Unveiling Ureaplasma: A Case Report of a Rare Culprit in Pyelonephritis
Manish Shrestha, Devi Parvathy Jyothi Ramachandran Nair, Shefali Amin, Arpan Pokhrel, Salina Munankami

TL;DR
A rare case of pyelonephritis caused by Ureaplasma highlights the need for molecular diagnostics when standard tests fail.
Contribution
This case report presents a rare instance of Ureaplasma-induced pyelonephritis and emphasizes the role of molecular diagnostics in its detection.
Findings
Routine urine culture failed to detect Ureaplasma in a pyelonephritis case.
PCR identified Ureaplasma urealyticum as the causative agent after empirical treatment failed.
Switching to doxycycline led to significant clinical improvement in the patient.
Abstract
Ureaplasma species, typically considered commensal organisms of the human urogenital tract, have been implicated in various urinary tract infections (UTIs), including the rare and challenging presentation of pyelonephritis. This case report describes a unique instance of pyelonephritis induced by Ureaplasma, characterized by a negative routine urine culture and a lack of response to empirical antibiotic treatment, highlighting the complexities associated with diagnosing and managing infections caused by atypical pathogens. A 50-year-old female presented to the emergency department with symptoms suggestive of UTI, including fever, vomiting, and dysuria. However, initial urine analysis was notable for pyuria while routine bacterial culture returned negative results, creating a diagnostic dilemma. Empirical treatment with third-generation cephalosporin was initiated. However, the patient's…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1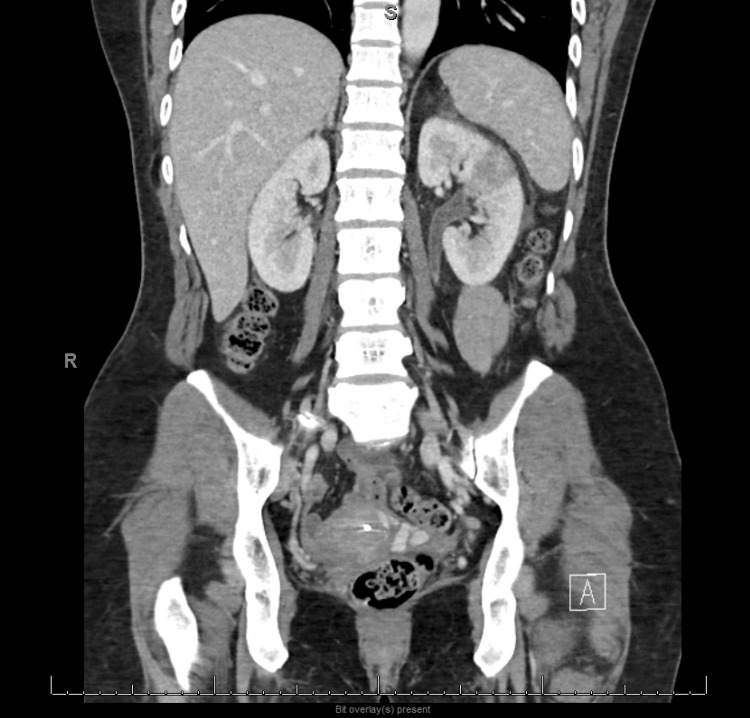 Figure 2
Figure 2| Laboratory Test | Value | Reference Range |
| Sodium (mmol/L) | 137 | 136-145 |
| Potassium (mmol/L) | 3.4 | 3.5-5.1 |
| Chloride (mmol/L) | 107 | 98-107 |
| Blood Urea Nitrogen (mg/dL) | 9 | 7-25 |
| Creatinine (mg/dL) | 0.61 | 0.6-1.3 |
| Glucose (mg/dL) | 107 | 70-99 |
| Calcium (mg/dL) | 8.3 | 8.6-10.3 |
| Albumin (g/dL) | 3.3 | 3.5-5.7 |
| Total protein (g/dL) | 6 | 6.4-8.9 |
| Aspartate aminotransferase (IU/L) | 65 | 13-39 |
| Alanine aminotransferase (IU/L) | 54 | 7-52 |
| Alkaline phosphatase (IU/L) | 62 | 34-104 |
| White blood cells (x 103/uL) | 15.6 | 4.8-10.8 |
| Red blood cells (x 106/uL) | 3.61 | 4.5-6.1 |
| Hemoglobin (g/dL) | 10.2 | 12-16 |
| Platelets (x 103/uL) | 125 | 130-400 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Pediatric Urology and Nephrology Studies · Urinary Bladder and Prostate Research
Introduction
Ureaplasma urealyticum, a member of the family Mycoplasmataceae, is a small, wall-deficient bacterium that is a common inhabitant of the human urogenital tract [1]. Although often considered a commensal organism, Ureaplasma has been implicated in various clinical conditions, ranging from asymptomatic colonization to severe infections such as non-gonococcal urethritis and pyelonephritis [1]. Pyelonephritis, an infection of the upper urinary tract, typically presents with symptoms of fever, flank pain, and dysuria and is most commonly caused by Escherichia coli with the standard approach to diagnosis being urine culture, which guides targeted antimicrobial therapy [2].
