Ascending Colon Schwannoma: A Rare Submucosal Tumour
Kugendran Ponniah, Larissa Yong, Abdul Rana, Christopher McDonald

TL;DR
A 60-year-old woman with a rare colon tumor called schwannoma was successfully treated with robotic surgery and fully recovered.
Contribution
This case report highlights a rare occurrence of schwannoma in the ascending colon and its successful robotic treatment.
Findings
Schwannoma was diagnosed in the ascending colon through histological and immunohistochemical analyses.
Robotic-assisted right hemicolectomy led to a complete recovery in the patient.
The case underscores the importance of accurate diagnosis for rare submucosal tumors.
Abstract
We present a rare case of schwannoma in the ascending colon of a 60-year-old female with dyslipidemia. A series of diagnostic procedures, including colonoscopy and CT colonography, led to the successful robotic-assisted right hemicolectomy. Histological and immunohistochemical analyses confirmed the diagnosis of schwannoma, and the patient achieved a complete recovery post-surgery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
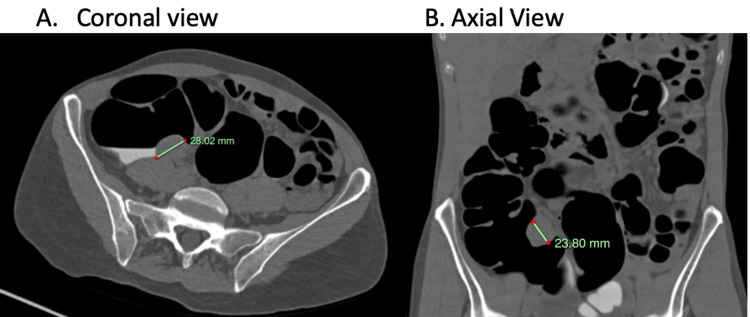 Figure 1
Figure 1 Figure 2
Figure 2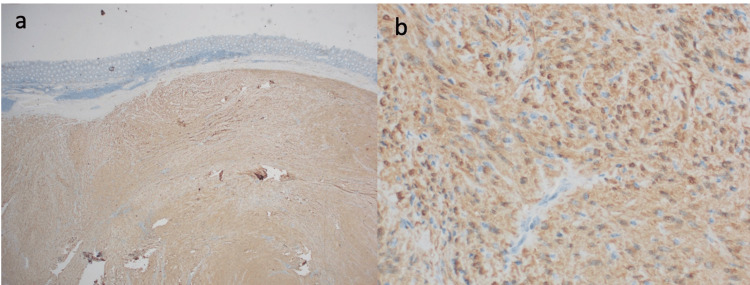 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Neurofibromatosis and Schwannoma Cases · Gastrointestinal disorders and treatments
Introduction
Schwannomas, though infrequent in the gastrointestinal tract, can present diverse clinical challenges. Our case highlights a unique manifestation of schwannoma in the ascending colon, an unusual location for this type of tumour [1]. Through a combination of diagnostic investigations and surgical intervention, we navigated the challenges posed by this condition, emphasizing the significance of accurate diagnosis and appropriate management strategies.
Case presentation
We present the case of a 60-year-old female with a background of dyslipidaemia, referred by her general practitioner after a positive fecal occult blood test (FOBT). The patient reported experiencing intermittent diarrhea over the past year, accompanied by an unintentional weight loss of 5 kg. Notably, she denied any abdominal pain or rectal bleeding but had a family history of bowel cancer at 80 years of age.
Thus, we proceeded with a colonoscopy which revealed a 35 mm submucosal polypoidal lesion in the ascending colon, and subsequent biopsies confirmed the benign nature of the lesion, although submucosa evaluation was not possible due to the sampling limitation.
Subsequently, a CT colonography was done that demonstrated a 28 x 23.8 mm circumscribed ovoid soft tissue lesion on the posterior wall of the caecum, proximal to the ileocecal (IC) valve, with no evident infiltration of the adjacent pericolic fat, except for a small (5 mm) non-specific pericolic node (Figure 1). Given the differential possibilities, including a gastrointestinal stromal tumour (GIST), leiomyoma, and lymphoproliferative lesions, a robotic-assisted right hemicolectomy with intracorporeal anastomosis was performed.
