Situation, Education, Innovation, and Recommendation: A Large-Scale Systematic Review of Advance Care Planning in the Age of COVID-19
Thomas Mayers, Ayaka Sakamoto, Ryota Inokuchi, Kyoko Hanari, Huijun Z. Ring, Nanako Tamiya

TL;DR
This paper reviews how the COVID-19 pandemic affected advance care planning, identifying key barriers and facilitators to help improve future strategies.
Contribution
The study provides a large-scale systematic review of ACP during the pandemic, highlighting novel barriers and facilitators specific to this context.
Findings
Social distancing and technological barriers were the most common obstacles to ACP during the pandemic.
Telehealth platforms and clinician training were the most effective facilitators for ACP implementation.
The study identified 115 relevant studies, offering insights into ACP across diverse populations and contexts.
Abstract
The COVID-19 pandemic highlighted the need for advance care planning (ACP) as a way to help mitigate the various care concerns that accompanied the healthcare crisis. However, unique obstacles to typical ACP practice necessitated the need for guidance and innovation to help facilitate these vital conversations. The aim of this systematic review was to identify the various ACP barriers and facilitators that arose during the pandemic and determine how ACP practice was affected across different contexts and among different populations. This systematic review (PROSPERO registration number: CRD42022359092), which adheres to the PRISMA guidelines for reporting systematic reviews, examined studies on ACP in the context of the COVID-19 pandemic. The review involved searches of five databases, including MEDLINE and Embase. Of the 843 identified studies, 115 met the inclusion criteria. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
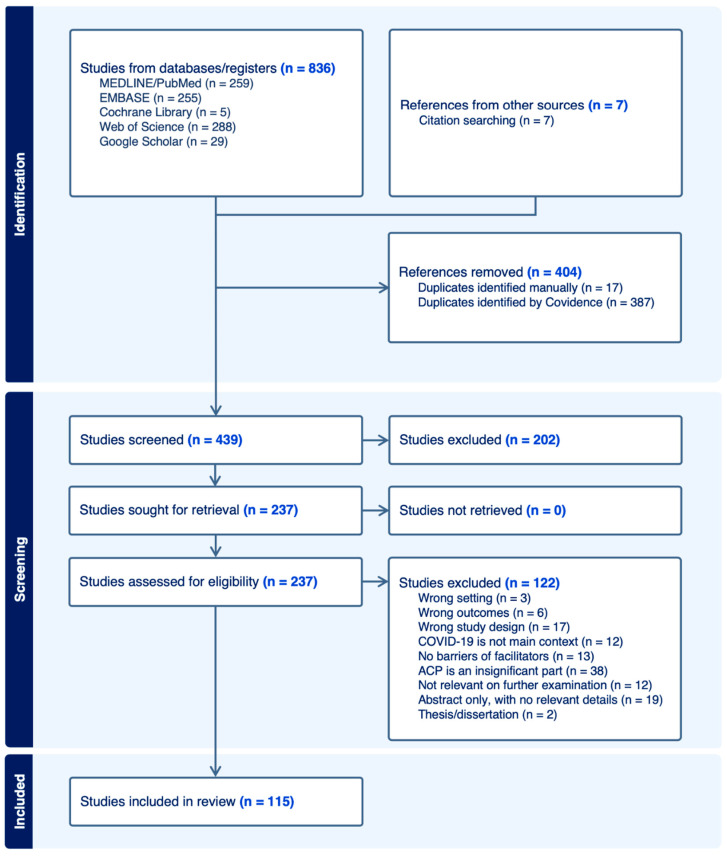 Figure 1
Figure 1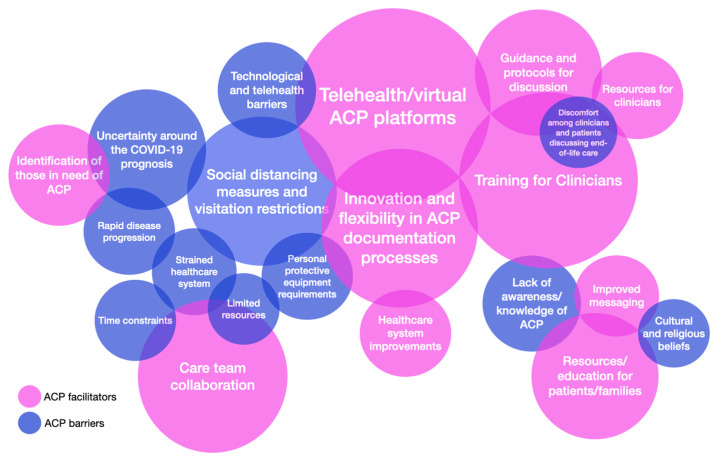 Figure 2
Figure 2| Study ID | Country | Setting | Population | Number of Participants | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|---|---|---|
| Mota Romero 2022 [ | SP | NH | HP | 20 |
| Barriers: Lack of awareness/knowledge of ACP |
| Statler 2022 [ | US | HO | PT | 356 |
| Barriers: Legal concerns; Uncertainty surrounding the COVID-19 prognosis; Limited resources; Healthcare system barriers; Discomfort among clinicians and patients discussing end-of-life care |
| Porteny 2022 [ | US | HO | PT | 76 |
| Barriers: Social distancing measures and visitation restrictions |
| Epler 2022 [ | US | HO | PT | 720 |
| Barriers: Discomfort among clinicians and patients discussing end-of-life care; Familial disagreement; Time constraints; Rapid disease progression |
| Kaehr 2022 * [ | US | NH | HP | 17 |
| Barriers: Personal protective equipment requirements; Social distancing measures and visitation restrictions; Uncertainty surrounding the COVID-19 prognosis |
| Sun 2022 [ | US | HO | PT | 276 |
| Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements; Strained healthcare system; Uncertainty surrounding the COVID-19 prognosis |
| Barnato 2022 [ | US | ED | PT | 5394 |
| Facilitators: Diagnosis of dementia |
| Ter Brugge 2022 [ | NL | NH | HP | 127 |
| Barriers: Social distancing measures and visitation restrictions |
| Perumalswami 2022 [ | US | HO | HP | 22 |
| Barriers: Technological/telehealth barriers |
| Jayes 2022 [ | UK | HO, NH | HP | 107 |
| Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements; Time constraints |
| Janssen 2021 [ | NL | HO | PT |
| Barriers: Uncertainty surrounding the COVID-19 prognosis; Time constraints; Negative perceptions about advance care planning | |
| Brophy 2021 [ | US | SV | PB | 522 |
| Barriers: Emotional barriers |
| Piers 2021 [ | BL | HO | PT | 711 |
| Facilitators: ACP/palliative care experts: co-management by geriatricians |
| Bradshaw 2021 [ | UK | NH | HP | 277 |
| Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements; Strained healthcare system; Rapid disease progression; Emotional barriers; Uncertainty surrounding the COVID-19 prognosis |
| Dujardin 2021 [ | NL | HO | HP | 15 |
| Barriers: Uncertainty surrounding the COVID-19 prognosis; Discomfort among clinicians and patients discussing end-of-life care; Technological/telehealth barriers; Social distancing measures and visitation restrictions; Time constraints; Healthcare system barriers |
| Connellan 2021 [ | IR | ED | PT | 430 |
| Facilitators: Understanding/fear of COVID-19 |
| Vellani 2021 [ | CN | NH | HP | 14 |
| Facilitators: ACP/palliative care experts; Telehealth/virtual ACP platforms; Care team collaboration; Proactive ACP Conversations |
| Toccafondi 2021 * [ | IT | HO | PT | 110 |
| Facilitators: Guidance and protocols for ACP discussions |
| DeGette 2021 * [ | US | HO | PT | 258 |
| Barriers: Personal protective equipment requirements; Social distancing measures and visitation restrictions; Uncertainty surrounding the COVID-19 prognosis; Racial and ethnic barriers |
| Copley 2021 [ | UK | HO | PT | 164 |
| Facilitators: Resources for clinicians; Understanding/fear of COVID-19; Public awareness of ACP; Resources/education for patients/families |
| Lin 2021 [ | TW | HO | PT | 2493 |
| Barriers: Social distancing measures and visitation restrictions; Lack of awareness/knowledge of ACP; Healthcare system barriers; Limited resources; Legal concerns; Discomfort among clinician and patients discussing end-of-life care; Time constraints; Strained healthcare system |
| Ye 2021 [ | US | NH | PT | 963 |
| Barriers: Social distancing measures and visitation restrictions |
| Huayanay 2021 [ | US | HO | PT | 1 |
| Barriers: Communication difficulties; Cultural and religious beliefs; Financial concerns |
| Nguyen 2021 [ | US | SV | PT | 100 |
| Facilitators: Public awareness of ACP; Improved messaging |
| Coles 2020 * [ | UK | NH | HP |
| Facilitators: Care team collaboration; ACP/palliative care experts; Healthcare system improvements | |
| Wei 2020 [ | US | HO | HP |
| Barriers: Rapid disease progression; Social distancing measures and visitation restrictions | |
| Maia 2020 * [ | PO | HO | PT | 51 |
| Barriers: Personal protective equipment requirements; Social distancing measures and visitation restrictions; Strained healthcare system; Technological/telehealth barriers |
| Hendriks 2022 [ | NL | HO | PT | 275 |
| Facilitators: Training for clinicians; Resources for clinicians |
| Holdsworth L.M. 2022 [ | US | HO | HP | 15 |