However, the diagnosis and management of pyelonephritis caused by atypical pathogens such as Ureaplasma are challenging as the infection has atypical presentation, such as a negative urine culture or resistance to empiric antibiotic therapy, which is designed to cover common uropathogens [3]. The case of Ureaplasma-induced pyelonephritis with negative culture results and non-responsiveness to empiric treatment is unique and noteworthy as it underscores the diagnostic limitations of standard urine cultures in detecting Ureaplasma species, which require specific culture media and conditions for growth [1,3]. Moreover, it highlights the organism's potential for pathogenicity in the urinary tract, challenging the prevailing notion of Ureaplasma as a harmless commensal [1,3]. Thus, the case illustrates the importance of considering atypical pathogens in patients with pyelonephritis who do not respond to standard empiric therapy.
Case presentation
A 50-year-old sexually active woman with a history of recurrent urinary tract infection (UTI) and bacterial vaginosis presented to the hospital with fever, chills, nausea, and vomiting for three days. These symptoms were associated with burning urination and increased urinary frequency. She denied having hematuria and abdominal pain but experienced mild discomfort in the suprapubic area. Initially seen as an outpatient, she was prescribed 500 mg of ciprofloxacin twice daily for her symptoms. She took a single dose before presenting to the emergency department due to worsening symptoms. She has been taking nitrofurantoin 100 mg as postcoital prevention for her recurrent urinary tract infections for a few years.
Upon presentation, her temperature was 100.7°F, heart rate was 82 beats per minute, respiratory rate was 18 breaths per minute, and blood pressure was 111/70 mmHg, with an oxygen saturation of 98% on room air. She was awake, alert, and oriented but appeared fatigued. The examination revealed left costovertebral angle tenderness and mild lower abdominal tenderness with normal bowel sounds. She did not exhibit rebound tenderness. Laboratory analysis (Table 1) showed an unremarkable basic metabolic panel, while the complete blood count revealed elevated white blood cells at 15.6 x 10^9^/L. Urinalysis revealed cloudy urine with moderate blood. Microscopic urine assessment found occasional mucus and six white blood cells per high-power field, and it was negative for nitrites, leukocyte esterase, and bacteria.
Table 1: Laboratory Analysis
<table><tbody><tr><td rowspan="1" colspan="1"> Laboratory Test </td><td rowspan="1" colspan="1"> Value </td><td rowspan="1" colspan="1"> Reference Range </td></tr><tr><td rowspan="1" colspan="1"> Sodium (mmol/L) </td><td rowspan="1" colspan="1"> 137 </td><td rowspan="1" colspan="1"> 136-145 </td></tr><tr><td rowspan="1" colspan="1"> Potassium (mmol/L) </td><td rowspan="1" colspan="1"> 3.4 </td><td rowspan="1" colspan="1"> 3.5-5.1 </td></tr><tr><td rowspan="1" colspan="1"> Chloride (mmol/L) </td><td rowspan="1" colspan="1"> 107 </td><td rowspan="1" colspan="1"> 98-107 </td></tr><tr><td rowspan="1" colspan="1"> Blood Urea Nitrogen (mg/dL) </td><td rowspan="1" colspan="1"> 9 </td><td rowspan="1" colspan="1"> 7-25 </td></tr><tr><td rowspan="1" colspan="1"> Creatinine (mg/dL) </td><td rowspan="1" colspan="1"> 0.61 </td><td rowspan="1" colspan="1"> 0.6-1.3 </td></tr><tr><td rowspan="1" colspan="1"> Glucose (mg/dL) </td><td rowspan="1" colspan="1"> 107 </td><td rowspan="1" colspan="1"> 70-99 </td></tr><tr><td rowspan="1" colspan="1"> Calcium (mg/dL) </td><td rowspan="1" colspan="1"> 8.3 </td><td rowspan="1" colspan="1"> 8.6-10.3 </td></tr><tr><td rowspan="1" colspan="1"> Albumin (g/dL) </td><td rowspan="1" colspan="1"> 3.3 </td><td