Diagnostic Challenges in Inflammatory Choroidal Neovascularization
Izabella Karska-Basta, Weronika Pociej-Marciak, Katarzyna Żuber-Łaskawiec, Anna Markiewicz, Michał Chrząszcz, Bożena Romanowska-Dixon, Agnieszka Kubicka-Trząska

TL;DR
Inflammatory choroidal neovascularization is a rare but serious eye condition linked to uveitis, and modern imaging techniques like OCT can help with diagnosis.
Contribution
The paper highlights the diagnostic challenges of iCNV and the potential of OCT and OCT angiography in improving detection.
Findings
Inflammation can cause hypoxia, promoting choroidal neovascularization in uveitis.
OCT and OCT angiography offer noninvasive tools to distinguish iCNV from choroiditis.
More research is needed to confirm the role of these imaging techniques in evaluating iCNV activity.
Abstract
Inflammation plays a key role in the induction of choroidal neovascularization (CNV). Inflammatory choroidal neovascularization (iCNV) is a severe but uncommon complication of both infectious and non-infectious uveitides. It is hypothesized that its pathogenesis is similar to that of wet age-related macular degeneration (AMD), and involves hypoxia as well as the release of vascular endothelial growth factor, stromal cell-derived factor 1-alpha, and other mediators. Inflammatory CNV develops when inflammation or infection directly involves the retinal pigment epithelium (RPE)–Bruch’s membrane complex. Inflammation itself can compromise perfusion, generating a gradient of retinal–choroidal hypoxia that additionally promotes the formation of choroidal neovascularization in the course of uveitis. The development of choroidal neovascularization may be a complication, especially in conditions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