| Barriers: Technological/telehealth barriers; Social distancing measures and visitation restrictions |
| Dassel 2021 [ | US | HC | FC | 82 |
| Barriers: Emotional barriers; Social distancing measures and visitation restrictions; Lack of awareness/knowledge of ACP |
| de Vries 2021 [ | CN | SV | PB | 3923 |
| Barriers: Distrust in the healthcare system |
| Payne 2022 [ | US | ED | PB | 50 |
| Barriers: Lack of awareness/knowledge of ACP |
| Ninteau 2022 [ | US | NH | HP | 7 |
| Barriers: Social distancing measures and visitation restrictions |
| Elizondo 2022 * [ | AR | HO | PT |
| Facilitators: Care team collaboration; Innovation and flexibility in ACP documentation processes; Healthcare system improvements | |
| Hafid 2022 * [ | CN | HO | HP | 48 |
| Facilitators: Public awareness of ACP; Resources/education for patients/families; Telehealth/virtual ACP platforms |
| Study ID | Country | Setting | Population | No. of Participants | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|---|---|---|
| van de Wiel 2022 [ | BL | AC | MS | 172 |
| Facilitators: Training for clinicians |
| Casey 2022 [ | US | HO | PT | 143 |
| Facilitators: Training for clinicians; Guidance and protocols for ACP discussions; Innovation and flexibility in ACP documentation processes |
| Cousins 2022 [ | UK | NH | HP, FM | 54 |
| Facilitators: Resources/education for patients/families; Resources for clinicians; Training for clinicians |
| Rosedale 2022 * [ | US | HO | PT |
| Facilitators: Training for clinicians; ACP/palliative care experts | |
| Rabow 2021 [ | US | OT | HP |
| Facilitators: Training for clinicians; Resources for clinicians | |
| Oulton 2021 [ | US | HO | HP | 9 |
| Facilitators: Training for clinicians |
| Budidi 2021 * [ | US | AC | HP | 30 |
| Barriers: Time constraints; Low education level; Communication difficulties; Technological/telehealth barriers; Lack of adequate ACP training for clinicians |
| Price 2021 * [ | US | HO | PT | 143 |
| Facilitators: Training for clinicians |
| Roberts 2020 [ | US | AC | HP |
| Facilitators: Training for clinicians | |
| Markwalter 2022 * [ | US | HO | PT | 143 |
| Facilitators: Training for clinicians; Resources for clinicians |
| Preston 2022 * [ | UK | NH | HP, NH, FM |
| Barriers: Technological/telehealth barriers | |
| Cooney 2022 [ | US | AC | MS | 83 |
| Facilitators: Training for clinicians |
| Holdsworth 2022 * [ | UK | HO | PT | 69 |
| Facilitators: Training for clinicians; Identification of those in need of ACP; Guidance and protocols for ACP discussions |
| Volandes 2022 [ | US | HO | PT | 14107 |
| Facilitators: Resources/education for patients/families; Training for clinicians |
| Mills 2021 [ | US | HO | HP | 48 |
| Facilitators: Telehealth/virtual ACP platforms |
| Varey 2021 * [ | UK | OT | HP, PT, FM |
| Facilitators: Resources/education for patients/families | |
| Phenwan 2021 [ | TL | OT | MS, HP, PB | 103 |
| Barriers: Cultural and religious beliefs; Lack of awareness/knowledge of ACP |
| Berning 2021 [ | US | NH | PT | 581 |
| Facilitators: Care team collaboration; Identification of those in need of ACP; Guidance and protocols for ACP discussions |
| Dobert 2021 * [ | US | NH | HP |
| Facilitators: Care team collaboration; Training for clinicians; Improved messaging; Resources for clinicians; Telehealth/virtual ACP platforms | |
| Smith 2020 [ | US | OT | PT | 413 |
| Facilitators: Training for clinicians |
| McAfee 2022 [ | US | AC | PB, HP |
| Barriers: Cultural and religious beliefs; Racial and ethnic barriers; Healthcare system barriers; Lack of awareness/knowledge of ACP; Low health literacy; Limited resources: accessibility to health directives | |
| Huang 2021 [ | US | HO | HP |
| Barriers: Discomfort among clinicians and patients discussing end-of-life care; Lack of adequate ACP training for clinicians |
| Study ID | Country | Setting | Population | No. of Participants | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|---|---|---|
| Finger 2022 [ | US | NH | PT | 24 |
| Barriers: Social distancing measures and visitation restrictions; Strained healthcare system |
| Hannon 2022 * [ | CN | NH, HO | PT | 26 |
| Facilitators: Telehealth/virtual ACP platforms |
| Hui 2022 * [ | US | HO | PT | 12,941 |
| Facilitators: Guidance and protocols for ACP discussions; Identification of those in need of ACP; Care team collaboration; Training for clinicians; Healthcare system improvements |
| Zhukovsky 2022 * [ | US | HO | PT | 76 |
| Facilitators: Care team collaboration |
| Gessling 2022 * [ | US | OT | PT | 294 |
| Facilitators: Telehealth/virtual ACP platforms; Care team collaboration |
| Vellani 2022 [ | CN | HO | PT | 21 dyads |
| Barriers: Emotional barriers |
| Yen 2022 [ | TW | HO | PT | 897 |
| Barriers: Uncertainty surrounding the COVID-19 prognosis; Limited resources |
| Liberman 2022 [ | US | HO | PT | 64 |
| Facilitators: Telehealth/virtual ACP platforms; ACP/palliative care experts |
| Meyers 2022 * [ | US | OT | VT | 106 |
| Barriers: Social distancing measures and visitation restrictions |
| Yourman 2022 * [ | US | HO | PT | 53 |
| Facilitators: Training for clinicians; Telehealth/virtual ACP platforms |
| MacInnes 2022 * [ | UK | OT | HP |
| Facilitators: Telehealth/virtual ACP platforms | |
| Allen 2021 * [ | UK | OT | PT, HP, PB |
| Facilitators: Resources for clinicians | |
| Acevedo Rodriguez 2021 * [ | US | OT | VT | 500 |
| Facilitators: Telehealth/virtual ACP platforms |
| Singh 2021 [ | US | HO | PT |
| Facilitators: Care team collaboration; Healthcare system improvements | |
| Nandhra 2021 * [ | UK | NH | PT | 585 |
| Facilitators: Identification of those in need of ACP; ACP/palliative care experts |
| Paladino 2021 [ | US | HO | HP |
| Facilitators: Guidance and protocols for ACP discussions | |
| Lin 2020 [ | US | ED | HP |
| Barriers: Social distancing measures and visitation restrictions | |
| Handalage 2020 * [ | UK | OT | PT | 160 |
| Facilitators: Resources for clinicians; ACP/palliative care experts |
| Schoenherr 2020 [ | US | HO | PT | 29 |
| Barriers: Social distancing measures and visitation restrictions |
| Langmaid 2020 [ | US | OT | PT |
| Facilitators: Care team collaboration; Telehealth/virtual ACP platforms | |
| Gaur 2020 [ | US | NH | HP | 10 |
| Barriers: Social distancing measures and visitation restrictions |
| Bhatia 2021 [ | US | HO | PT | 356 |
| Barriers: Social distancing measures and visitation restrictions |
