Atlas of Tumor and Tumor Microenvironment Cells of Lymphovascular Space Invasion (LVSI) in High-Grade Serous Endometrial Adenocarcinoma: A Case Study
Raed Sulaiman, Adam Dale, Xiaoqian Lin, Jennifer C. Aske, Kris Gaster, David Starks, Luis Rojas Espaillat, Pradip De, Nandini Dey

TL;DR
This study creates a detailed map of tumor and surrounding cells involved in lymphovascular invasion in a high-grade endometrial cancer case.
Contribution
The first marker-based immunohistological atlas of tumor and TME cells in LVSI of high-grade endometrial adenocarcinoma.
Findings
Tumor cells within LVSI are positive for IL-12R-B2 and S100A4.
LVSI involves changes in the immune landscape of both tumor and tumor microenvironment.
Expressions of epithelial, proliferation, apoptosis, and immune markers were characterized in LVSI.
Abstract
Lymphovascular invasion (LVSI) is defined as the presence of tumor cells within a definite endothelial-lined space (lymphatics or blood vessels) in the organ surrounding invasive carcinoma. The presence of LVI is associated with an increased risk of lymph nodes and distant metastases. Lymphovascular invasion is described as cancer within blood or lymph vessels and is an independent risk factor for metastasis, recurrence, and mortality. This study aims