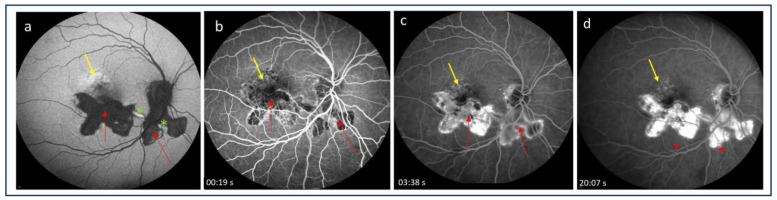 Figure 1
Figure 1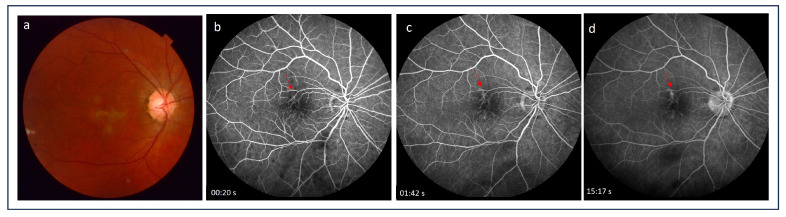 Figure 2
Figure 2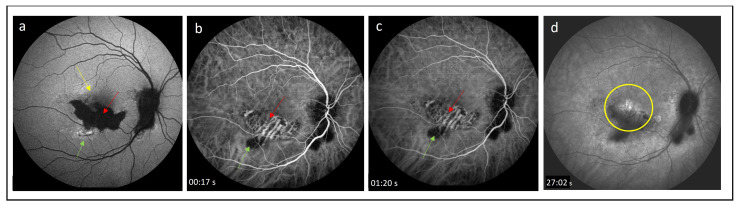 Figure 3
Figure 3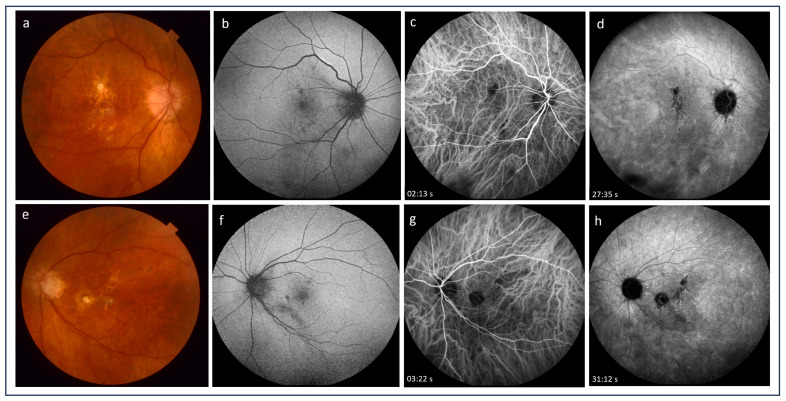 Figure 4
Figure 4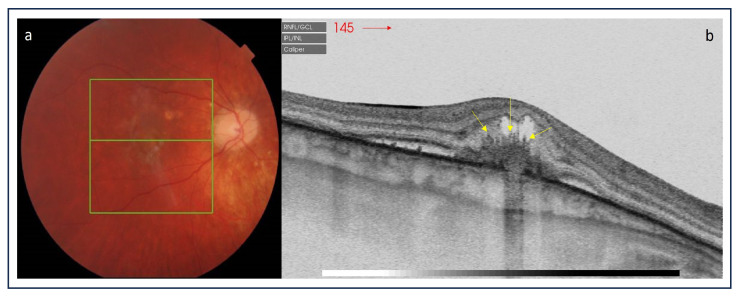 Figure 5
Figure 5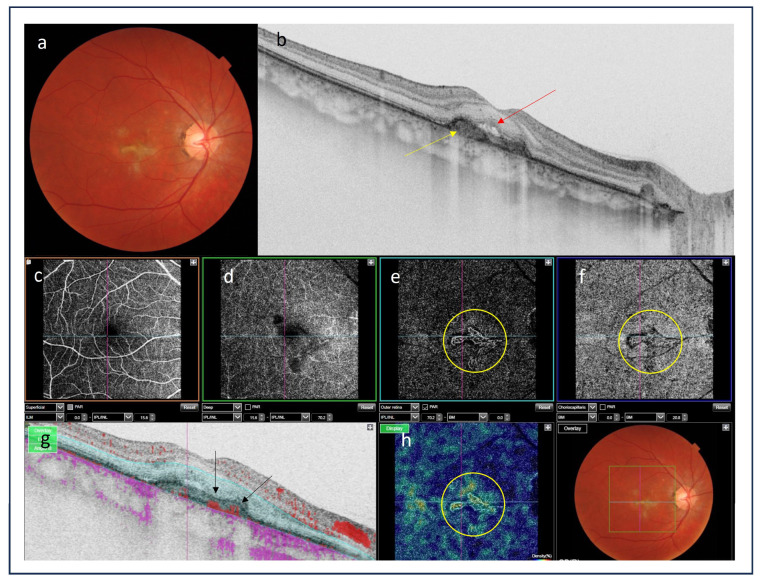 Figure 6
Figure 6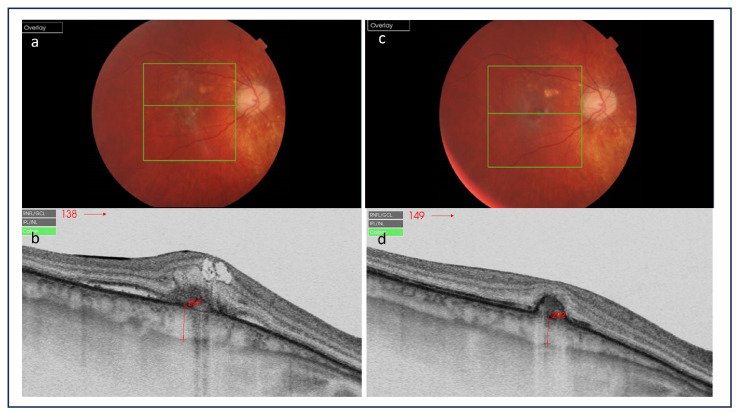 Figure 7
Figure 7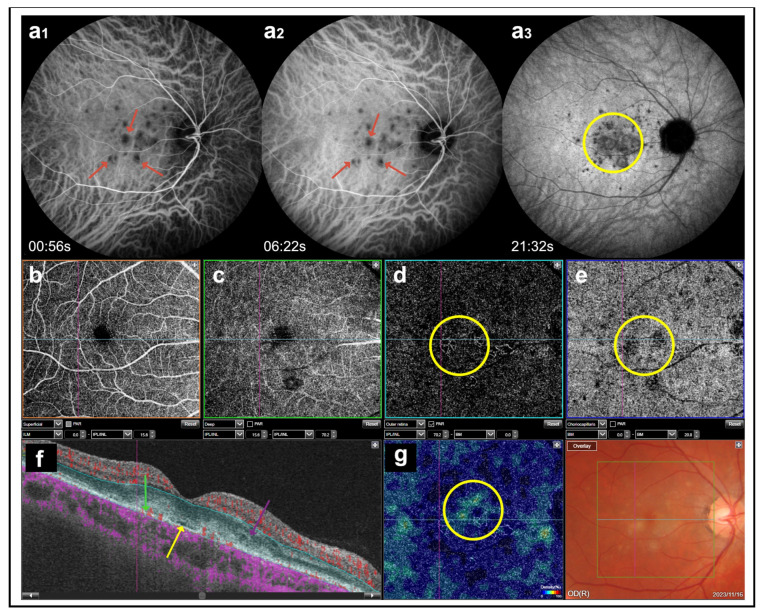 Figure 8
Figure 8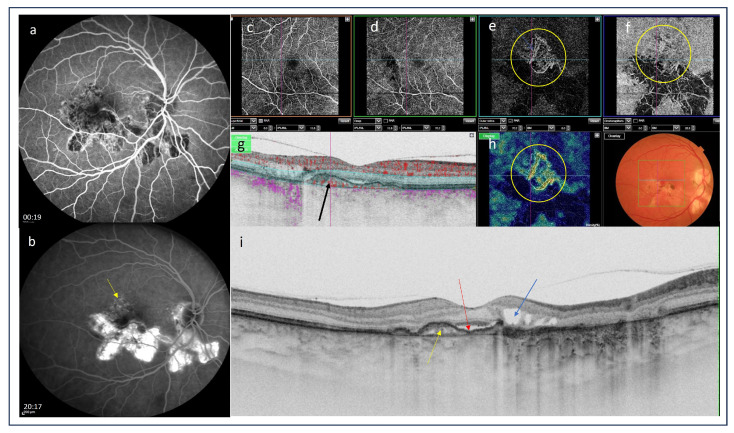 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Retinal Diseases and Treatments · Retinal and Optic Conditions
1. Introduction
Uveitis-related choroidal neovascularization (CNV), known as inflammatory CNV (iCNV), is an uncommon complication of uveitis. At the same time, it is one of the most severe causes of visual impairment in patients with uveitis [1,2,3]. Inflammatory CNV is the third cause of CNV following wet age-related macular degeneration (AMD) and pathological myopia [2,3]. Inflammatory CNV develops more frequently in patients with posterior uveitis (2.7%) and panuveitis (0.8%) as compared with those with anterior and intermediate uveitis (0.1%) [4]. CNV is a clinically important complication of both infectious and non-infectious uveitis and is found to be more frequent in some specific clinical entities. Its incidence in non-infectious posterior uveitis has been reported to reach 2% [5]. A higher incidence of CNV was reported in