| Cavalier 2020 [ | US | HO | PT |
| Facilitators: Innovation and flexibility and in ACP documentation processes | |
| Janssen 2020 [ | NL | SV | HP | 68 |
| Facilitators: Proactive ACP conversations |
| Baharlou 2020 [ | US | OT | PT | 183 |
| Facilitators: Innovation and flexibility in ACP documentation processes; Understanding/fear of COVID-19; Healthcare system improvements; Care team collaboration; Training for clinicians; ACP/palliative care experts; Telehealth/virtual ACP platforms |
| McFarlane 2022 * [ | UK | ED | PB | 56,343 |
| Facilitators: Innovation and flexibility in ACP documentation processes |
| Mulyak 2021 * [ | UK | ED | PT | 107,614 |
| Facilitators: Innovation and flexibility in ACP documentation processes |
| Hurlow 2021 [ | UK | ED | PT |
| Facilitators: Innovation and flexibility in ACP documentation processes | |
| Funk 2020 [ | US | ED | PB |
| Facilitators: Telehealth/virtual ACP platforms; Innovation and flexibility in ACP documentation processes | |
| Portz 2020 [ | US | OT | PB | 3292 |
| Facilitators: Innovation and flexibility in ACP documentation processes; Resources/education for patients/families |
| Schifeling 2020 [ | US | OT | PT | 190 |
| Facilitators: Telehealth/virtual ACP platforms |
| Auriemma 2020 [ | US | OT | PT, FM |
| Facilitators: Resources/education for patients/families |
| Study ID | Country | Quality Assessment | ACP Barriers and Facilitators |
|---|---|---|---|
| Auriemma 2022 [ | US |
| Barriers: Social distancing measures and visitation restrictions; Technological/telehealth barriers; Uncertainty surrounding the COVID-19 prognosis; Negative perceptions about advance care planning; Distrust in the healthcare system; Racial and ethnic barriers |
| Back 2021 [ | US |
| Barriers: Lack of awareness/knowledge of ACP; Uncertainty surrounding the COVID-19 prognosis; Distrust in the healthcare system |
| Bender 2021 [ | US |
| Barriers: Time constraints; Limited resources; Healthcare system barriers; Discomfort among clinicians and patients discussing end-of-life care; Strained healthcare system; Personal protective equipment requirements |
| Block 2020 [ | US |
| Barriers: Legal concerns; Social distancing measures and visitation restrictions |
| Chan 2020 [ | UK |
| Barriers: Limited resources; Familial disagreement; Uncertainty surrounding the COVID-19 prognosis; Lack of awareness/knowledge of ACP; Social distancing measures and visitation restrictions |
| Chase 2020 [ | CN |
| Facilitators: Telehealth/virtual ACP platforms; Healthcare system improvements; Guidance and protocols for ACP discussions |
| Curtis 2020 [ | US |
| Barriers: Strained healthcare system |
| Dattolo 2021 [ | IT |
| Barriers: Social distancing measures and visitation restrictions |
| Dewhurst 2021 [ | UK |
| Facilitators: Proactive ACP Conversations |
| Farrell 2020 [ | US |
| Facilitators: Healthcare system improvements; Care team collaboration: teamwork/multi-disciplinary involvement; Telehealth/virtual ACP platforms; Identification of those in need of ACP |
| Gordon 2020 [ | UK |
| Barriers: Social distancing measures and visitation restrictions; Blanket approaches to ACP; Negative perceptions about advance care planning |
| Hill 2021 [ | UK |
| Barriers: Social distancing measures and visitation restrictions; Personal protective equipment requirements |
| Hopkins 2020 [ | UK |
| Barriers: Social distancing measures and visitation restrictions; Technological/telehealth barriers |
| Hughes 2021 [ | US |
| Barriers: Distrust in the healthcare system; Lack of awareness/knowledge of ACP |
| Janwadkar 2020 [ | US |
| Barriers: Limited resources; Time constraints; Rapid disease progression; Social distancing measures and visitation restrictions; Technological/telehealth barriers |
| Kuzuya 2020 [ | JP |
| Barriers: Social distancing measures and visitation restrictions; Rapid disease progression; Communication difficulties |
| Moorman 2021 [ | US |
| Barriers: Emotional barriers; Social distancing measures and visitation restrictions; Familial disagreement; Rapid disease progression; Financial concerns; Low education level; Racial and ethnic barriers; Strained healthcare system |
| Palipane 2021 [ | UK |
| Barriers: Rapid disease progression |
| Parekh de Campos 2021 [ | US |
| Barriers: Limited resources; Time constraints; Lack of adequate ACP training for clinicians; Cultural and religious beliefs |
| Parks 2021 [ | US |
| Barriers: Social distancing measures and visitation restrictions; Communication difficulties |
| Powell 2021 [ | US |
| Barriers: Social distancing measures and visitation restrictions |
| Sinclair 2020 [ | AU |
| Barriers: Personal protective equipment requirements |
| Swinford 2020 [ | US |
| Facilitators: Telehealth/virtual ACP platforms; Care team collaboration; Guidance and protocols for ACP discussions |
| Van Buren 2021 [ | US |
| Barriers: Family clustering of COVID-19; Social distancing measures and visitation restrictions |
| Wallace 2020 [ | US |
| Barriers: Rapid disease progression |
| Zaurova 2020 [ | US |
| Barriers: Strained healthcare system; Rapid disease progression; Uncertainty surrounding the COVID-19 prognosis |
- —Ministry of Health, Labour and Welfare
- —Health and Labor Sciences Research Grant, Japan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Asia Education and Culture
1. Introduction
The COVID-19 pandemic was most devastating, in many respects, for older adults; not only was the SARS-Covid-2 virus more deadly in this population, but the damage caused by the social isolation that many faced was profound [1,2,3,4,5,6,7,8]. For older adults and other vulnerable populations, the pandemic brought to the forefront the critical importance of advance care planning (ACP). ACP is a well-established and evidenced practice that helps to ensure the wishes of a person, regarding their medical care and treatment towards the end of life, are respected should they become unable to communicate those preferences and complex healthcare decisions need to be made [9,10,11,12]. The unprecedented nature of the COVID-19 pandemic; however, characterized by rapid disease progression [13,14], healthcare system overload [15,16], and constantly evolving clinical guidelines [17,18], has posed significant challenges to ACP. Conversely, the pandemic has also potentially acted as a catalyst for enhancing the awareness and implementation of ACP due to the heightened perception of health risks [19,20,21].
