Cerebral Air Embolism After Endoscopy: A Case Report
James Whall, Eli Besser, Jaymes Lonzanida, Ryan Roten

TL;DR
A 90-year-old woman developed a rare cerebral air embolism after an endoscopy, highlighting the need for awareness of this complication.
Contribution
This case report adds to the understanding of cerebral air embolism risks associated with endoscopic procedures.
Findings
A cerebral air embolism occurred after an esophagogastroduodenoscopy in a 90-year-old woman.
The patient presented with acute focal neurologic deficits.
The case emphasizes the importance of considering air embolism in post-endoscopy neurological emergencies.
Abstract
Cerebral air embolisms are a rare but potentially devastating event where air enters the vascular system. Although commonly associated with intravascular catheters, they can arise from a variety of mechanisms including endoscopic procedures. We report the case of a 90-year-old woman who presented with focal neurologic deficits due to an air embolism after undergoing an esophagogastroduodenoscopy. Cerebral air embolisms should be considered in patients who present to the emergency department with acute neurologic changes, especially after an endoscopic procedure.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
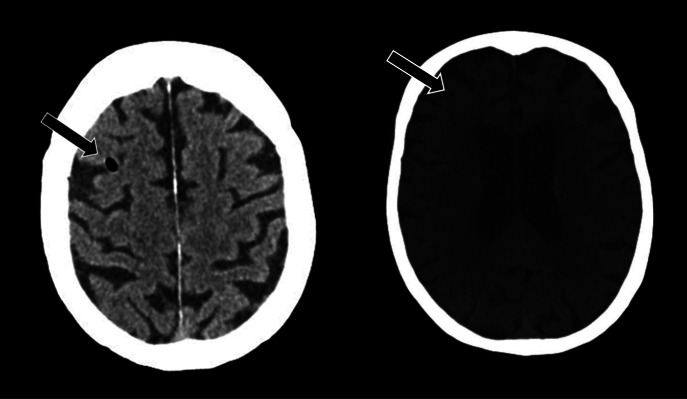 Image 1
Image 1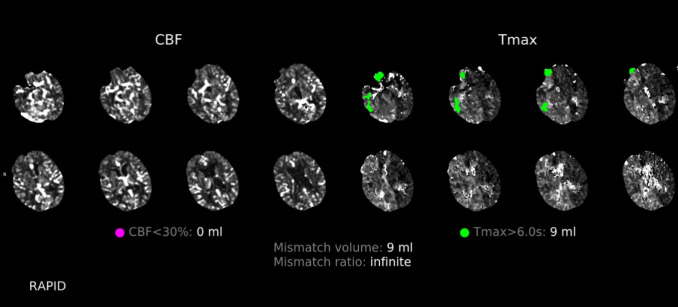 Image 2
Image 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Cardiac and Coronary Surgery Techniques · Pneumothorax, Barotrauma, Emphysema
INTRODUCTION
Air embolisms are characterized as unwanted air in the vascular system with potentially devastating morbidity and mortality.1 More commonly associated with intravascular catheters, these events have been rarely reported in a variety of endoscopic procedures.2 Although there are potentially devastating consequences of cerebral air embolisms (CAE), rapid diagnosis and treatment improves chances of recovery.3 Therefore, this rare complication should be considered in patients presenting for focal neurological deficits after endoscopic procedure.
CASE REPORT
A 90-year-old woman presented to the emergency department (ED) from an outpatient surgical center after undergoing an esophagogastroduodenoscopy (EGD) with right gaze deficit, left upper extremity flaccid paralysis, and aphasia. The patient received fentanyl and midazolam for sedation during the EGD, which were reversed with naloxone and flumazenil prior to arrival to the ED.
The patient’s presenting vital signs were a temperature of 36.8° Celsius, heart rate of 75 beats per minute, respiratory rate of 16 breaths per minute, blood pressure of 130/75 millimeters of mercury, and pulse oximetry at 100% on room air. The physical exam was significant for forced gaze to the right, left lower facial weakness, left upper and lower extremity flaccid paralysis. The patient was able to intermittently follow commands but could not speak. She was rapidly taken for imaging. A computed tomography (CT) head without contrast found several sub-centimeter air embolisms in the right frontal parietal region (Image 1).
Computed tomography head without contrast demonstrating air embolisms (arrow).
There was no evidence of intracranial hemorrhage or mass effect. A CT angiography of the head and neck did not reveal large vessel occlusions. A CT head with contrast found scattered right frontal, parietal, and temporal perfusion abnormalities compatible with ischemia (Image 2). Upon her return from imaging, the patient had seizure activity with rhythmic movement of the right upper extremity. The patient was treated with multiple doses of benzodiazepines and levetiracetam. She ultimately required intubation and was placed on a continuous infusion of midazolam.