to present the marker-based immunohistological characterization of cells around LVSI in a high-grade adenocarcinoma of the endometrium to build a cellular atlas of cells of LVSI. A cellular characterization of the cells around lymphovascular space invasion in a 67-year-old female patient with invasive high-grade serous endometrial adenocarcinomas is presented. Resected tumor tissue from a consented patient with invasive high-grade serous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1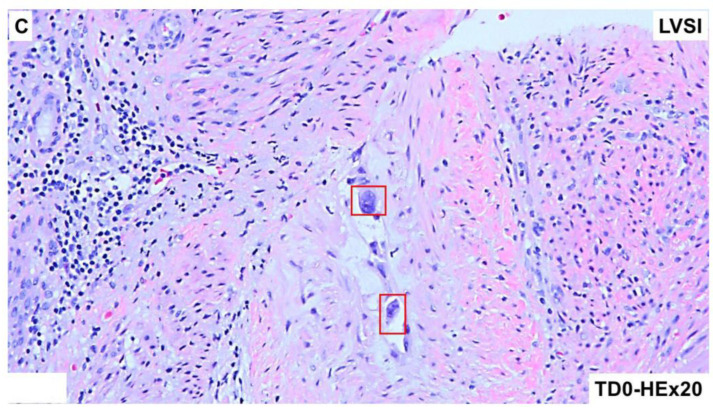 Figure 2
Figure 2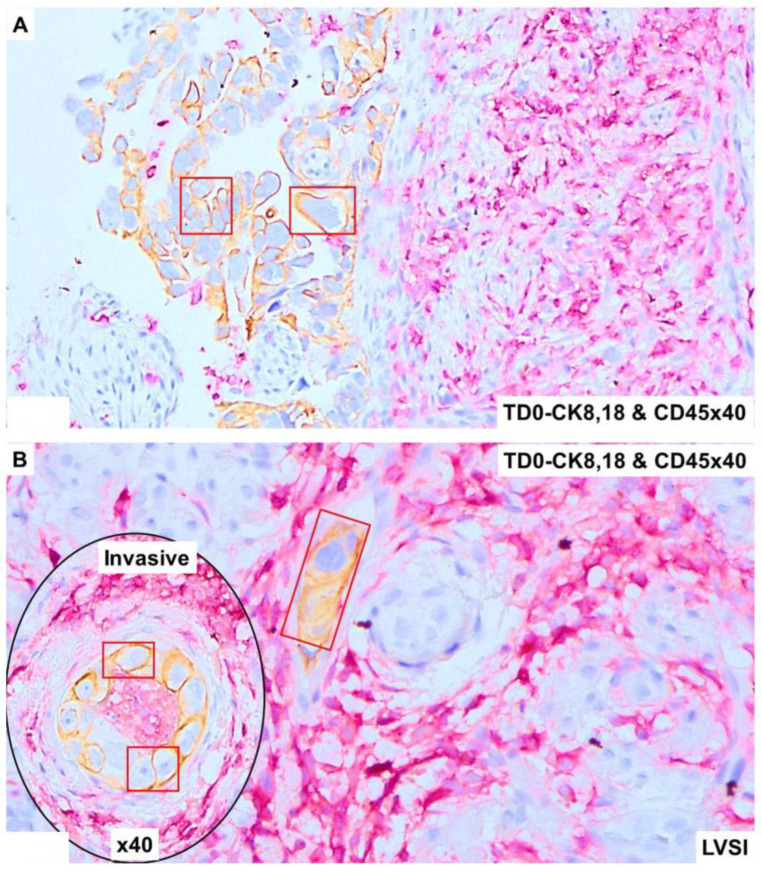 Figure 3
Figure 3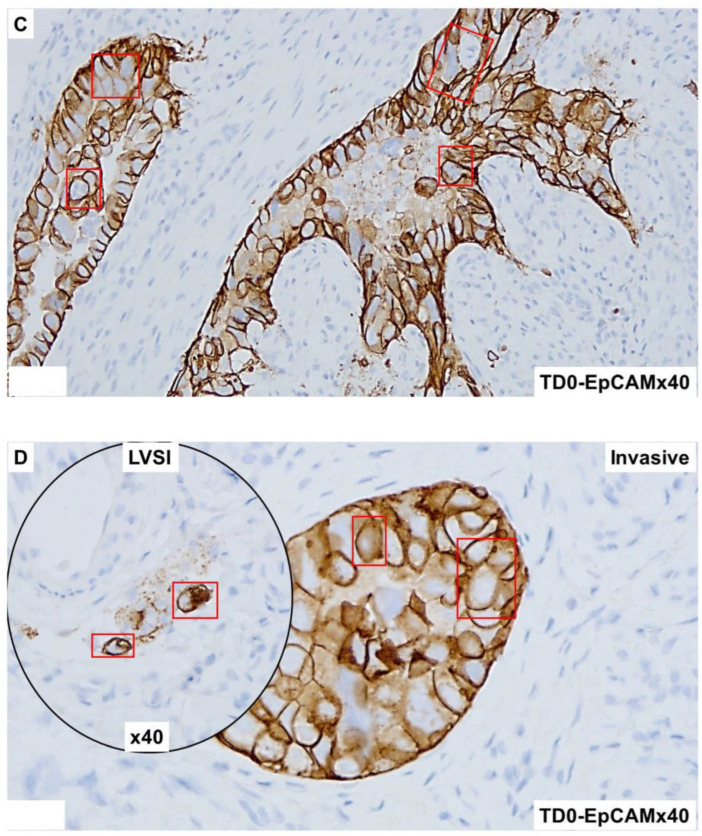 Figure 4
Figure 4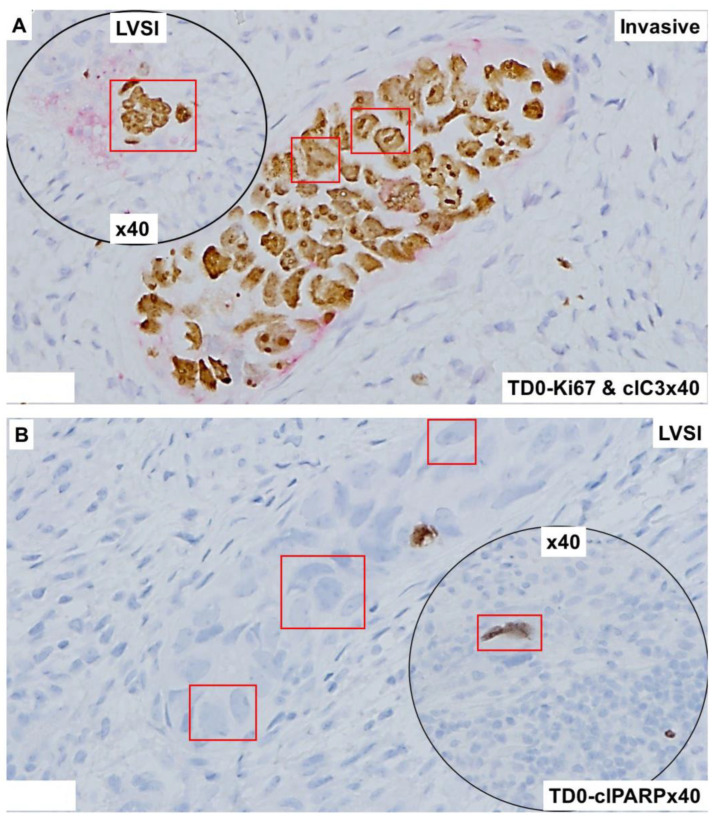 Figure 5
Figure 5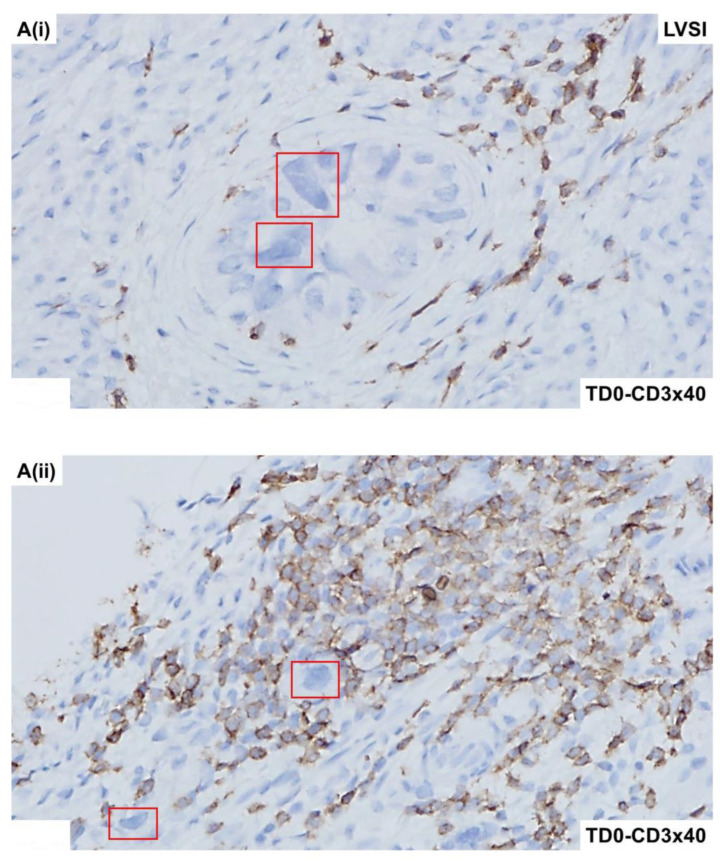 Figure 6
Figure 6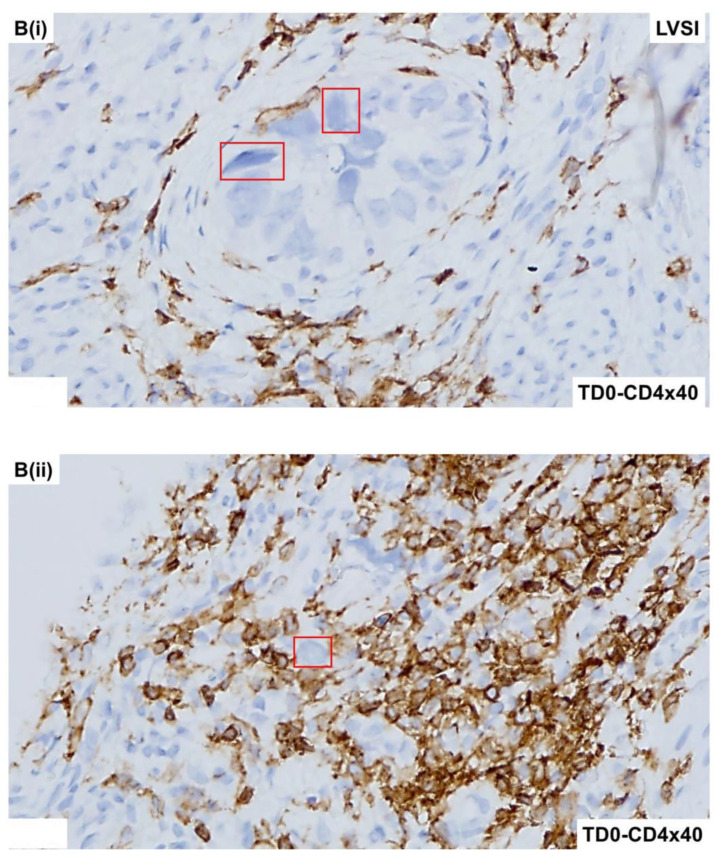 Figure 7
Figure 7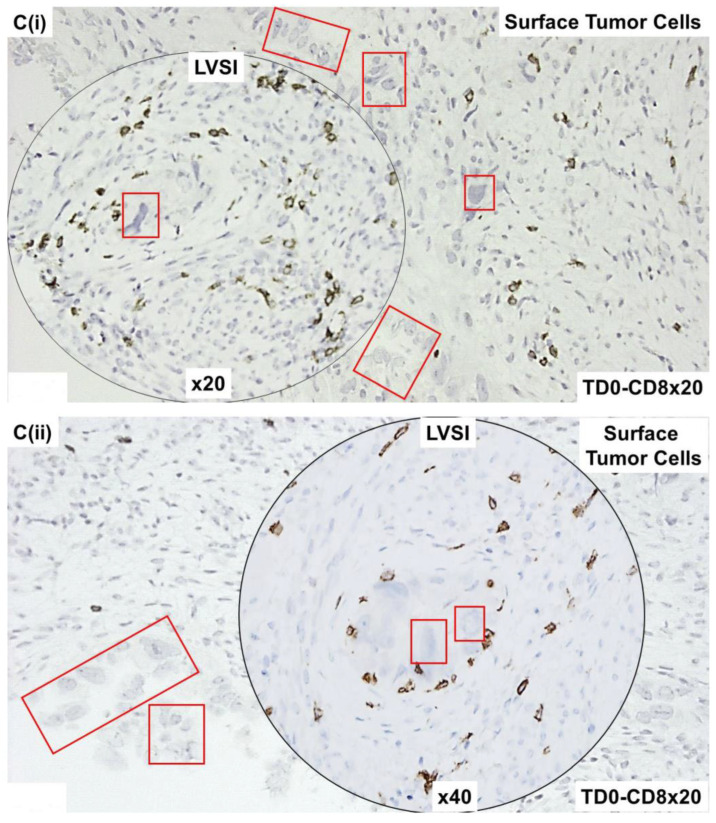 Figure 8
Figure 8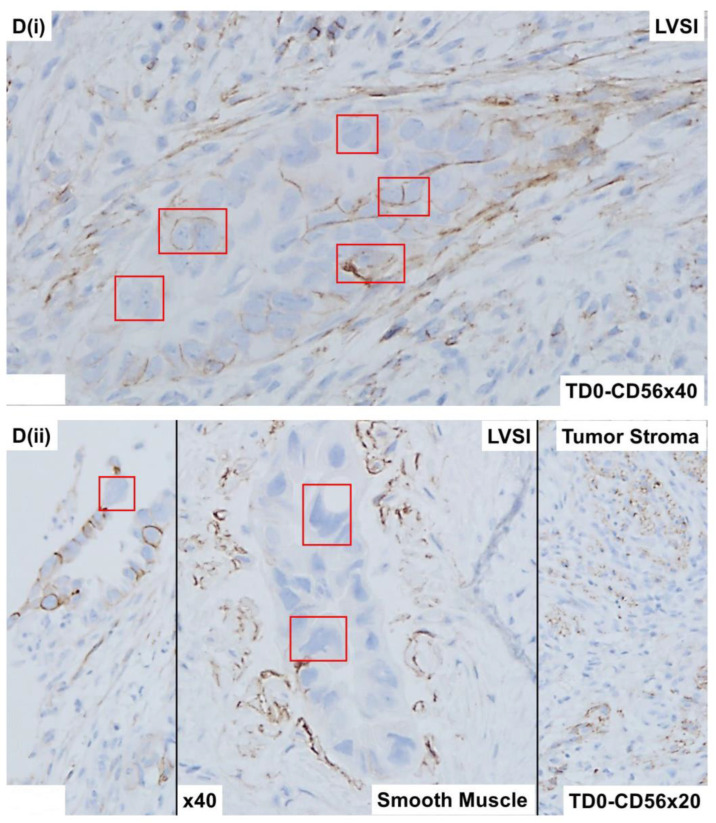 Figure 9
Figure 9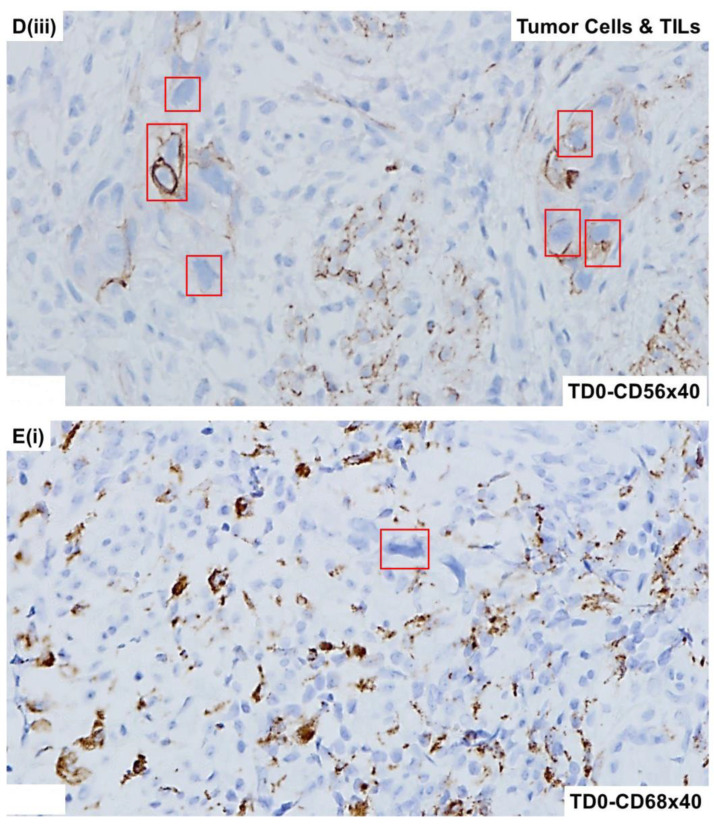 Figure 10
Figure 10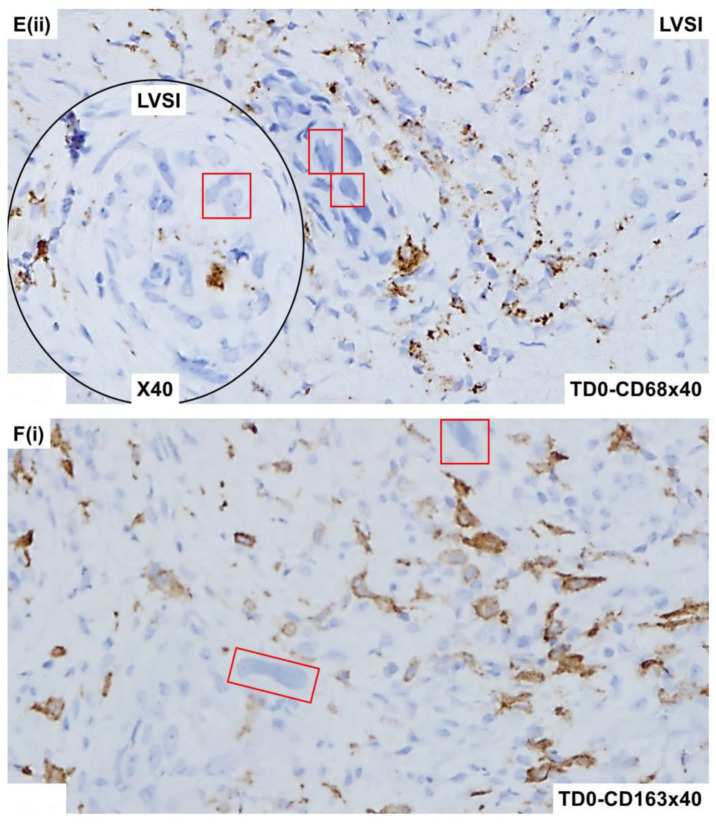 Figure 11
Figure 11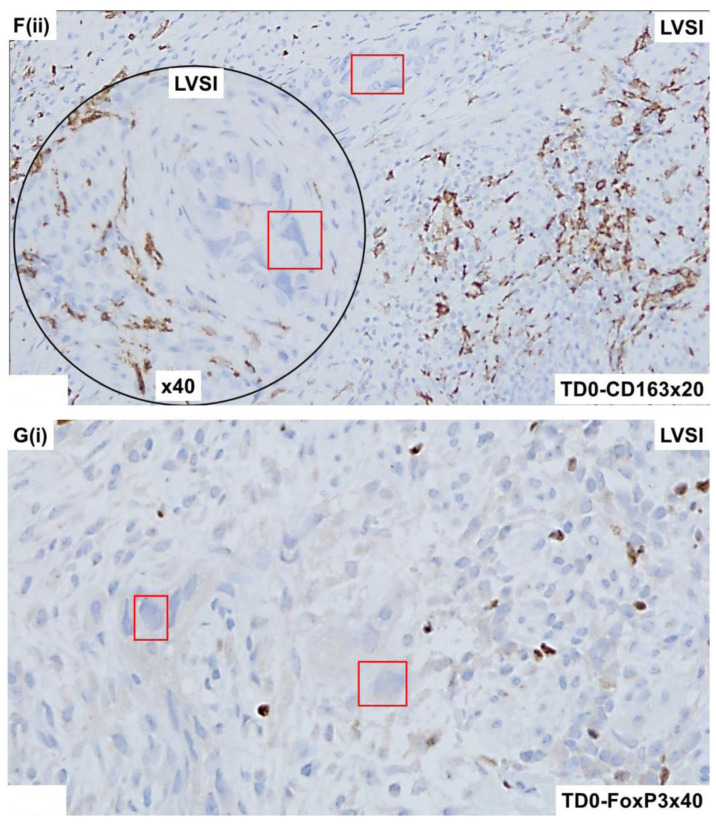 Figure 12
Figure 12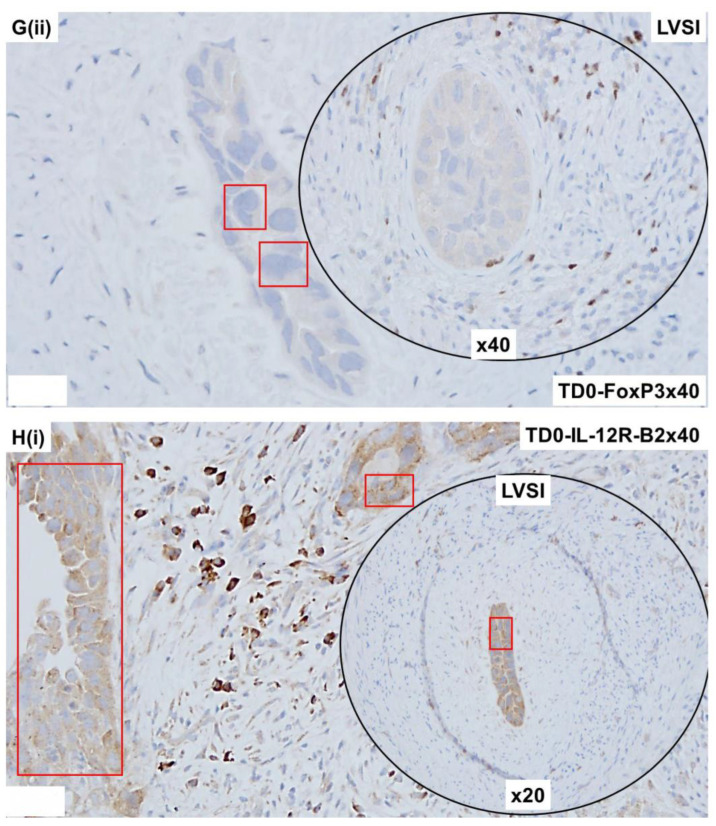 Figure 13
Figure 13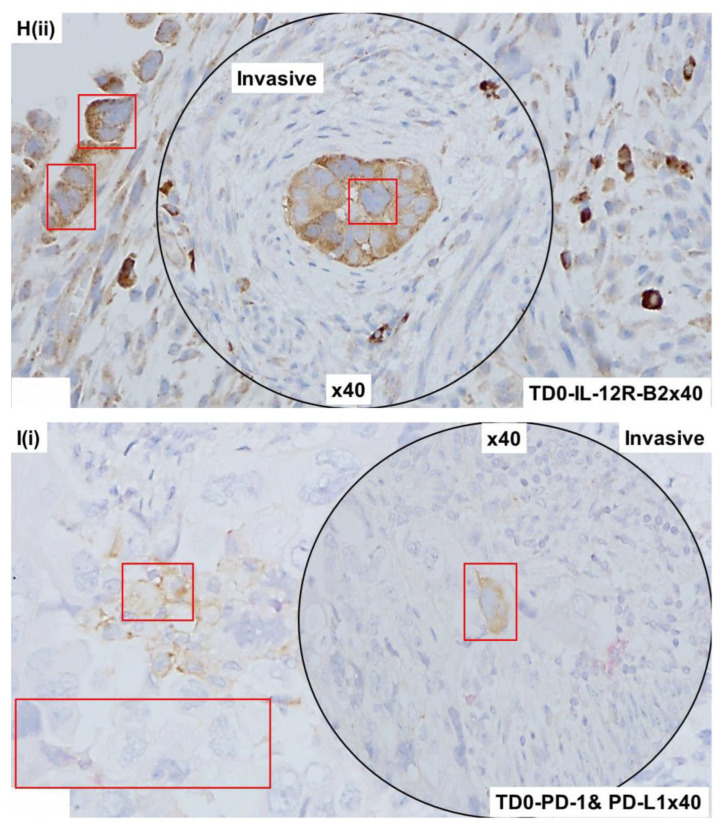 Figure 14
Figure 14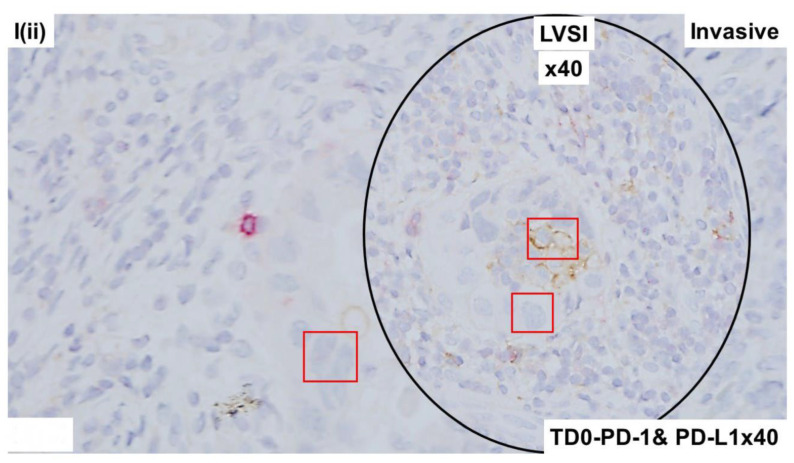 Figure 15