rowspan="1" colspan="1"> 3.5-5.7 </td></tr><tr><td rowspan="1" colspan="1"> Total protein (g/dL) </td><td rowspan="1" colspan="1"> 6 </td><td rowspan="1" colspan="1"> 6.4-8.9 </td></tr><tr><td rowspan="1" colspan="1"> Aspartate aminotransferase (IU/L) </td><td rowspan="1" colspan="1"> 65 </td><td rowspan="1" colspan="1"> 13-39 </td></tr><tr><td rowspan="1" colspan="1"> Alanine aminotransferase (IU/L) </td><td rowspan="1" colspan="1"> 54 </td><td rowspan="1" colspan="1"> 7-52 </td></tr><tr><td rowspan="1" colspan="1"> Alkaline phosphatase (IU/L) </td><td rowspan="1" colspan="1"> 62 </td><td rowspan="1" colspan="1"> 34-104 </td></tr><tr><td rowspan="1" colspan="1"> White blood cells (x 10<sup>3</sup>/uL) </td><td rowspan="1" colspan="1"> 15.6 </td><td rowspan="1" colspan="1"> 4.8-10.8 </td></tr><tr><td rowspan="1" colspan="1"> Red blood cells (x 10<sup>6</sup>/uL) </td><td rowspan="1" colspan="1"> 3.61 </td><td rowspan="1" colspan="1"> 4.5-6.1 </td></tr><tr><td rowspan="1" colspan="1"> Hemoglobin (g/dL) </td><td rowspan="1" colspan="1"> 10.2 </td><td rowspan="1" colspan="1"> 12-16 </td></tr><tr><td rowspan="1" colspan="1"> Platelets (x 10<sup>3</sup>/uL) </td><td rowspan="1" colspan="1"> 125 </td><td rowspan="1" colspan="1"> 130-400 </td></tr></tbody></table>Computed tomography of the abdomen and pelvis with contrast showed findings consistent with left-sided pyelonephritis (Figure 1) and associated urethritis (Figure 2), as well as a suggestion of chronic pelvic venous congestion syndrome. The patient was admitted with a primary working diagnosis of sepsis secondary to left-sided pyelonephritis and was treated with intravenous fluids and empirical antibiotic coverage with IV ceftriaxone. Urine culture results showed no growth. She was discharged on oral cefpodoxime to complete a 10-day course.
CT scan of abdomen and pelvis revealing areas of low-attenuation within the anterior lateral and posterior medial mid-left kidney suggestive of acute pyelonephritis
CT scan of abdomen and pelvis showing mild left ureteral wall thickening secondary to ureteritis
One week later, she presented to the outpatient internal medicine office with persistent symptoms of dysuria and urinary frequency, even after she had completed the prescribed course of antibiotics. The examination also revealed mild left costovertebral angle tenderness. There was a growing suspicion of atypical organisms like Ureaplasma and Mycoplasma, and tests were conducted accordingly. Polymerase chain reaction (PCR) testing on the urine sample returned positive for U. urealyticum. She was started on a 10-day course of oral doxycycline. Upon follow-up after a week, the patient had successfully recovered from the treatment. Considering her recurrent UTI symptoms, we suspect that untreated Ureaplasma may have been the cause of her longstanding urethritis and might have contributed to the reflux pyelonephritis.
Discussion
Ureaplasma species, particularly U. urealyticum and U. parvum, are common inhabitants of the human urogenital tract [1]. While often commensal, these microorganisms have been implicated in various UTIs, including urethritis, cystitis, and, more rarely, pyelonephritis [1,2]. The precise prevalence of Ureaplasma-induced pyelonephritis remains difficult to ascertain due to diagnostic challenges [4]. Ureaplasma species are frequently isolated from the urogenital tract, with varying colonization rates reported in sexually active adults, with up to 80% of healthy females having Ureaplasma species in their cervical or vaginal secretions [5]. Despite their prevalence, the incidence of these bacteria as causative agents in pyelonephritis cases is not well-documented, partly because of limitations in routine bacterial culture methods [5].