*Computed tomography head with contrast demonstrating right frontal, parietal, and temporal regions with perfusion deficits (green). These deficits are defined by a time-to-maximum delay of over six seconds for contrast to move to the tissue. Without intervention, these regions are a reliable estimate of the final infarction area. There are no regions with cerebral blood flow deficits (purple), which would indicate completed ischemia. 4
CBF, cerebral blood flow; Tmax, time to maximum.*
Given the CT findings of CAE, the patient was placed in the left lateral Trendelenburg position, the fraction of inspired oxygen (FiO_2_) was maximized to 100%, and dexamethasone was given upon recommendation from the neurologist. A transthoracic echocardiogram found a normal ejection fraction, no patent foramen ovale, and no other significant findings. An electroencephalogram found no evidence of non-convulsive status epilepticus. The patient was transferred to a higher level of care for hyperbaric oxygen (HBO) therapy. Per the patient’s family, the patient did not have improvement at the tertiary hospital and was placed on comfort care.
DISCUSSION
Cerebral air embolisms have been reported in a variety of endoscopic procedures; however, they remain uncommon. A recent review of inpatient procedures found a rate of 0.57/100,000 endoscopic procedures and specifically 0.44/100,000 for EGD.5 A review of recent literature found a case of CAE presenting as a tonic-clonic seizure in a 52-year-old man during an EGD and a 71-year-old man presenting with hemiparesis and dysarthria two hours after undergoing EGD.6 ^,^ 7 In total there appear to be only 13 reported cases of CAE after EGD, reinforcing its rarity.8
There are a variety of proposed mechanisms by which gas can enter vasculature during endoscopy including through the portal vein, exposed gastrointestinal vessels, or through adjacent veins of inflamed mucosa.2 Theories on how air reaches the arterial system, and specifically the central nervous system, include paradoxical embolization through heart shunts such as a patent foramen ovale, retrograde flow through the superior vena cava, and through pulmonary veins if not filtered by the pulmonary system.8 The air then causes ischemia and injury by directly occluding vessels or by initiating an inflammatory cascade leading to thrombus formation.9
Although exceedingly rare, air embolism should be suspected in any patient with acute neurologic changes after an endoscopic procedure. A CT head may show evidence of cerebral gas embolism, as in this case. Gas may also be reabsorbed quickly and not be evident on imaging. Treatments include the following: 100% FiO_2_ to reduce bubble volume and increase diffusion gradient; placement in the left lateral Trendelenburg position; and HBO.3 Hyperbaric oxygen therapy is the most critical intervention; if started within five hours, HBO can double the chances of full recovery.10
CONCLUSION
Air embolisms are a rare but potentially devastating event. Air embolisms should be considered in patients who present to the ED with acute neurologic changes, especially after an endoscopic procedure. Rapid identification and treatment can lead to improved outcomes for the patient, highlighting the importance of increased awareness of this condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lanke G Adler DG. Gas embolism during endoscopic retrograde cholangiopancreatography: diagnosis and management. Ann Gastroenterol. 2019;32(2):156–67.30837788 10.20524/aog.2018.0339 PMC 6394273 · doi ↗ · pubmed ↗
- 2Donepudi S Chavalitdhamrong D Pu Let al. Air embolism complicating gastrointestinal endoscopy: a systematic review. World J Gastrointest Endosc. 2013;5(8):359–65.23951390 10.4253/wjge.v 5.i 8.359PMC 3742700 · doi ↗ · pubmed ↗
- 3Cooper J. Treatment of endoscopy associated cerebral gas embolism. Am J Gastroenterol. 2018;113(12):1742–4.29915395 10.1038/s 41395-018-0139-z PMC 6768578 · doi ↗ · pubmed ↗
- 4Butcher K Parsons M Allport Let al. Rapid assessment of perfusion–diffusion mismatch. Stroke. 2008;39(1):75–81.18063829 10.1161/STROKEAHA.107.490524 · doi ↗ · pubmed ↗
- 5Olaiya B Adler DG. Air embolism secondary to endoscopy in hospitalized patients: results from the National Inpatient Sample (1998–2013). Ann Gastroenterol. 2019;32(5):476–81.31474794 10.20524/aog.2019.0401 PMC 6686097 · doi ↗ · pubmed ↗
- 6Popa D Grover I Hayden Set al. Iatrogenic arterial gas embolism from esophagogastroduodenoscopy. J Emerg Med. 2019;57(5):683–8.31672399 10.1016/j.jemermed.2019.08.053 · doi ↗ · pubmed ↗
- 7Pandurangadu AV Paul JAP Barawi Met al. A case report of cerebral air embolism after esophagogastroduodenoscopy: diagnosis and management in the emergency department. J Emerg Med. 2012;43(6):976–9.21236613 10.1016/j.jemermed.2010.11.031 · doi ↗ · pubmed ↗
- 8Farouji I Chan KH Abed Het al. Cerebral air embolism after gastrointestinal procedure: a case report and literature review. J Med Cases. 2021;12(3):119–25.34434442 10.14740/jmc 3639 PMC 8383579 · doi ↗ · pubmed ↗