multifocal choroiditis, punctate inner choroidopathy, serpiginous choroidopathy, birdshot retinochoroidopathy, and Vogt–Koyanagi–Harada disease [6,7,8,9,10,11,12,13,14,15,16,17,18]. On the other hand, data on the incidence of iCNV secondary to infectious uveitis are scarce and are derived mainly from case series and case reports. The prevalence of iCNV, depending on the etiology of uveitis, is presented in Table 1.
According to Baxter et al. [4], the presence of epiretinal neovascularization is associated with an over three-fold higher risk of iCNV. Moreover, the risk of CNV was significantly greater in eyes with active inflammation vs. those with inactive inflammation. The presence of anterior chamber cells grade 2+, as defined by the Standardization of Uveitis Nomenclature Working Group, was shown to be associated with iCNV. However, increased vitreous cells and vitreous haze were not significantly associated with an altered risk of incident CNV in patients with uveitis [4]. A previous diagnosis of CNV in the contralateral eye was associated with a several-fold higher risk of CNV in the second eye. However, the eyes of patients with bilateral uveitis were less likely to develop CNV than the affected eyes of patients with unilateral uveitis [4].
The underlying pathophysiology of iCNV is likely similar to the pathophysiology of CNV in other conditions associated with CNV, such as age-related macular degeneration (AMD) or pathologic myopia. Inflammatory CNV may thus be considered not as a distinct form of CNV, but rather as associated with a set of circumstances that permit its development [1,2,3].