The importance of ACP in aging societies, such as Japan, cannot be overstated [22,23]. As the demographic structure shifts towards a higher proportion of elderly individuals, the burden on healthcare systems intensifies, accompanied by an increase in chronic illnesses and end-of-life care needs [24,25]—a burden further exacerbated by the COVID-19 pandemic. ACP can aid in reducing this burden on healthcare systems by promoting effective resource utilization and preventing unnecessary or unwanted medical interventions [9,10,26]. Moreover, ACP can foster better communication and understanding between healthcare providers, patients, and their families, leading to more coordinated and compassionate care [27,28]. This alignment of care with patient preferences is especially important in preserving the dignity and quality of life of older adults. Therefore, the implementation of ACP can not only address the practical aspects of healthcare delivery in an aging society but can also resonate deeply with the cultural and ethical values surrounding care for older adults [22,29]. Thus, in 2022, after the immediate crisis of the pandemic had passed, in response to a request from the Japanese Ministry of Health, Labour, and Welfare, we sought to investigate how ACP practice had been impacted. Following our previously published umbrella review [30], the purpose of this current study was to explore the following questions: How did the COVID-19 pandemic affect the practice of ACP? What obstacles or barriers did the COVID-19 pandemic create to the delivery of ACP? What trends occurred to facilitate ACP practice during the pandemic?
To comprehensively explore these questions, our research employed the systematic review methodology, which allowed for a thorough and structured examination of the existing literature, capturing a wide array of experiences and findings from different healthcare settings and populations affected by the COVID-19 pandemic. By synthesizing data from multiple studies, we aimed to identify common themes and granular, divergent, or unique findings regarding the facilitators and barriers to ACP during this global health crisis. Identifying the factors that have either hindered or aided ACP during this period is not only essential for developing effective strategies to promote ACP in similar situations in the future, but also for improving ACP’s delivery, accessibility, and acceptability in general. The insights gained from this systematic review are expected to inform healthcare policy and practice, contributing to more resilient and patient-centered healthcare systems.
2. Materials and Methods
2.1. Protocol and Registration
The protocol for this systematic review was registered with the PROSPERO International Prospective Register of Systematic Reviews system (registration number: CRD42022359092; https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022359092, accessed on 15 November 2023). This systematic review strictly adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [31]. Covidence systematic review software (with Extraction version 2.0, Veritas Health Innovation, Melbourne, Australia), which is widely used for conducting systematic reviews and acknowledged by Cochrane as the foremost tool for initial screening and data extraction in standard intervention reviews [32], was used for all data management, including the study selection and data extraction processes [32].
2.2. Information Sources
Using the identified search strategies (Box 1), potentially relevant papers were identified from five databases: MEDLINE/PubMed, Embase, Cochrane Central Register of Controlled Trials, Web of Science, and Google Scholar. The strategy also included manually checking the reference lists of included studies to identify any further relevant studies. The search was restricted to the literature from peer-reviewed journals, including conference abstracts, published in 2020 or later. The search was performed by two researchers (T.M. and H.R.).
Box 1Search strategy used for each database. 1. Embase (‘covid-19’:ab OR ‘covid-19’:ti OR ‘covid-19’:kw OR ‘novel coronavirus disease’:ab OR ‘novel coronavirus disease’:ti OR ‘novel coronavirus disease’:kw OR ‘sars-cov-2’:ab OR ‘sars-cov-2’:ti OR ‘sars-cov-2’:kw OR ‘severe acute respiratory syndrome coronavirus 2’:ab OR ‘severe acute respiratory syndrome coronavirus 2’:ti OR ‘severe acute respiratory syndrome coronavirus 2’:kw) AND (‘advance care planning’:ab OR ‘advance care planning’:ti OR ‘advance care planning’:kw OR ‘advance care directive’:ab OR ‘advance care directive’:ti OR ‘advance care directive’:kw OR ‘living will’:ab OR ‘living will’:ti OR ‘living will’:kw) AND [2020–2022]/py 2. MEDLINE/PubMed Search: (((((((COVID-19[Title/Abstract])) OR (novel coronavirus disease[Title/Abstract])) OR (SARS-CoV-2[Title/Abstract])) OR (severe acute respiratory syndrome coronavirus 2[Title/Abstract])) AND (advance care planning[Title/Abstract])) OR (advance care directive[Title/Abstract])) OR (living will[Title/Abstract]) Filters: Full text, from 2020 to 2022 3. Web of Science ((((((TS=(COVID-19)) OR TS=(“novel coronavirus disease”)) OR TS=(SARS-CoV-2)) OR TS=(“severe acute respiratory syndrome coronavirus 2”)) AND TS=(“advance care planning”)) OR TS=(“advance care directive”)) OR TS=(“living will”) 2020–2022 4. Google Scholar allintitle: “COVID 19” OR “novel coronavirus disease” OR “SARS CoV 2” OR “severe acute respiratory syndrome coronavirus 2” AND “advance care planning” OR “advance care directive” OR “living will” 5. Cochrane Library (“COVID 19” OR “novel coronavirus disease” OR “SARS CoV 2” OR “severe acute respiratory syndrome coronavirus 2”):ti,ab,kw AND (“advance care planning” OR “advance care directive” OR “living will”):ti,ab,kw
2.3. Study Selection
Covidence software was used for all aspects of the screening, data extraction, and quality assessment processes. Most duplicates were automatically removed by the Covidence software at the point of importing the studies; however, during the later screening process, some duplicate studies were further identified and removed manually. The titles and abstracts of the remaining citations were individually screened by two researchers (T.M. and A.S.). Irrelevant texts were excluded based on the following exclusion criteria: (1) not mentioning ACP (or other synonymous terms); (2) not mentioning the COVID-19 pandemic; (3) giving no indication of facilitators of or barriers to ACP; and (4) other reasons such as wrong setting, study design, etc. Review articles were excluded from the study but were used for manual citation searching for further relevant studies. Conflicting votes were resolved through discussion, before moving onto review of the full texts. Full text review was performed in the same manner by the same two researchers (T.M. and A.S.). An inter-rater reliability assessment was performed and extracted using the Covidence software.
2.4. Data Extraction
The data extraction form was created within the Covidence software. Data extraction was conducted according to the study characteristics. The extraction form contained the following items: study identification (ID), title, lead author, publication year, country in which the study was conducted, publication category, aim of study, study design, setting, population description, total number of participants, barriers, facilitators, increase or decrease in ACP during COVID-19 (Yes/No, value), and a summary of the main findings and implications/recommendations. Before beginning the data extraction process, the extraction form was tested on a number of studies and refined. During this process, four key categories emerged: (1) Situation—studies that described the situation regarding ACP practice; (2) Education—studies that described public- or professional-facing ACP-related educational programs/interventions; (3) Innovation—studies that described new ACP-related innovations; and (4) Recommendation—documents from experts or organizations that gave recommendations on ACP practice. Because of the large number of included studies, the data extraction process and quality assessment were conducted primarily by one researcher (T.M.) and were reviewed by another (A.S.), while collaborators oversaw all the data extraction processes. Data were exported from Covidence and presented as tables. The extracted data pertaining to the ACP barriers and facilitators were coded using a simple labeling system in which codes were assigned to categorize and quantify each barrier and facilitator.