Figure 15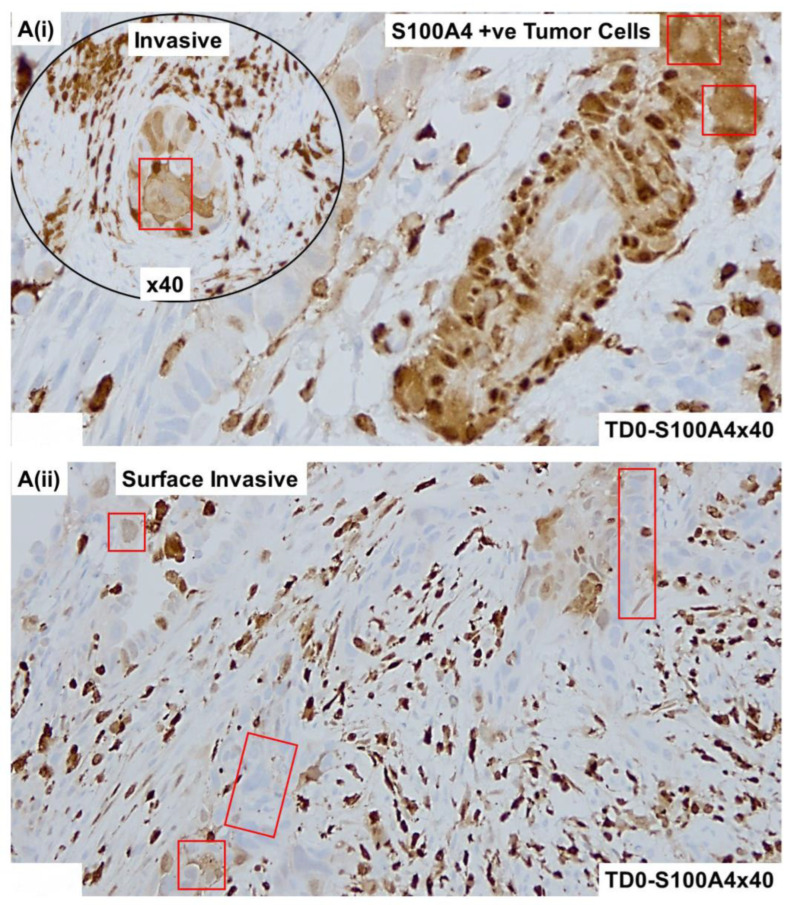 Figure 16
Figure 16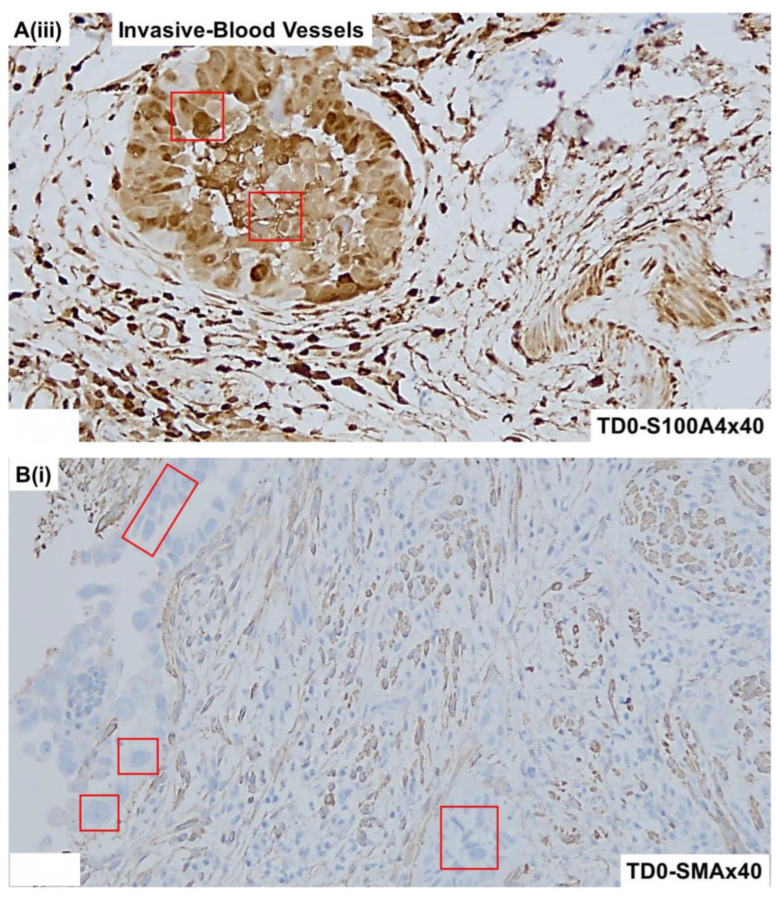 Figure 17
Figure 17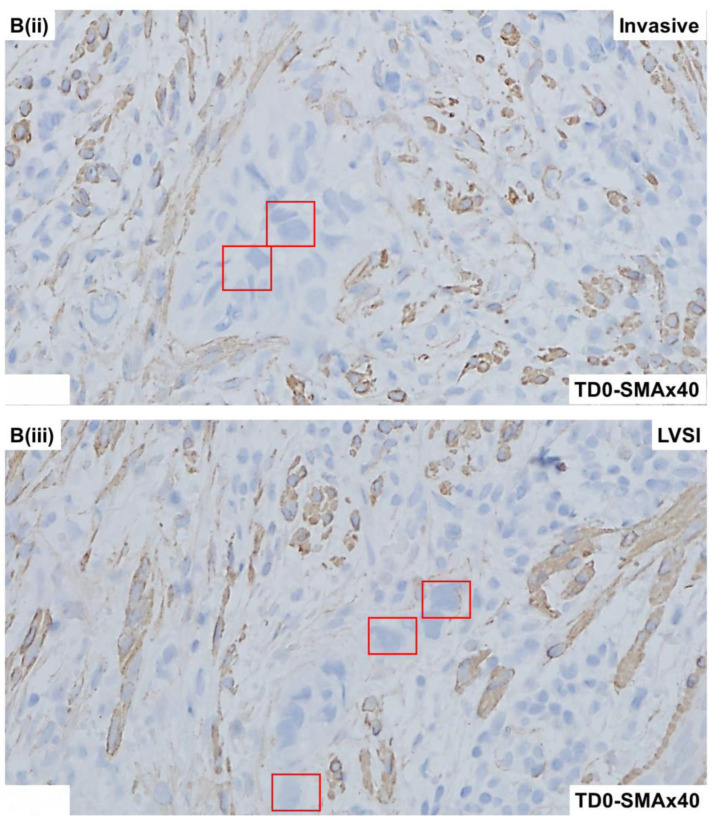 Figure 18
Figure 18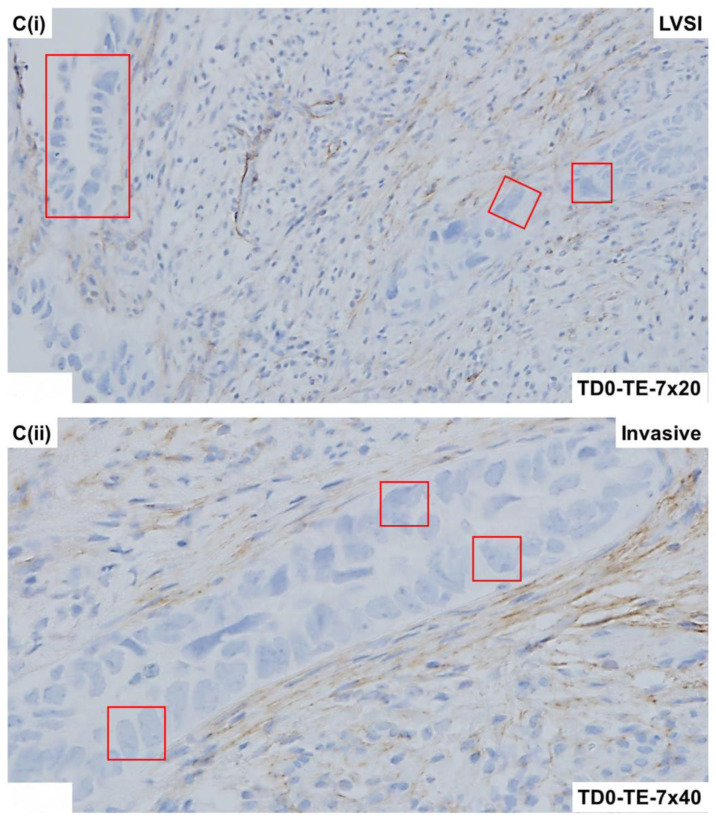 Figure 19
Figure 19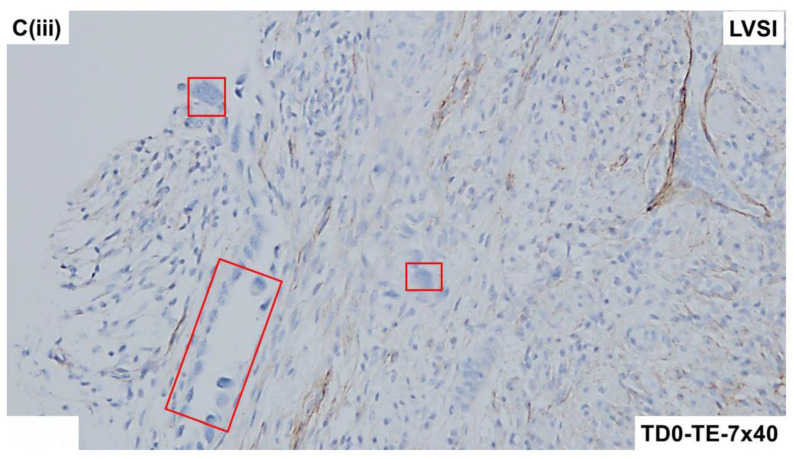 Figure 20
Figure 20- —Avera Cancer Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Ovarian cancer diagnosis and treatment · Angiogenesis and VEGF in Cancer
1. Introduction
Lymphovascular space invasion (LVSI), histological grade, and myometrial invasion are important prognostic factors of endometrial carcinoma, one of the most frequent gynecological cancers in developed countries [1]. LVSI, found in up to 35% of patients with endometrial cancers [2], is pathologically defined as the detection of tumoral cells in lymphatics or small vessels outside the core tumor. LVSI is characterized by the tumor cells within endothelium-lined spaces around the primary tumor that are observed as “free-floating” cell clusters, which frequently fit the space shape.
Uterine serous carcinoma is an uncommon form of endometrial cancer [3]. Serous carcinoma is the prototype of type-II endometrial cancer and accounts for 10% of all endometrial carcinomas; although rare, they are very