It was demonstrated that vascular endothelial growth factor (VEGF) plays a key role in CNV development [2,3]. Moreover, CNV has an extravascular component consisting of fibroblasts and leukocytes that express C-X-C motif chemokine receptor 4 (CXCR4). Retinal pigment epithelial (RPE) cells showed an increased production of tumor necrosis factor as well as interleukins IL-1, IL-2, IL-6, and IL-10, accounting for the inflammatory component of CNV [47,48]. Also, other mediators are involved in CNV development, such as nitric oxide, angiostatin, endostatin, C-C chemokine receptor type 3 (CCR3), and pigment epithelium-derived growth factor (PEDF), contrasting the neovascularization [49].
Recently, D’Ambrosio et al. [8], based on the immunohistochemical staining grading of three structures of CNV, namely, the RPE, vascular network, and fibroblasts for SDF1, CXCR4, and VEGF receptor 2, revealed differences in the CXCR4 staining of the vascular meshwork of iCNV as compared with AMD-related CNV, suggesting that capillaries have a different role in membrane development [8]. However, because of a low P value for the CXCR4 staining of the vascular meshwork of uveitis-related CNV versus AMD-related CNV, the authors concluded that further studies on this distinctive aspect are necessary [8].
There are two pathophysiological mechanisms by which uveitis can promote the development of iCNV [2,47]. The first one is associated with inflammation-mediated damage of the RPE-Bruch’s membrane complex, which disrupts the outer blood-retinal barrier and permits neovascular upgrowth from the choroid. The damage can be induced by an angiogenic stimulus mediated by local inflammation, or it can result from a combination of both [2]. The imbalance between the inhibitory and stimulatory actions of the soluble mediators produced by the RPE is supposed to be the trigger of neoangiogenesis. Activated inflammatory cells secrete enzymes that damage cells and cause degradation in the Bruch’s membrane. Proangiogenic cytokines released by these inflammatory cells may promote CNV growth through breaks in the membrane and into the sub-RPE space, potentially leading to edema, exudation, hemorrhages, and fibrosis, resulting in profound central vision loss [1,2]. Thus, a higher risk of damage to the RPE–Bruch’s membrane complex related to adjacent chorioretinal inflammation may explain the higher incidence of iCNV in patients with panuveitis and posterior uveitis [50]. It is noteworthy that the RPE is often intact in individuals with iCNV, and a majority of iCNVs are type 2 lesions (“classic” type CNVs) with abnormal growth of the vasculature into the outer retinal space [2,8]. The proposed mechanism of iCNV development is thus the focal breach of the RPE due to infection or inflammation leading to the growth and entry of new vessels into the outer retinal space [50]. The second theory explains that retinal and choroidal inflammation directly compromises perfusion, generating a gradient of retinal–choroidal hypoxia that promotes the formation of choroidal neovascularization [2]. It should also be noted that, in some cases, “idiopathic” choroidal neovascularization may herald the subsequent development of posterior uveitis [51].
Inflammatory CNV is typically diagnosed when a patient with uveitis reports a sudden deterioration of vision and/or metamorphopsias [2,3,4,52]. In advanced cases of iCNV, a central scotoma may be present. Some active extrafoveal lesions can be asymptomatic and may be missed initially due to the presence of associated features such as inflammatory lesions, scars, and pigmentation, as well as intra- or subretinal fluid accumulation [1,2,3,8]. In such cases, iCNV may be detected in imaging studies [1,6,52,53].
Inflammatory CNV lesions typically grow close to the edge of a postinflammatory atrophic chorioretinal scar, although iCNV can rarely be synchronous with an active disease [52,53]. Inflammatory CNVs can be subfoveal, extrafoveal, or juxtafoveal, and are highly focal [8]. These can be associated with intra- or subretinal hemorrhages and exudations. Inactive iCNV can result in a subretinal yellow-white scar, which may be associated with fibrosis and pigmentation. The presence of intra- or subretinal fluid with iCNV, as well as serous retinal detachment, may also represent signs of inflammation, leading to a misdiagnosis during a basic ophthalmological examination [1,2,3,4,8].
Thus, in patients with posterior uveitis, the identification of iCNV is challenging due to related abnormalities, including choroiditis, chorioretinal scarring, and inflammatory lesions [52,53]. Difficulties in a differential diagnosis of iCNV and active inflammatory lesions arise from the characteristic presence of intraretinal or subretinal fluid as well as serous retinal detachment in both [1,8,52]. An accurate characterization of inflammatory lesions is important for the diagnosis of an underlying pathology and the implementation of adequate treatment.