2.5. Quality Appraisal
Quality assessment tools were created within the Covidence software. The Mixed Methods Appraisal Tool (MMAT) [33] was used for the assessment of qualitative and quantitative studies. Appraisal of nonrandomized trials assessed the following criteria: participant selection, outcome measures, outcome data, confounding factors, and intervention administration. Appraisal of quantitative descriptive studies assessed the following criteria: sampling strategy, study population, appropriateness of measures, nonresponse bias risk, and statistical analysis. Appraisal of randomized controlled trials assessed the following criteria: randomization methodology, group allocation, outcome data, blinding, and intervention adherence. For qualitative studies, assessment was made of the following criteria: methodology, data collection methods, derivation of the findings, data interpretation, and coherence between the data source, collection analysis, and interpretation. For studies that fell outside of the scope of MMAT assessment, such as letters, recommendations, reports, and guidelines, the AACODS checklist was used [34]. This tool, developed for appraisal of gray literature, gives the appraiser various questions to consider for probing and evaluating the authority, accuracy, coverage, objectivity, date, and significance of a study. Quality assessment data was exported from Covidence, synthesized, and presented visually in the tables using the following color-coded labeling system: red = low; orange = low-middle; yellow = high-middle; and green = high. Quality assessment data were not used to exclude studies.
3. Results
3.1. Overview of the Results
The search of the five databases yielded a total of 836 studies, and a search of citations yielded a further 7 studies. The Covidence software automatically removed 387 duplicate studies, and a further 17 were removed manually. Of the remaining 439 studies, 202 irrelevant studies were excluded after screening the titles and abstracts. The remaining 237 studies underwent full-text screening and were assessed for eligibility and a further 122 studies were excluded. Finally, 115 studies that met the inclusion criteria were included in the review. Cohen’s Kappa values of 0.557 and 0.559 for the title/abstract and full-text screening showed moderate agreement between the two reviewers. The PRISMA flowchart detailing the study selection process is presented in Figure 1.
Table 1 shows the characteristics of the included studies. These comprised 34 (29.6%) nonrandomized studies, 28 (24.3%) letters/opinions/editorials, 20 (17.4%) quantitative descriptive studies, 19 (16.3%) qualitative studies, 7 (6.1%) reports (including case reports), and 7 (6.1%) were of mixed methods. Of the 115 included studies, 31 (27.0%) were conference abstracts. The included studies came from 13 different counties (in alphabetical order): Argentina (n = 1, 0.9%), Australia (n = 1, 0.9%), Belgium (n = 2, 1.7%), Canada (n = 6, 5.2%), Ireland (n = 1, 0.9%), Italy (n = 2, 1.7%), Japan (n = 1, 0.9%), Portugal (n = 1, 0.9%), Spain (n = 1, 0.9%), Taiwan (n = 2, 1.7%), Thailand (n = 1, 0.9%), the Netherlands (n = 5, 4.3%), the United Kingdom (n = 21, 18.3%), and the United States (n = 70, 60.9%). A range of different settings were represented among the studies, with the most frequent being hospitals (n = 42, 36.5%; including clinics, emergency departments, etc.), nursing homes (n = 21, 18.3%; including long-term care facilities, residential homes, etc.), and online/telehealth (n = 15, 13.0%). Study participants were largely patient populations of various kinds (n = 58, 50.4%; including those with COVID-19, inpatients, outpatients, nursing home residents, diagnosed with dementia, etc.) and healthcare professionals (n = 34, 29.6%; including doctors, nurses, residents, nursing home staff, etc.).
3.2. ACP Barriers and Facilitators during the COVID-19 Pandemic
Table 2, Table 3, Table 4 and Table 5 show the included studies divided into the above-mentioned four categories as follows: Situation (n = 35; Table 2), Education (n = 22; Table 3), Innovation (n = 32; Table 4), and Recommendation (n = 26; Table 5). The tables focus on the barriers to and facilitators of ACP during the pandemic identified in each of the studies.
3.2.1. Situation Category
The 35 studies included in the Situation category are presented in Table 2. These studies primarily describe the situation of ACP practice during the COVID-19 pandemic across different settings and populations. Included in the Table is the Study ID (comprised of the first author’s surname and year of publication), country in which the study was conducted, study setting (hospital, nursing home, etc.) and population, number of participants (when available), quality assessment (color-coded system), and the coded barriers and facilitators. Further details for each study included in this category are available in Table S1.
Across the included studies within this “situation” category, one consistent theme was how the pandemic highlighted the need for improved communication and awareness among healthcare professionals, patients, and their families with regards to ACP. For example, the NUHELP program’s findings [35] and observations from nursing homes [39], healthcare providers [48], and general practitioners [49] all point to the need for ACP discussions and familiarity with ACP processes. A study by Porteny et al., described how clinicians perceived an increased patient willingness to discuss quality of life and ACP due to COVID-19, but patients reported minimal engagement in such discussions [37]. This discrepancy was further exacerbated by challenges such as PPE hindering communication [44], remote discussions [42], and disparities in ACP knowledge across different communities [57].
A study by Statler et al. found that documentation of ACP, including code status and end-of-life preferences, was notably low (22.8%) for hospitalized COVID-19 patients [36]. However, palliative care consultations showed a positive correlation with ACP documentation [36,40], indicating the role of such consultations in the ACP process. The pandemic spurred an earlier initiation of ACP conversations, often influenced by media coverage and public awareness [45], but the quality of these discussions varied, with telemedicine emerging as a key but imperfect tool [43,44]. The variability in treatment intensity for patients with dementia [41] and the challenges in involving patients in shared decision-making [62] suggest that provider biases and systemic issues in healthcare communication persist.
The response to these issues has been multifaceted. Some institutions have seen an increase in the use of telemedicine for ACP [69], while others have emphasized the importance of personalized ACP [59] and integrated palliative care [51]. Redeployment of specialists [60] and creative solutions to facilitate discussions and legal documentation [63] have been implemented to address the challenges posed by the pandemic. This underscores the need for ongoing education and a more compassionate approach to encourage ACP discussions [66], not just during crises but as a standard practice in healthcare.
3.2.2. Education Category
Table 3 shows the 22 studies included in the Education category (Table S2 gives further details on each study). These studies have a strong focus on ACP-related educational interventions that were aimed at practicing healthcare professionals, medical students, and patients and their family members.
Education interventions for ACP during the COVID-19 pandemic have proven crucial for both the public and healthcare professionals, as evidenced by a variety of studies within the “education” category [70,71,72,73,74,75]. Training programs have shown a positive impact on the confidence of healthcare providers and students in initiating ACP discussions and recognizing patient cues, despite the challenges presented by social distancing and the need for remote communication [72,84]. This training has led to revised ACP procedures and empowered families to partake in care decisions [80], highlighting the importance of ACP as an ongoing, iterative process that is highly individualized and extends beyond medical and end-of-life considerations [86].
Despite the reported advancements, disparities persist, with a higher percentage of white patients meeting ACP quality standards post-intervention compared to non-white patients [73]. One study suggested that the pandemic has underscored the need to integrate death education more broadly into teacher training and undergraduate curricula to address cultural taboos and educate the public on ACP [90]. Virtual interventions, like online workshops and telemedicine curricula, have broadened the reach and accessibility of ACP education, proving to be effective in engaging diverse audiences [89,91]. Narrative-based education [78], virtual training sessions [75], and electronic resources [85] have emerged as valuable methods to facilitate ACP-related decisions and discussions. Overall, these studies indicate that while the pandemic posed challenges, it also provided an opportunity to enhance the understanding and implementation of ACP through public- and professional-facing educational interventions, making it more accessible and relevant for a wider population.
3.2.3. Innovation Category
The Innovation category included 32 studies, which are presented in Table 4 (further details are giving in Table S3). These studies describe innovations that aided ACP practice and delivery during the pandemic.
The COVID-19 pandemic served as a catalyst for various innovations that led to increases in the engagement of patients in ACP [104,116,123]. The adoption of telehealth technologies and electronic platforms, such as eMOLST, facilitated this increase, allowing patients and families to discuss ACP remotely and ensure their care preferences are documented and respected [96,109]. Due to visitation restrictions, patients and healthcare providers employed virtual tools for ACP discussions, leading to significant improvements in ACP documentation [99,102,117].
