumotomy was closed with interrupted resorbable sutures and pleural cavity was closed on a chest tube. The postoperative course was uneventful. The patient was discharged 2 days after surgery. Further follow-up was uneventful.Fig. 1. Chest X ray showing a Kirschner pins in the right upper lobeFig. 2A–C Chest Computed tomography showing the wire in the upper right lobe adjacent to ascending aorta (white arrow shows well the pin)Fig. 3. Intra-operative images, Kirschner pins sitting seated in the mediastinal surface of the right upper lobe (A), removal of the pin (B) (white arrow shows well the pin)
Discussion
We reported the case of 61-year-old man who presented for an intrapulmonary migration of a K-pin, 25 years after a closed reduction and fixation of a clavicle fracture.
The migration of K-pins or metallic wires had been scarcely reported in literature. Lyons and Rockwood described 49 cases of K-wire migration in 47 patients, reported between 1943 and 1981 [7]. A recent review of the literature reported 68 cases of intra-thoracic migration. In most of these cases, migration was early. However, a great variability in the interval between positioning and migration of the K-pin has been reported, varying from 1 day to 21 years [2, 8]. In our case, migration was discovered 25 years later. Despite many attempts to explain the peculiar phenomenon, the exact reason remains unclear. Several factors might contribute to migration, such as muscle action, respiratory movements, intra-thoracic negative pressure, regional bone resorption, gravitational forces and the great range of motion of the upper extremity [6]. Some authors reported axillary migration with or without nervous lesions. Intra-thoracic migration is often followed with subsequent complication such as pneumothorax, hemothorax, lung consolidation, or hemoptysis. Migration to the lung had been mainly revealed with hemoptysis or pneumothorax [1, 4]. Fatal cardiac and vascular perforation [5] with hemothorax, collapse and pericardial tamponade, had also been described. Intra-abdominal migration through the diaphragm with or without intestinal perforation was also reported in 2 cases [2]. A variety of signs and complications have been described as a result of intra-thoracic migration such as pain, dyspnea, hemoptysis, anemia, subcutaneous emphysema, respiratory distress, and cardiac tamponade [4]. K-pin migration could be completely asymptomatic, dangerously delaying the diagnosis [2]. The type of the wire used, smooth, threaded or bent, did not impact the occurrence of migration [7].
Several precautions should be taken if K-pins are to be used for internal fixation of shoulder girdle fractures and dislocation. To prevent potential migration, it is highly recommended to bent sufficiently the extremities of the wire to involve the periosteum, or positioning the wire with percutaneous technique, avoiding, if possible, anterograde wire positioning. For tuberosity fixation, the use of a cannulated screw should be considered [2]. During fixation, K-pin positioning should be accurate, and, after pinning, hardware stability should be always checked through dynamic maneuvers. Pinning techniques should be carefully discussed especially in cases of elder patients with presumably low bone quality and low compliance to the immobilization regimen [2, 9]. Moreover, the patient must receive close clinical and radiographic follow-up until the K-pins are removed [9, 10]. The wires must be withdrawn when the desired therapeutic effect has been attained [10]. The surgeon must be aware of the risk of devastating organ damages. Reported complications of fractures, or shoulder girdle dislocation, particularly those arising at the sterno-clavicular joint, should be kept in mind.
In addition, displacements of considerable distance may occur in only a few hours after the diagnosis [1]. Our patient was lost to follow-up because he was unaware of the need to remove the pin.
If any sign of migration is detected, an X-ray and a CT scan should be performed. Surgical removal should be promptly performed, to prevent further complications. In the case of intra-thoracic migration, sternotomy [3] or thoracotomy [5] have been used by different authors. Sternotomy may be considered more appropriate in emergent conditions or in the presence of a cardiac or an intra-pericardial vascular injury [8]. A minimally invasive approach, such as video-assisted thoracoscopy may be useful for retrieving and removing an intrapulmonary migrated pin [11]. In our patient, we used a mini-lateral thoracotomy.
Conclusion
Although our patient underwent a successful removal of the wire and recovered uneventfully, migration of an osteosynthesis pin can be lethal. Patients with osteosynthesis pins, should have a regular follow, until the removal of the wires.
The surgeon must explain to the patient the importance of the regular follow-up, in order to detect any complication as soon as possible.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cameliere L Rosat P Heyndrickx M Le Rochais J-P Icard PJAC Annals T Migration of a Kirschner pin from the shoulder to the lung, requiring surgery Asian Cardiovasc Thorac Ann 201321222222310.1177/021849231245002124532628 · doi ↗ · pubmed ↗
- 2Cerruti P Mangano T Giovale M Repetto I Early asymptomatic intrathoracic migration of a threaded pin after proximal humeral osteosynthesis Int J Shoulder Surg 20161014110.4103/0973-6042.17452026980989 PMC 4772416 · doi ↗ · pubmed ↗
- 3Janssens de Varebeke B Van Osselaer G Migration of Kirschner's pin from the right sternoclavicular joint resulting in perforation of the pulmonary artery main trunk Acta Chirurg Belgica 1993936287918140842 · pubmed ↗
- 4Mellado J Calmet J García Forcada I SauríA GinéJ Early intrathoracic migration of Kirschner wires used for percutaneous osteosynthesis of a two-part humeral neck fracture: a case report Emerg Radiol 200411495210.1007/s 10140-004-0361-415278700 · doi ↗ · pubmed ↗
- 5Nordback I Markkula HJ Migration of Kirschner pin from clavicle into ascending aorta Acta Chirurg Scand 1985151217793890437 · pubmed ↗
- 6Wang S-Q Gao Y-S Mei J Ni M Wang J-Q Zeng Z-L Migration of a broken Kirschner pin into thoracic spinal canal 4 years following internal fixation of a clavicle fracture Eur J Orthopaed Surg Traumol 201020493510.1007/s 00590-010-0592-x · doi ↗
- 7Kumar P Godbole R Rees GM Sarkar PJ Intrathoracic migration of a Kirschner wire J Roy Soc Med 2002954198910.1177/01410768020950040911934911 PMC 1279515 · doi ↗ · pubmed ↗
- 8Venissac N Alifano M Dahan M Mouroux J Intrathoracic migration of Kirschner pins J Roy Soc Med 20006961953510.1016/s 0003-4975(00)01198-x 10892963 · doi ↗ · pubmed ↗