Ureaplasma species possess several virulence factors that facilitate colonization of the urogenital tract and evasion of host immune responses [6]. The organisms' ability to adhere to uroepithelial cells and produce urease contributes to urinary tract colonization and infection by increasing urinary pH, promoting the formation of struvite stones, and creating a favorable environment for bacterial proliferation [6,7]. However, the mechanisms by which Ureaplasma species ascend to the upper urinary tract and induce pyelonephritis are not fully understood and warrant further investigation. Diagnosing Ureaplasma-induced pyelonephritis is complicated by the organisms' fastidious growth requirements, which are not met by standard UTI culture protocols [8]. Molecular methods such as PCR offer greater sensitivity and specificity but are only routinely available in some clinical settings ([8,9]. The development of rapid, accurate, and cost-effective diagnostic tests remains a critical need in managing Ureaplasma-associated UTIs. Treatment of Ureaplasma-induced pyelonephritis typically involves antibiotics such as tetracyclines and macrolides, to which these organisms are generally susceptible ([10]. However, emerging resistance to these antibiotics poses a significant challenge, and the lack of standardized treatment guidelines for Ureaplasma infections complicates the management of these cases, highlighting the need for further research on effective therapeutic strategies ([10,11].
The clinical outcomes of Ureaplasma-induced pyelonephritis vary, ranging from complete resolution with appropriate antibiotic therapy, like in this case, to chronic infection and renal scarring in cases of delayed diagnosis or treatment failure [12].
Conclusions
Ureaplasma-induced pyelonephritis represents a complex and underrecognized clinical entity. Current challenges include improved diagnostic methods, effective treatment regimens, and a deeper understanding of the pathogenesis of Ureaplasma infections. Addressing these issues through continued research and clinical vigilance is essential for optimizing patient care and outcomes in Ureaplasma-associated UTIs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ureaplasma urealyticum pyelonephritis presenting with progressive dysuria, renal failure, and neurologic symptoms in an immunocompromised patient Transpl Infect Dis Schwartz DJ Elward A Storch GA Rosen DA 0212019 https://pubmed.ncbi.nlm.nih.gov/30472777/10.1111/tid.13032 PMC 654245930472777 · doi ↗ · pubmed ↗
- 2Acute pyelonephritis Stat Pearls [Internet] Belyayeva M Jeong JM Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 519537/30137822 · pubmed ↗
- 3Ureaplasma urealyticum infection presenting as pyelonephritis and perinephric abscess in an immunocompromised patient BMJ Case Rep Ngoo A Eisemann J Matsika A Winkle D 0132020 https://pubmed.ncbi.nlm.nih.gov/32414777/10.1136/bcr-2020-234538 PMC 723273832414777 · doi ↗ · pubmed ↗
- 4A systematic review of mycoplasma and ureaplasma in urogynaecology Geburtshilfe Frauenheilkd Combaz-Söhnchen N Kuhn A 12991303772017 https://pubmed.ncbi.nlm.nih.gov/29269957/2926995710.1055/s-0043-119687 PMC 5734936 · doi ↗ · pubmed ↗
- 5Congenital and opportunistic infections: Ureaplasma species and Mycoplasma hominis Semin Fetal Neonatal Med Waites KB Schelonka RL Xiao L Grigsby PL Novy MJ 190199142009 https://pubmed.ncbi.nlm.nih.gov/19109084/1910908410.1016/j.siny.2008.11.009 · doi ↗ · pubmed ↗
- 6Adherence of Ureaplasma urealyticum to human epithelial cells Microbiology (Reading) Smith DG Russell WC Thirkell D 28932898140 ( Pt 10)1994 https://pubmed.ncbi.nlm.nih.gov/8000551/800055110.1099/00221287-140-10-2893 · doi ↗ · pubmed ↗
- 7The role of Ureaplasma spp. in the development of nongonococcal urethritis and infertility among men Clin Microbiol Rev Beeton ML Payne MS Jones L 322019 https://pubmed.ncbi.nlm.nih.gov/31270127/10.1128/CMR.00137-18PMC 675013531270127 · doi ↗ · pubmed ↗
- 8Should we be testing for urogenital Mycoplasma hominis, Ureaplasma parvum and Ureaplasma urealyticum in men and women? - a position statement from the European STI Guidelines Editorial Board J Eur Acad Dermatol Venereol Horner P Donders G Cusini M Gomberg M Jensen JS Unemo M 18451851322018 https://onlinelibrary.wiley.com/doi/10.1111/jdv.151462992442210.1111/jdv.15146 · doi ↗ · pubmed ↗