Initiatives like the BRIDGES program [111] and telemedicine curricula [97] further broadened the scope and accessibility of ACP discussions, ensuring that even during the pandemic, care remained aligned with patient values and goals. Meanwhile, healthcare providers saw the importance of proactive ACP in reducing unwanted interventions and healthcare costs [113] and made strides towards incorporating ACP into standard practice, as evidenced by the integration of ACP into electronic health records and the widespread use of care planning tools [108,118]. Furthermore, one study demonstrated that ACP led to cost benefits for healthcare systems and enhanced patient quality of life, especially in frail populations [106].
Despite the complexity of initiating ACP discussions and the preference for in-person encounters, some studies demonstrated that meaningful ACP conversations can occur remotely, with tailored approaches to individual needs [100,101]. This shift was also reflected in the increased utilization of patient portals for ACP [121], and the expansion of ACP discussions to address a wider range of medical issues during telehealth visits [122]. The pandemic’s pressures underscored the need for ACP to be routine, adaptable, and patient-centered [107,110,115], and, moving forward, the innovations made during the pandemic were believed to help facilitate those goals.
3.2.4. Recommendation Category
The 26 manuscripts included in the Recommendation category are shown in Table 5 (extra details are presented in Table S4). The works included here represent documents from experts in the field of ACP or organizations that gave recommendations concerning ACP practice at a time of great upheaval in the healthcare system. For this category, the table includes only the Study ID, country, quality assessment, and coded barriers and facilitators.
The COVID-19 pandemic spurred many experts in the field to write recommendations regarding ACP, emphasizing its importance and utility for healthcare systems [142,146]. The manuscripts within the Recommendation category emphasized the need for ACP to be patient- and family-centered, addressing both general and acute serious illness-specific preferences [124,125,126]. The authors of the papers within this category also suggested the necessity of innovations in ACP, including, again, the use of telehealth to facilitate discussions [126,127,128,130,145,146,147,148], and temporary policy changes or innovations to ease the completion and accessibility of ACP documents [135,138,145,146,147,148]. However, the urgency of the situation also highlighted the potential for misunderstandings and mistrust [125,137], suggesting the importance of clear, empathetic communication and ongoing dialogue [133,141,149].
There were recommendations that ACP discussions during the pandemic should encompass preferences concerning COVID-19 treatment options, ventilator use, and hospitalization [132,133,135,144,149]. The pandemic has prompted a reevaluation of ACP processes, encouraging a more nuanced approach that considers individual relationships, cultural, and religious aspects, within the evolving nature of the healthcare crisis [136,137,140,141,148]. ACP was recognized as useful for managing healthcare surges, respecting human rights, and enabling proactive care coordination [138,139]. A number of commentators suggested that the emphasis on ACP was expected to continue beyond the pandemic, with a push for incorporating these discussions as a routine element of care for all patients, particularly older adults and those with multiple health conditions [109,110]. Health and care organizations focused on older adults are encouraged to ensure up-to-date ACP policies, establish effective storage systems for ACP documentation, and provide comprehensive support to facilitate these critical discussions [144,145].
3.3. ACP Barriers and Facilitators Coding
The extracted ACP barriers and facilitators were codified and quantified; 165 barriers, categorized into 25 codes, and 250 facilitators, categorized into 21 codes, were identified. Table 6 shows the list of codified and quantified barriers to ACP and their frequency across the four categories. The most frequently occurring ACP barrier codes were: Social distancing measures and visitation restrictions (n = 35, 21%), Uncertainty surrounding the COVID-19 prognosis (n = 12, 7.1%), Technological/Telehealth barriers (n = 10, 5.9%), Lack of awareness/knowledge of ACP (n = 9, 5.3%), Limited resources (n = 9, 5.3%), Personal protective equipment requirements (n = 9, 5.3%), Rapid disease progression (n = 9, 5.3%), Strained healthcare system (n = 9, 5.3%), Time constraints (n = 9, 5.3%), Cultural and religious beliefs (n = 7, 4.1%), Discomfort among clinicians and patients discussing end-of-life care (n = 7, 4.1%), and Healthcare system barriers (n = 7, 4.1%).
Table 7 shows the list of codified and quantified facilitators to ACP and the frequency across the four categories. The most frequently occurring ACP facilitator codes were: Telehealth/virtual ACP platforms (n = 41, 16.4%), Training for clinicians (n = 29, 11.6%), Care team collaboration (n = 24, 9.6%), Innovation and flexibility and in ACP documentation processes (n = 22, 8.8%), Guidance and protocols for ACP discussions (n = 21, 8.4%), ACP/palliative care experts (n = 18, 7.2%), Resources/education for patients/families (n = 16, 6.4%), Identification of those in need of ACP (n = 12, 4.8%), Healthcare system improvements (n = 11, 4.4%), Improved messaging (n = 11, 4.4%), Resources for clinicians (n = 11, 4.4%), and Public awareness of ACP (n = 8, 3.2%).
Figure 2 shows a visualization in the form of a bubble diagram, of the identified ACP barriers (n = ≥7) and facilitators (n = ≥11) during the COVID-19 pandemic. The bubble diagram was created manually with the size and placement of the bubbles, respectively, representing the frequencies and interactions between the different barriers and facilitators.
3.4. Sub-Analysis of ACP Documentation/Engagement Increase and Decrease
Of the 115 included studies, 3 (2.6%) and 29 (25.2%) studies attested to decreased and increased ACP engagement/documentation during the COVID-19 pandemic, respectively. One study from Taiwan reported a 48% (1.9-fold) decrease in ACP engagement/documentation caused by the pandemic. The level of increase (% increase) in engagement/documentation ranged between 25.4% and 396% (mean 137.75%) according to the 18 studies that included analyzable data (Table 8). One of these studies also reports a 3163% increase in life-sustaining treatment (LST) documentation. Of the 34 studies that reported increased ACP, those that described ACP-related educational interventions and innovations (6) reported an increase in ACP of 25.4–101.6% (mean 55.2%). Studies that described ACP-related innovations (10) reported an increase in ACP of 33.3–396% (mean 151%).
4. Discussion
The purpose of this systematic review was to gain granular insights into the facilitators of and barriers to ACP during the COVID-19 pandemic. Analysis of the 115 included studies revealed 25 barrier codes and 21 facilitator codes, some of which were typical to ACP and others that were unique to, or amplified by, the pandemic situation. The findings of this study are in accordance with our previously published umbrella review, which aimed to identify the barriers to and facilitators of ACP implementation for healthcare workers across different settings [30]. In that study, we found frequent barriers to implementing ACP were visitation restrictions, a scarcity of resources and staff, poor collaboration among healthcare workers, an insufficient number of palliative care doctors, and the emotional strain on staff. The widespread uptake of telemedicine for communication was found to be the key facilitator of ACP. Other facilitating factors consisted of ACP/palliative care training, the integration of palliative care physicians into the acute care teams, and emotional support for medical staff [30]. The current study, while undergirding the findings of our previous study, builds upon that work by offering a deeper level of granularity. There follows separate discussions of the key barriers and facilitators identified in this study.
4.1. Barriers to ACP during the COVID-19 Pandemic
The findings of our review demonstrate that the COVID-19 pandemic has presented multifaceted barriers to effective ACP, necessitating a comprehensive understanding of these challenges to improve future practices. The most important and obvious barrier identified was the requirement for social distancing and restrictions on visitation in healthcare settings [36,37,39,40,42]. These measures, while deemed essential for infection control, intentionally isolated vulnerable populations and limited the face-to-face interactions with family members and healthcare professionals that are crucial for meaningful ACP discussions and shared decision-making. While telehealth emerged as an alternative to in-person consultations, it presented its own set of challenges [43,49,61,63,76]. The digital divide, particularly among older adults and those from lower socioeconomic backgrounds, has the potential to hinder access to telehealth services. Additionally, the nuances of ACP conversations, which often rely on non-verbal cues and a personal touch, could be lost in virtual settings.