aggressive tumors and are regarded as high-grade [4]. Despite its rarity, uterine serous carcinoma accounts for a disproportionate number of endometrial cancer deaths (estimated at approximately 40%; see [5]). The poor clinical outcomes for patients are attributable, in part, to an increased risk for occult metastases as compared to endometrioid endometrial carcinoma (See [4]).
The significance of LVSI in uterine serous carcinoma is recognized [6]. The presence and extent of LVSI and cervical stromal invasion are reported predictors for lymph node metastasis in uterine serous carcinoma [7].
In this case study, we have built a cellular atlas of LVSI in HGS-invasive endometrial adenocarcinoma. In this effort, we have used six types of marker-based characterization of the tumor compartment and cells of the tumor microenvironment (TME), including epithelial markers, LCA (leukocyte common antigen) markers, proliferation markers, apoptosis markers, immune cell markers, and fibroblast (mesenchyme) markers.
2. Patient Information and Consent
A 67-year-old female patient with invasive high-grade serous endometrial adenocarcinoma with no history of chemotherapies, undergoing surgical procedure of hysterectomy, BSO, and SLN dissection in 2021 consented to the ex vivo study as approved by the Avera IRB. The patient’s CA125 was 18.7 two weeks prior to the surgery.
2.1. Pathology
The final diagnosis was performed by a pathologist from the routine H and E (Hematoxylin and Eosin)-stained FFPE (Formalin-Fixed Paraffin-Embedded) sections from the resected tissues: hysterectomy, bilateral salpingo-oophorectomy, and sentinel and non-sentinel lymph node sampling and omentectomy. Invasive high-grade serous endometrial adenocarcinoma with deep myometrial invasion (87% of the uterine wall; depth of myometrial invasion was 19 mm of 22 mm uterine wall thickness) and lymphovascular space invasion was reported. There was a focal extension of carcinoma into the cervical stroma only; and the cervical and parametrial margins were free of malignancy. The serosa, fallopian tubes, and ovaries were intact and univloved. The sentinel lymph nodes (right external iliac, one lymph node; left obturator, two lymph nodes; and left pelvic, two lymph nodes) were free of malignancy. The periaortic non-sentinel lymph nodes showed micrometastatic carcinoma involving one of three lymph nodes. Very focal lymphovascular invasion is seen in the form of small clusters of tumor cells within delicate vascular spaced with identifiable endothelial cells recognized on routine H and E-stained sections. With these findings, the tumor was pathologically staged as pT2 p(sn)N2mi (AJCC 8th Edition).
2.2. Genomics
Serous uterine carcinomas are a limited feature of any known hereditary cancer syndrome [4]. This study evaluated the familial risk of cancers for patients with serous uterine carcinoma, focusing on Lynch syndrome malignancies, and identified a significant excess of ovarian and endometrial cancers in relatives of patients with endometrial cancer with pure serous and mixed serous tumors based on detailed three-generation family history data and medical record confirmation of malignancies in a single-institution cohort [4]. An IHC (ImmunoHistochemistry) ancillary test for MMR (Mis-Matched Repair) was performed. Ventana monoclonal antibodies against MSH2 (clone G219-1129), PMS2 (clone A 16-4), MLH 1 (clone M 1), and MSH6 (clone SP93) were evaluated. MLH1, MSH2, MSH6, and PMS2 were normal (intact nuclear expression), indicating an MMR-proficient tumor. BRCA germline mutations in women with uterine serous carcinoma are a topic of debate [8]. BRCA 1/2 Analyses with CustoinNext-Cancer^®^ +RNA/nsight^®^ showed no pathogenic mutations, variants of unknown significance, gross deletions or duplications, and no clinically relevant aberrant RNA transcripts.