The aim of this paper was to discuss current multimodal imaging tools for the diagnosis of iCNV, with an emphasis on technological advances and future perspectives.
2. Imaging Tools for the Detection of iCNV
2.1. Fluorescein Angiography
Fluorescein angiography (FA) has been widely employed in the diagnosis of CNV secondary to various ocular pathologies. Since iCNV is often a classic type of neovascular membrane (type 2), it can be visualized by FA. CNV lesions are present on FA as early iso- or hyperfluorescence with late leakage [54]. Similarly, active inflammatory lesions show features of early isofluorescence (although mostly hypofluorescence) and late leakage, while inactive atrophic lesions are characterized by early hypo- or isofluorescence with late staining (suggesting an RPE window defect) without leakage [4,55,56] (Figure 1 and Figure 2). These highly similar FA features of iCNV and inflammatory lesions pose a diagnostic challenge. In conditions such as multifocal choroiditis, serpiginous choroiditis, or Vogt–Koyanagi–Harada disease, which present with scarring and pigmentation due to extensive retinal involvement, the detection of hyperfluorescence associated with CNV may be particularly difficult [52,53,57]. Thus, FA alone may be insufficient to identify iCNV lesions and initiate appropriate therapy. Therefore, a multimodal approach with additional tests is recommended.
2.2. Indocyanine Green Angiography
One of the imaging techniques for the visualization of the choroid is indocyanine green angiography (ICGA), which allows a better visualization of the choroid compared with FA [58]. ICGA plays an important role in assessing pathologies involving the choroidal vasculature and choriocapillaris in chorioretinal inflammatory diseases. It is helpful in differentiating between iCNV and inflammatory lesions [59,60]. ICGA allows us to tell the difference between a recurrent inflammatory focus and iCNV: the former appears as an early hypofluorescent lesion, whereas the latter has been a hyperfluorescent lesion since early angiographic frames [58,59]. ICGA is also mandatory in the case of CNV associated with choriocapillaritis, such as multifocal choroiditis (MFC), where it shows the extent of occult choriocapillaris nonperfusion and hence the risk for CNV development [60,61]. CNV secondary to MFC is more frequent in inflamed areas; however, this may originate from an old chorioretinal scar as well. Low-grade chronic inflammation can be at the core of this process, and ICGA frequently shows areas of non-perfusion indicating ischemia, which may be the trigger of angiogenesis. In such cases, ICGA is essential in the evaluation of the choroidal status. Importantly, ICGA was shown to outperform FA in detecting occult CNV lesions [54]. While iCNV is typically a classic lesion that can be easily visualized by FA, ICGA has been recently reported to be more accurate in assessing the size of neovascular lesions, especially in patients with idiopathic CNV, which shares several clinical features with iCNV [62]. Thus, ICG helps identify both iCNV and inflammatory choroidal alterations in patients with uveitis, allowing clinical differentiation between these lesions and a more comprehensive evaluation of the disease [60] (Figure 3 and Figure 4).
2.3. Optical Coherence Tomography
Optical coherence tomography (OCT) is a noninvasive and highly repeatable imaging technique that has revolutionized the management of retinal and choroidal diseases. By providing the quasi-histological sections of the ocular structure, it allows clinicians to identify ocular pathologies and assess response to treatment [63]. Moreover, the enhanced depth imaging modality of OCT can be used to evaluate choroidal thickness and structural modifications, which is particularly valuable in the treatment of uveitis [63].
Inflammatory CNV usually develops between the RPE and neurosensory retina, demonstrating similar features on OCT imaging as classic (type 2) CNV [58]. In both cases, the lesions appear as hyperreflective structures located in front of a disrupted RPE, with solid tissue in the subretinal space [1,64,65,66]. However, there is a single OCT feature that can help distinguish between iCNV and other classic CNVs. This is the so-called “pitchfork sign”, characterized by finger-like hyperreflective lesions extending from the CNV into the outer retinal layers, and it allows us to differentiate iCNV from other causes of CNV [1,53,67,68] (Figure 5). The inflammatory conditions associated with this sign include idiopathic multifocal choroiditis/punctate inner choroidopathy (MFC/PIC), intraocular tuberculosis, and acute syphilitic posterior placoid chorioretinitis [1,53,67,68]. Rajabian et al. and Berensztejn et al. reported “pitchfork signs” in patients with choroidal osteoma. The authors proposed that inflammation is the most important stimulus for the development of CNV in these cases [69,70]. However, recently, Falavrajani et al. [71] have described the “pitchfork sign” in five eyes with type 2 CNV and without any sign of ocular inflammation. They speculated that traction of the type 2 CNV complex on the outer retinal layers and consequent dragging of the layers or Müller cell activation could explain the presence of the “pitchfork sign” [71].