Similarly, the necessity for PPE created a further physical barrier between healthcare providers and patients [39,40,44,48,53]. This not only made communication more challenging but also added an impersonal element to clinical interactions, which, in the context of ACP, are typically highly sensitive and personal. Furthermore, ACP discussions are typically time intensive due to their complexity and sensitivity; thus, the high volume of patients and the acute nature of COVID-19 treatment left healthcare professionals with limited time, which was identified as a barrier to ACP in various studies [44,45,49,55,76]. Indeed, the lack of time, PPE, hospital beds, medical equipment, and personnel were symptomatic of a healthcare system at breaking point. The overwhelming number of COVID-19 patients stretched healthcare resources thin [90,98,126,128,138]. Limited resources, including staff time and attention, impeded the ability to conduct thorough ACP discussions. The pandemic put an unprecedented strain on healthcare systems globally. This strain on healthcare systems, which was also noted as a barrier to ACP [40,48,55,61,92], led to a focus on managing acute cases and emergencies, often at the expense of important care planning conversations.
The COVID-19 disease itself presented a number of barriers to ACP. The novel and unpredictable nature of COVID-19 made prognostication challenging, complicating ACP discussions [98,124,125,128,149]. Uncertainty about the disease’s progression, outcomes, and long-term effects made it difficult for both patients and healthcare providers to make informed decisions about future care preferences. In particular, the rapid disease progression of COVID-19 infection was identified as a barrier to ACP in a number of studies [38,48,60,138,139,140]. Healthcare providers often found themselves making critical decisions rapidly, with limited input from patients or their families, potentially compromising the principles of patient-centered care and informed consent. The urgent focus on acute care for COVID-19 patients also often overshadowed the need for ACP, leading to missed opportunities for proactive care planning, especially for high-risk populations. Family clustering of COVID-19 was also identified as a barrier to ACP in one study [147].
The pandemic exposed a significant gap in public and sometimes professional awareness and understanding of ACP. This lack of awareness or knowledge of ACP was identified as a major barrier [55,64,66,86,90,125]. Some studies noted a need for adequate ACP training for clinicians as a barrier [76,91,142]. Moreover, the findings of our review indicate that certain communities experienced or were vulnerable to a lack of engagement in ACP due to a combination of factors; disparities in health education [90], cultural and religious beliefs [57,86,90,142], socioeconomic challenges [57,140], a general distrust in the healthcare system [65,124,125,137], and racial or ethnic barriers [53,90,124,140] played significant roles. These factors were compounded by the pandemic’s exacerbation of healthcare access disparities. This situation highlighted the need for more tailored, inclusive, and accessible approaches to health education and care planning, especially in underserved communities.
4.2. Facilitators of ACP during the COVID-19 Pandemic
The COVID-19 pandemic, while presenting numerous challenges, has also acted as a catalyst for several facilitators that have enhanced the process of and access to ACP. These facilitators have played a pivotal role in adapting ACP to the unique demands of a global health crisis. The rapid expansion and adoption of telehealth services has been a significant facilitator for ACP, identified in a large number of studies [93,96,99,100,101,102,104]. Virtual platforms have provided a means for clinicians and patients to engage in ACP discussions safely, overcoming the barriers imposed by social distancing and visitation restrictions as discussed above. This technology has made ACP more accessible, particularly for vulnerable populations or those in remote areas. Acevedo Rodriguez and colleagues, for example, describe their intervention to increase ACP among a population of veterans diagnosed with COVID-19, through direct telephone calls, which led to a 37% increase in ACP documentation and a 3163% increase in life-sustaining treatment (LST) documentation [104]. The videoconferencing software Zoom (Zoom Video Communications Inc., San Jose, CA, USA, 2016), was mentioned in numerous papers as a means for facilitating ACP or related educational interventions [67,83,86,111].
Alongside the telehealth-related innovations that have facilitated ACP conversation, this review also revealed notable innovation and flexibility in ACP documentation accommodating the constraints of the pandemic [116,117,118,119,120,121,126,127,128,135]. These innovations, which have facilitated the completion and accessibility of ACP documents, include streamlining the ACP processes [127], modification of the electronic health records to facilitate ACP documentation [71], the use of user-friendly [83] and electronic ACP forms [116,121,126,145], COVID-19-specific ACP documentation [135], apps to capture electronic signatures [63], electronic means of signature witnessing [138], and drive-by document signing [63]. As an example of how ACP documentation innovations can increase ACP documentation, McFarlane and colleagues describe a 296% increase in usage of the NHS’s Coordinate My Care services (https://www.coordinatemycare.co.uk, accessed on 14 May 2023), which takes an innovative integrative approach to care planning (including an ACP component) [117].
As described above, the need for adequate ACP training for clinicians, identified as a barrier to ACP, was addressed in numerous studies (largely in the Education category) that aimed to encourage ACP engagement through the training of health professionals [70,71,72,73,74,75,76,77,78,79,80,81,82,83,86,88,89]. During the pandemic, enhanced training programs for healthcare professionals have been crucial in equipping them with the skills necessary for effective ACP conversations, including clinical communication skills training and best practice in telehealth/virtual ACP. Casey and colleagues, for example, described a 25.4% increase in emergency department-based ACP following implementation of a “rapid and simple” educational program for emergency physicians on ACP [71]. Alongside such training, access to clinician-facing ACP-related resources [72,74,78,88,103] was also a facilitator to ensure that clinicians can navigate the complex and sensitive nature of ACP discussions, even under the stressful pandemic conditions. Resources for physicians included websites for palliative care/ACP information, visual aids, video materials, telephone call-center support, ACP tip sheets, etc. Among the most important resources for clinicians, identified as a ACP facilitators, were guidance and protocols for ACP discussions [139,141,144,146,147,148,149], including established guides such as Vital Talk [139,148] and COVID-19-specific goals-of-care discussion guides [94,112]. The development of specific guidance and protocols for ACP during the pandemic provided clinicians with clear frameworks to help ensure that ACP discussions are consistent, comprehensive, and adapted to the COVID-19 context.
Similar to the education and resources offered to healthcare professionals, public-facing ACP education and resources for patients and family members were also identified as facilitators for ACP [64,65,66,69,72,80]. The increased availability of resources and education for patients and families has been vital in facilitating ACP. This includes information delivered through websites, videos, community-based education, etc., about the importance of ACP, how to approach ACP conversations, and the specifics of healthcare decision-making in the context of COVID-19. For example, one 2020 study by Auriemma and colleagues showed that their free online resource, OurCareWishes.org, designed to guide patients and families through ACP, saw a 396% increase in ACP documentation after the onset of the COVID-19 pandemic [123]. Volandes and colleagues, in their large-scale nonrandomized controlled trial, implemented an intervention using ACP video decision aids and clinician communication during the pandemic that was associated with higher rates of ACP documentation (32% overall increase), especially for Hispanic and African American patients [50]. Increasing the availability and quality public-facing ACP resources, thus, could be particularly useful for reaching underserved communities.