2.3. Tissue Collection at the Time of Surgery
All experimental protocols were approved by the institutional and/or licensing committee(s). Informed consent (IRB approved: Protocol Number Study: 2017.053-100399_ExVivo001) was obtained from the patient. The resected tumor tissue from the patient was collected during a surgical procedure (total hysterectomy and bilateral salpingo-oophorectomy) in designated collection media as per the guidelines and relevant regulations provided by the pathologist.
2.4. Immunohistological Marker-Based Characterization of Tumor and TME Compartments
Tumor cells and cells of TME around LVSI were characterized using immunological markers, including epithelial markers, LCA markers, proliferation markers, apoptosis markers, immune cell markers, and fibroblast (mesenchyme) markers. Morphological and immunohistological staining of the FFPE sections from the resected tumor tissue was performed, as mentioned earlier [9]. In short, IHC expression of PD-L1(22C3; Dako # M3653) and PD-1 (ABCAM # ab137132) was carried out on FFPE sections from the tumor by double stain. All IHC expression of PD-L1 and PD-1 was performed on resected tissues, which were processed within an hour of surgery to preserve different types of cells, including tumor cells and cells of the TME. Tumor samples were tested for the IHC expression of CD3 (Anti-CD3 [SP7] ab16669), CD4 ([EPR6855] ab133616), CD8 (ab85792), CD68 (Dako. #M0876), CD163 (Cell Signaling #93498), FoxP3 ([236A/E7] ab20034) in immune cells and PD-L1 (Clone 22C3; Dako. #M3653) in tumor cells and tumor-associated macrophages. The IHC expression of EpCAM, CD45, CK 8, 18, S100A4, SMA, TE-7, Ki-67, cleaved-PARP, cleaved-caspase3, CD3, CD4, CD8, CD56, CD68, CD163, IL12R-B2, and FoxP3 and PD-L1 from the tumor was carried out on FFPE sections. The IHC detection kits were procured from Dako (Envision+ Dual-link system-HRP (DAB+), code K4065; Envision GI2 Doublestain system, Rabbit/Mouse (DAB+/Permanent Red), code K5361), and Abcam (ab210059 DoubleStain IHC Kit: M&R on human tissue (DAB and AP/Red). The validation of the protein expression was carried out in FFPEs of tonsil and tumor tissues. A board-certified pathologist evaluated the staining intensity and distribution pattern of expression of proteins by applying the standard scoring protocol and guidelines using a standard scoring system. Table 1 presents the list of markers included in the case study.
2.5. Expression of Immuno-Histological Markers in Tumor Cells and Cells of TME Compartments
Morphologically, the tumor demonstrated marked nuclear atypia, solid growth, and mitotic bodies. Figure 1 presents the LVSI in the resected tumor sample showing characteristic histopathological features of high-grade serous adenocarcinoma of endometrium by H&E. The invasive nature of the histology (Figure 1A) and the invasive tumor into the myometrium (Figure 1B) is observed along with a representative LVSI (Figure 1C). We tested the epithelial and leucocyte common antigen (LCA) marker expressions in cells around LVSI in the resected tumor sample, as seen in Figure 2.
The invasive nature of the histology of the tumor cells positive for CK8,18 and negative for CD45 as double stained with CK8,18 and CD45 is presented (Figure 2A,B). Epithelial tumor cells were negative for CD45 (alkaline phosphatase stain in pink) and positive for CK 8,18 (DAB stain in brown). The invasive tumor cells of the LVSI (Figure 2C,D) with membranous EpCAM positivity are presented. We stained the tumor sample with proliferation and apoptosis markers around LVSI, as shown in Figure 3. Epithelial tumor cells were found to be mostly negative for apoptosis markers, cleaved caspase3 (alkaline phosphatase stain in pink), and cleaved PARP (DAB stain in brown), while strongly nuclear positive for the proliferation marker, Ki67 (DAB stain in brown). The invasive tumor cells were found to be positive for Ki67 with rare positivity for cleaved caspase3 as stained simultaneously with Ki67 and cleaved caspase3 double stain (Figure 3A). In contrast, the invasive tumor cells of the LVSI (Figure 2B) were rarely stained with cleaved PARP. Figure 4 shows the immune cell marker expressions around the LVSI. The invasive nature of the histology of the non-tumor cells and tumor cells of the LVSI were demonstrated with CD3 (Figure 4A(i,ii)), CD4 (Figure 4B(i,ii)), CD8 (Figure 4C(i,ii)), CD56 (Figure 4D(i–iii)), CD68 (Figure 4E(i,ii)), CD163 (Figure 4F(i,ii)), FoxP3 (Figure 4G(i,ii)), IL-12RB2 (Figure 4H(i,ii)), and PD-1 and PD-L1 double stain (Figure 4I(i,ii)). Epithelial tumor cells were found negative for TIL markers, macrophage markers, and PD-1. Tumor cells of LVSI were positive for the pro-inflammatory marker, IL-12RB2. TILs were positive for PD-1 (alkaline phosphatase stain in pink) and PD-L1 (DAB stain in brown) in double stain. Immune cell marker expressions in the T-cells were membranous. Finally, the fibroblastic and tumor mesenchyme marker expressions demonstrated the fibroblastic nature of the TME mesenchyme in cells around LVSI (Figure 5). The invasive nature of the histology and the invasive tumor cells of the LVSI were stained with S100A4 Figure 5A(i–iii), SMA Figure 5B(ii,iii), and TE-7 Figure 5C(i–iii) single IHC stains (DAB stain in brown). Epithelial tumor cells were found to be mostly positive for S100A4, although the intensity of the stain varied between tumor cells. In contrast, both SMA and TE-7 were expressed in mesenchyme cells. The tumor cells were negative for SMA and TE-7.
3. Discussion
As LVSI has been recognized as one of the initial events in the lymphomatous and hematogenous metastases in endometrial carcinoma [3], LVSI is associated with lower overall survival, higher risk of recurrence, lymph node metastasis, and distant metastasis that LVSI correlates with poorer prognosis in endometrial cancers of FIGO stage I–III. The LVSI is associated with higher histologic grade and deep MMI and is considered an independent poor prognostic factor in endometrial carcinoma [10]. We observed no histomorphologic differences in the LVSI features among endometrial adenocarcinoma subtypes. Recently, LVSI in endometrial carcinoma has been known to be a prognostic factor independent of molecular signature [11]. The deep myometrial invasion correlates to positive LVSI, positive LNM, cancer recurrence, and poor OS for endometrial cancer patients [12]. Due to the high frequency of hematogenous dissemination in patients with serous carcinoma, LVSI is the primary feature of the dissemination. Here, we studied the cellular characterization of LVSI in a case of high-grade (3) and stage (IIIC2) invasive serous adenocarcinoma patients. Since we studied the LVSI, we also tested the patient’s blood for circulating tumor cells (CTCs) and circulating cancer-associated macrophage-like cells (CAMLs) on the day of the surgery. Although IHC can aid in the identification of LVSI in difficult or challenging cases, keeping in mind the histopathological features of our case, in line with other reports [13,14], we used standard H&E to aid in the diagnosis of LVSI in our case. As mentioned earlier, CTC and CAMLs were identified in our laboratory [15,16]. The patient’s blood was positive for both CTC and CAMLs.