It was reported that the OCT features of CNV activity such as retinal thickening, subretinal and intraretinal fluid, intraretinal hyperreflective flecks, and undefined boundaries of subretinal material predicted the presence of FA leakage [1,66] (Figure 6b,g). Thus, it was concluded that OCT can be used for monitoring disease progression and response to treatment [68,72].
Moreover, central retinal thickness evaluated by OCT is often used as an objective measure of iCNV activity [73,74,75]. Recently, Giuffrè et al. [76] demonstrated increased choroidal thickness under iCNV that decreases after therapy: the so-called “sponge sign” (Figure 7). The authors investigate choroidal thickness changes related to the clinical activity of inflammatory choroidal neovascularization in punctate inner choroidopathy/multifocal choroiditis as compared to myopic choroidal neovascularization. They found that choroidal thickness beneath inflammatory choroidal neovascularization significantly increased at baseline and decreased after therapy, reaching preclinical values. Conversely, no significant choroidal thickness changes were disclosed in myopic choroidal neovascularization eyes, under any location. Thus, OCT-based choroidal thickness evaluation may represent an additional useful tool to monitor inflammatory choroidal neovascularization activity. Moreover, choroidal thickness under CNV could be used to discriminate the origin of the choroidal neovascular membrane in doubtful cases (either inflammatory or myopic) and to guide therapeutic management [76].
OCT images can also help differentiate between iCNV lesions and non-neovascular alterations at the RPE level that are characteristic of several types of uveitis. For example, acute inflammatory foci in multifocal choroiditis show a deeper penetration of the OCT signal, a feature that is usually not seen in iCNV [56,65]. However, when distinguishing CNV lesions from iCNV, the use of OCT alone may be limited as these lesions display similar features of outer retinal or RPE hyperreflectivity, intraretinal edema, sub-RPE fluid, and exudation in conditions with the involvement of the RPE or choriocapillaris (e.g., multifocal choroiditis and punctate inner choroidopathy) [1,74,75,77,78]. In such cases, the characteristics of the lesions can be determined by a combination of FA, ICGA, and OCT angiography (OCTA).
2.4. Optical Coherence Tomography Angiography
The usefulness of OCTA as a noninvasive technique for the detection of iCNV has been reported by several investigators. Cheng et al. [79] assessed the ability of OCTA to detect iCNV and differentiate it from inflammatory lesions as compared with conventional FA in 26 patients with multifocal choroiditis. The authors concluded that OCTA outperformed FA in differentiating CNV from inflammatory lesions, as the latter do not show any blood flow signals. It also permitted the visualization of the detailed vascular structure of CNV. Therefore, it could be used as an alternative option for CNV identification and to guide therapeutic decision making [77]. Similarly, in a recent retrospective study of 14 patients, Zahid et al. [80] used OCTA to evaluate neovascular flow signals in macular chorioretinal lesions occurring in idiopathic multifocal choroiditis. They concluded that OCTA may be a useful tool for understanding the pathophysiology of the disease and monitoring its course. The utility of OCTA for the noninvasive diagnosis of iCNV and its subsequent follow-up was also confirmed by Yee et al. [81]. Finally, in a recent study, Aggarwal et al. [82] investigated the OCTA features of tuberculosis-associated choroiditis in comparison with conventional imaging modalities, including FA, ICGA, and OCTA. This was the first study to demonstrate that OCTA can identify type 1 neovascular networks. The research led to the conclusion that OCTA is indispensable to exclude neovascular networks when FA, ICGA, and OCT results are inconclusive [81] (Figure 6c–h, Figure 8 and Figure 9).
In patients with posterior uveitis, the identification of iCNV is challenging due to related abnormalities, including associated pathologies such as choroiditis, chorioretinal lesions, and choroidal scarring [1,82,83]. In such cases, OCTA allows noninvasive diagnostic imaging of iCNV and differentiation from inflammatory pathologies [1,82,83].
While the above studies prove the role of OCTA in the diagnosis and follow-up of patients with iCNV, larger prospective studies are needed to determine its advantages over conventional imaging.