Raising public awareness of ACP acted as an important facilitator for ACP engagement [42,45,48,54,58]. Among the studies included in our review were accounts of various efforts and recommendations to promote the need to engage in ACP, including large-scale initiatives [69], mass dissemination of ACP-related materials [58], and increased media coverage [42,54] around the necessity for early ACP decision-making. Tied to the need for improved resources, improved messaging [66,88,91,125,137] was also noted as a facilitator for ACP. Among the strategies to improve messaging were connections with community religious leaders and community organizations [58,137], the use of short videos [88], and motivational stories [125]. Enhanced messaging strategies regarding ACP have the potential to improve public awareness of its importance, leading to greater engagement in ACP. Indeed, the pandemic itself seems to have increased public understanding of the importance of ACP; the widespread fear of COVID-19, or an understanding of its dangers, has served as a motivator for both individuals and families to engage in ACP, recognizing the potential for rapid health deterioration and the importance of having care preferences documented [42,46,50,54,116]. Brophy and colleagues, for example, found that “perceived susceptibility to COVID-19 was a statistically significant positive predictor of intention to share one’s own EOL wishes” [46]. Comparing pre- and post-pandemic numbers, Connellan and colleagues reported a 291.5% increase in do-not-attempt-cardiopulmonary-resuscitation (DNACPR) documentation in older hospitalized patients [50].
The pandemic has fostered a greater sense of the need for collaboration among healthcare teams, which was identified as a major facilitator of ACP [92,94,95,96,105,111]. This teamwork was leveraged to help facilitate comprehensive, patient-centered ACP during the pandemic, ensuring that various perspectives and expertise are considered in care planning. A study by Singh and colleagues, for example, showed how social work and care management intervention, by involving social workers within the care team, increased Medical Durable Power of Attorney (MDPOA) documentation by 12.7% compared to baseline averages [105]. The care team collaboration that emerged from our review included the establishing of new, or developing preexisting, networks of support and integrated working within and between care teams and services, multi-disciplinary/interdisciplinary team engagement [96], an Interdisciplinary Ethics Panel (IEP) approach to decision making [92], and teams of professionals focused on proactively providing and supporting ACP [87,88,94,95].
In the same vein, a number of studies highlighted the involvement of ACP and palliative care experts, such as geriatricians, nurse practitioners, trained ACP clinicians, specialist palliative care clinicians, and chaplains, as an important facilitator of ACP [124,134,144,147,148]. ACP and palliative care experts can help to ensure that ACP is conducted with a high level of expertise and sensitivity, especially in complex and difficult cases or in those with advanced illness, of which there were many during the pandemic. Effective strategies to identify patients who would most benefit from ACP were also observed to be key facilitators [82,87,94,98,100]. These strategies included intensive outreach efforts to identify vulnerable patients, targeted programs aimed at those without ACP documentation, palliative care consultations, and the use of palliative care screening tools. As alternatives to in-person consultations, these programs often utilized telehealth technology, while some opted for direct postal mail. This proactive approach helped to deliver ACP to those at high risk of COVID-19 hospitalization/complications or those with significant healthcare needs. Similar to the proactive identification of those in need of ACP, the pandemic has encouraged an appreciation of a more proactive initiation of ACP conversations, with healthcare providers beginning discussions earlier in the patient journey [51,56,113,115,132]. In summary, these facilitators, among others, have collectively contributed to a more robust and adaptable ACP process that could weather the storm of the COVID-19 pandemic. This period of crisis has brought about significant learning and adaptation, potentially shaping the future of ACP to be more resilient, patient-centered, and integrated into routine healthcare.
4.3. Limitations
There are a number of limitations to this review that should be considered. First, the large number of included studies, while allowing for a high-resolution picture of ACP practice during the pandemic, also raised a number of issues with regards to data extraction, analyses, and quality assessment. These steps, because they were so time-consuming, were primarily conducted by the first author (T.M.) with careful oversight from the other authors to help mitigate potential bias. Second, inter-rater reliability measures for the manuscript screening showed only moderate agreement between the two reviewers. This could be due to a number of factors, namely, language differences and vision for the review; however, the final inclusion of papers was reached after lengthy discussion and debate, thus the included papers represent an agreed-upon selection. Thirdly, the majority (84.2%) of the included studies came from North America (n = 76, 66%) and the UK (n = 21, 18.2%), which biases the findings of our review towards these regions and perhaps does not give as full a picture of global trends as we originally sought to achieve. However, the US, Canada, and the UK are multicultural societies with healthcare systems in place that cater for people of various cultures, ethnicities, nationalities, languages, and faith traditions, which perhaps offsets this particular bias somewhat.
5. Conclusions
In this systematic review, we sought to investigate how the COVID-19 pandemic had affected the practice of ACP, the obstacles it presented, and the trends that emerged to facilitate ACP practice at a time when the healthcare system was strained to breaking point. In the published literature, the COVID-19 pandemic seems to have had a positive effect on the uptake and acceptance of ACP, or, at very least, it has increased general awareness of the importance and utility of ACP. The pandemic presented severe barriers, to ACP, such as strict social distancing measures, uncertainty surrounding the COVID-19 prognosis, the rapid disease progression, PPE requirements, and scarce resources and time, as well as exacerbating typical barriers to ACP, such as emotional, cultural, religious, educational, and racial barriers. However, the published literature from the first two years of the pandemic revealed a situation in which healthcare providers rose to meet those multiform challenges by finding innovative solutions to facilitate ACP, with trends towards widespread adoption of telehealth and flexibility in ACP documentation processes, utilizing multidisciplinary care teams and ACP and palliative care experts, and providing ACP-related guidance and recommendations, resources, and education to clinicians, patients, and caregivers. In summary, the findings of our systematic review showed that, for many counties, the COVID-19 pandemic, despite presenting many barriers, has been an opportunity for promoting ACP amongst diverse populations. Studying how healthcare providers rose to meet the challenges of delivering and promoting ACP during this pandemic can give us important insights for dealing with possible future medical crises and also for improving ACP practice in healthcare practice moving forward.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shahid Z. Kalayanamitra R. Mc Clafferty B. Kepko D. Ramgobin D. Patel R. Aggarwal C.S. Vunnam R. Sahu N. Bhatt D. COVID-19 and Older Adults: What We Know J. Am. Geriatr. Soc.20206892692910.1111/jgs.1647232255507 PMC 7262251 · doi ↗ · pubmed ↗
- 2Lebrasseur A. Fortin-Bédard N. Lettre J. Raymond E. Bussières E. Lapierre N. Faieta J. Vincent C. Duchesne L. Ouellet M. Impact of the COVID-19 Pandemic on Older Adults: Rapid Review JMIR Aging 20214 e 2647410.2196/2647433720839 PMC 8043147 · doi ↗ · pubmed ↗
- 3Nanda A. Vura N.V.R.K. Gravenstein S. COVID-19 in older adults Aging Clin. Exp. Res.2020321199120210.1007/s 40520-020-01581-532390064 PMC 7211267 · doi ↗ · pubmed ↗
- 4Kasar K.S. Karaman E. Life in lockdown: Social isolation, loneliness and quality of life in the elderly during the COVID-19 pandemic: A scoping review Geriatr. Nurs.2021421222122910.1016/j.gerinurse.2021.03.01033824008 PMC 8566023 · doi ↗ · pubmed ↗
- 5Armitage R. Nellums L.B. COVID-19 and the consequences of isolating the elderly Lancet Public Health 20205 e 25610.1016/S 2468-2667(20)30061-X 32199471 PMC 7104160 · doi ↗ · pubmed ↗
- 6Whitehead B.R. Torossian E. Older Adults’ Experience of the COVID-19 Pandemic: A Mixed-Methods Analysis of Stresses and Joys Gerontologist 202161364710.1093/geront/gnaa 12632886764 PMC 7499618 · doi ↗ · pubmed ↗
- 7Vahia I.V. Jeste D.V. Reynolds C.F. Older Adults and the Mental Health Effects of COVID-19JAMA 20203242253225410.1001/jama.2020.2175333216114 · doi ↗ · pubmed ↗
- 8Chen L.K. Older adults and COVID-19 pandemic: Resilience matters Arch. Gerontol. Geriatr.20208910412410.1016/j.archger.2020.10412432474351 PMC 7247489 · doi ↗ · pubmed ↗