Our study demonstrates, for the first time, that the tumor cells within LVSI were positive for IL-12R-B2 and S100A4. As an ideal example of cancer associated with epithelial–mesenchymal transition (EMT), which exhibits cancer stem cell (CSC)-like traits, uterine carcinosarcoma, more specifically, a high-grade form exhibiting LVSI, demands an in-depth understanding of the expression of EMT markers, like S100A4. S100A4 is a well-established tumor metastasis mediator in endometrial cancers, and estrogen-related receptor γ knockdown transcriptionally inhibits S100A4 expression to promote the expression of its downstream target E-cadherin, and vice versa [17]. Although S100A4 is a known inducer of EMT in uterine tumorigenesis [18], little is known about its involvement in LVSI and its differentiation. In a cell line-based study, Tochimoto et al. reported that cell lines stably overexpressing S100A4 enhanced CSC properties and decreased cell proliferation and acceleration of cell migration [19]. In their clinical samples, the S100A4 score was found to be significantly higher in sarcomatous as compared with carcinomatous components and was positively correlated with ALDH1, Slug, and vimentin scores and inversely with Ki-67-labeling indices. The study suggested the involvement of a S100A4-related signaling cascade, although initiated in the carcinomatous tumor components, to the establishment of EMT properties but can be a part of the event toward a divergent sarcomatous differentiation. The presence of LVSI indicates that the tumor is histopathologically predisposed to metastatic progression. S100A4 is known for its role in a number of cellular processes, including cell-cycle progression and metastasis. Hence, it is logical to argue that the S100A4 positivity of tumor cells in the LVSI is associated with poor prognosis. Our study demonstrates, for the first time, that the tumor cells within LVSI were positive for S100A4, highlighting its role as a promising prognostic marker in endometrial adenocarcinoma, especially in high-grade LVSI form.
The endometrial cancer (EC) cells in the LVSI in our study appeared to be positive with S100A4 IHC signal. S100A4 has been thought of as a crucial EMT mediator since the Wnt/B-catenin signaling pathway directly controls it, more specifically in the context of addressing the activation of the Wnt/B-catenin pathway in a diverse landscape of endometrial carcinogenesis [20]. Studies have reported that S100A4 promotes endometrial cancer progress through epithelial–mesenchymal transition regulation [18]. S100A4 promoted the migration and invasion capacity of EC cells via EMT modification. In their study, Hua et al. reported that an aberrant S100A4 expression may predict EC progression and play an important role in regulating EC cell invasion through EMT regulation, indicating that S100A4 is a promising therapeutic target. Although a future confirmation is warranted, it is very likely that the tumor cells are undergoing EMT.
When a tumor undergoes EMT, it is presumed that the intrinsic tumor-suppressor mechanisms have failed, and hence, it is understood that the CSCs experience extrinsic pressure from tumor-infiltrating lymphocytes (TILs) [21,22]. As various TILs interact with secreted cytokines in the tumor microenvironment and typically either kill tumors at early stages or promote tumors at advanced stages, CSCs and TILs form the “three-E” sequential cancer immunoediting phases: elimination, equilibrium, and escape [21,22,23,24]. Although intrinsic mechanisms of epigenetic immunoediting for IL-12-RB2 are not clear, IL-12-RB2 regulates both the number and functional maturity of regulatory T cells. IL-12RB2 is a part of homeostasis within the tumor cells and TILs, and this homeostasis affects prognosis [25]. Our results show that the granular cytoplasmic expression of IL-12-B2 was found in tumor cells uniformly in both regions of invasion and LVSI. However, the degree of expression was much lesser than that of the highly positive TILs. Pan-cancer data also show a limited expression of IL-12-RB2 in endometrial tumor cells as compared to other solid tumors, namely melanoma, breast, kidney, and colorectal cancers. Our data warrant further studies to understand the prognostic significance of IL-12-B2 expression in endometrial cancers.
4. Conclusions
Our case study demonstrates the characteristics of tumor cells and cells of TME around LVSI in a rare yet aggressive form of endometrial adenocarcinoma. Epithelial tumor cells of an aggressive disease enforce several pro-metastatic event(s), including LVSI, via direct and indirect crosstalk with the immune and fibroblastic/mesenchymal stromal cells of TME. This study demonstrates, for the first time, that the tumor cells within LVSI are positive for IL-12R-B2 and S100A4.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel R.L. Miller K.D. Fuchs H.E. Jemal A. Cancer statistics, 2022 CA Cancer J. Clin.20227273310.3322/caac.2170835020204 · doi ↗ · pubmed ↗
- 2Tortorella L. Restaino S. Zannoni G.F. Vizzielli G. Chiantera V. Cappuccio S. Gioe A. La Fera E. Dinoi G. Angelico G. Substantial lymph-vascular space invasion (LVSI) as predictor of distant relapse and poor prognosis in low-risk early-stage endometrial cancer J. Gynecol. Oncol.202132 e 1110.3802/jgo.2021.32.e 1133470061 PMC 7930448 · doi ↗ · pubmed ↗
- 3Bogani G. Ray-Coquard I. Concin N. Ngoi N.Y.L. Morice P. Enomoto T. Takehara K. Denys H. Nout R.A. Lorusso D. Uterine serous carcinoma Gynecol. Oncol.202116222623410.1016/j.ygyno.2021.04.02933934848 PMC 9445918 · doi ↗ · pubmed ↗
- 4Dewdney S.B. Kizer N.T. Andaya A.A. Babb S.A. Luo J. Mutch D.G. Schmidt A.P. Brinton L.A. Broaddus R.R. Ramirez N.C. Uterine serous carcinoma: Increased familial risk for lynch-associated malignancies Cancer Prev. Res.2012543544310.1158/1940-6207.CAPR-11-049922246618 PMC 3294192 · doi ↗ · pubmed ↗
- 5Moore K.N. Fader A.N. Uterine papillary serous carcinoma Clin. Obstet. Gynecol.20115427829110.1097/GRF.0b 013e 318218 c 75521508697 · doi ↗ · pubmed ↗
- 6Winer I. Ahmed Q.F. Mert I. Bandyopadhyay S. Cote M. Munkarah A.R. Hussein Y. Al-Wahab Z. Elshaikh M.A. Alosh B. Significance of lymphovascular space invasion in uterine serous carcinoma: What matters more; extent or presence?Int. J. Gynecol. Pathol.201534475610.1097/PGP.000000000000011325473753 · doi ↗ · pubmed ↗
- 7Qian Y. Pollom E.L. Nwachukwu C. Seiger K. von Eyben R. Folkins A.K. Kidd E.A. Extent of lymphovascular space invasion may predict lymph node metastasis in uterine serous carcinoma Gynecol. Oncol.2017147242910.1016/j.ygyno.2017.07.11928709703 PMC 5605436 · doi ↗ · pubmed ↗
- 8Lavie O. Ben-Arie A. Segev Y. Faro J. Barak F. Haya N. Auslender R. Gemer O. BRCA germline mutations in women with uterine serous carcinoma—Still a debate Int. J. Gynecol. Cancer 201020153115342111936810.1111/IGC.0b 013e 3181 cd 242f · doi ↗ · pubmed ↗