2.5. Near-Infrared Autofluorescence Imaging
Fundus autofluorescence (FAF) is a valuable imaging tool for multiple anatomical and physiological alterations in the ocular tissue [84]. Essentially, FAF is a map of lipofuscin distribution, which is the autofluorescent pigment of the eye naturally found in the RPE–photoreceptor complex [85]. It was reported that iCNV lesions may show a different pattern on FAF imaging than active inflammatory foci [1,84,85]. In FAF, normal autofluorescence may occur in active iCNV with preserved neurosensory retina [1,83,84,85,86]. Prolonged active CNV tends to present hyperautofluorescence, while hypoautofluorescent areas correlate with photoreceptor and RPE loss [1,83,86] (Figure 1a and Figure 7b). Active inflammatory foci may show an increased autofluorescence signal [84,85] (Figure 3a). Therefore, the technique may be used for differentiating between inflammatory and CNV lesions.
3. Conclusions
The detection of inflammatory CNV remains a challenge due to the presence of choroiditis lesions, scarring, and pigmentation that make it difficult to visualize CNV lesions. Available case reports and case series point to the benefits of using OCTA in combination with conventional imaging modalities such as FA, OCT, and ICGA. This multimodal approach may improve the detection and follow-up of iCNV lesions. OCTA is also an important addition to FA and ICGA in terms of providing important information on retinochoroidal abnormalities associated with uveitis, such as the severity of inflammation or the presence of any vascular changes and focal lesions. It may offer advantages over traditional modalities in the detection of neovascular flow in uveitis, but it should be used as an additional tool rather than a replacement for the existing ones. Also, FAF requires further research to reveal whether this imaging modality can be used to differentiate between iCNV and inflammatory lesions and between AMD-related CNV and CNV related to inflammatory disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agarwal A. Invernizzi A. Singh R.B. Foulsham W. Aggarwal K. Handa S. Agrawal R. Pavesio C. Gupta V. An update on inflammatory choroidal neovascularization: Epidemiology, multimodal imaging, and management J. Ophthalmic Inflamm. Infect.201881310.1186/s 12348-018-0155-630209691 PMC 6135736 · doi ↗ · pubmed ↗
- 2Dhingra N. Kelly S. Majid M.A. Bailey C.B. Dick A.D. Inflammatory choroidal neovascular membrane in posterior uveitis-pathogenesis and treatment Indian. J. Ophthalmol.20105831010.4103/0301-4738.5846720029141 PMC 2841372 · doi ↗ · pubmed ↗
- 3Neri P. Lettieri M. Fortuna C. Manoni M. Giovannini A. Inflammatory choroidal neovascularization Middle East. Afr. J. Ophthalmol.20091624525110.4103/0974-9233.5842220404991 PMC 2855665 · doi ↗ · pubmed ↗
- 4Baxter S.L. Pistilli M. Pujari S.S. Liesegang T.L. Suhler E.B. Thorne J.E. Foster C.S. Jabs D.A. Levy-Clarke G.A. Nussenblatt R.B. Risk of choroidal neovascularization among the uveitides Am. J. Ophthalmol.201315646847710.1016/j.ajo.2013.04.04023795984 PMC 3748230 · doi ↗ · pubmed ↗
- 5Dreyer R.F. Gass D.J. Multifocal choroiditis and panuveitis. A syndrome that mimics ocular histoplasmosis Arch. Ophthalmol.19841021776178410.1001/archopht.1984.010400314400196508619 · doi ↗ · pubmed ↗
- 6Morgan C.M. Schatz H. Recurrent Multifocal Choroiditis Ophthalmology 1986931138114710.1016/S 0161-6420(86)33611-X 2433660 · doi ↗ · pubmed ↗
- 7Brown J.Jr. Folk J.C. Reddy C.V. Kimura A.E. Visual prognosis of multifocal choroiditis, punctate inner choroidopathy, and the diffuse subretinal fibrosis syndrome Ophthalmology 19961031100110510.1016/S 0161-6420(96)30561-78684800 · doi ↗ · pubmed ↗
- 8Ahnood D. Madhusudhan S. Tsaloumas M.D. Waheed N.K. Keane P.A. Denniston A.K. Punctate inner choroidopathy: A review Surv. Ophthalmol.20176211312610.1016/j.survophthal.2016.10.00327751823 · doi ↗ · pubmed ↗