CT colonography. A 28.02 x 23.8 mm circumscribed ovoid soft tissue lesion on the posterior wall of the caecum
Macroscopically, the ascending colon mucosa exhibited a 34 x 31 x 17 mm submucosal nodule, accompanied by discoloured mucosa (Figure 2). Upon a histological examination, the findings revealed a submucosal proliferation of spindle to ovoid cells with a diverse cellular pattern, along with an associated chronic inflammatory response. This response included the presence of a rich lymphoid cuff, lymphocytes, plasma cells, and a sparse population of mast cells. Additionally, vessels with hyalinized walls were observed, and the lesion appeared to have invaded the muscularis propria. The immunohistochemical analysis displayed diffuse and strong nuclear positivity for S100 proteins, confirming the diagnosis of schwannoma (Figure 3).
A 34 x 31 x 17 mm submucosal nodule
A) H&E stain showing spindle to ovoid cells with a diverse cellular pattern. (B) Tumor immunohistochemistry (IHC) stain for S100 proteins
The post-operative histology indicated a complete resection, and no further treatment was deemed necessary. The patient had an uneventful recovery and was followed up in the clinic after two weeks to discuss the benign nature of the histology report.
Discussion
Schwannomas, a relatively rare type of peripheral nerve sheath tumour in the gastrointestinal (GI) tract, represent a small fraction (2-6%) of all mesenchymal tumours, which suggests their infrequency in clinical practice [1,2]. While GI schwannomas are uncommon, their occurrence in the ascending colon is exceptionally rare, with previous literature emphasizing the rectum as the most prevalent location for benign schwannomas, followed by the right colon [3,4]. Additionally, the slightly higher prevalence among females and their average manifestation during the sixth decade of life highlight the specific demographic trends associated with this rare pathology [5].
Despite their usual asymptomatic progression, some GI schwannomas present with pain, tenesmus, and bleeding, warranting meticulous diagnostic approaches and timely interventions [6,7]. Schwannomas are often found incidentally during regular colonoscopy surveillance or CT scans done for other reasons. They seldom erode the mucosa, typically appearing as submucosal masses or polyps during colonoscopy or CT scans [7,8].
An accurate diagnosis relies on the immunohistopathological examination of the surgically removed specimen. When observed macroscopically, these tumours typically manifest as distinct, well-defined masses with several lobulated areas, occasionally exhibiting mucosal ulceration. Schwannomas exhibit positive S100 staining while they display negative staining for various markers, including DOG1, SMA, desmin, CD 117, CD-34, and c-KIT, aiding in their differentiation from other mesenchymal cells [9,10].
Although schwannomas generally exhibit a benign and indolent clinical course, the potential for incomplete excision leading to recurrence and rare instances of malignant transformation emphasize the necessity for comprehensive surgical resection with negative margins [11].
Attaining complete surgical resection with tumour-free margins is considered the most effective therapeutic strategy. Incomplete surgical resection and insufficient margins are often implicated in tumour recurrence. Adjuvant therapies are generally not recommended when negative margins are successfully achieved through surgery [12].
Conclusions
In cases where a growth is seen during colonoscopy, accurately diagnosing schwannomas through biopsy poses significant challenges and carries the risk of a missed diagnosis. Consequently, surgical intervention becomes imperative to definitively determine the benign nature of the growth and ensure that the tumour is completely excised to prevent a recurrence. In addition to that, a clear examination of the removed tissue under a microscope, especially looking for S100, is crucial for confirming the diagnosis of schwannomas. Given the benign nature of this pathology, a complete resection would be adequate without further need for chemotherapy and radiotherapy post surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastrointestinal schwannomas: a rare but important differential diagnosis of mesenchymal tumors of gastrointestinal tract BMC Surg Mekras A Krenn V Perrakis A 471820183004573910.1186/s 12893-018-0379-2PMC 6060462 · doi ↗ · pubmed ↗
- 2Schwannoma of the colon and rectum: a systematic literature review World J Surg Oncol Bohlok A El Khoury M Bormans A 1251620182997007510.1186/s 12957-018-1427-1PMC 6029403 · doi ↗ · pubmed ↗
- 3Schwannoma of the colon Case Rep Gastroenterol Nonose R Lahan AY Santos Valenciano J Martinez CA 293299320092110324410.1159/000237736 PMC 2988920 · doi ↗ · pubmed ↗
- 4Solitary schwannoma of the colon: report of two cases Surg Today Inagawa S Hori M Shimazaki J 8338383120011168656810.1007/s 005950170060 · doi ↗ · pubmed ↗
- 5Cecal schwannoma: a rare cause of gastrointestinal bleeding in a young woman with a review of literature Gastroenterol Res Pract Kanneganti K Patel H Niazi M Kumbum K Balar B 142781201120112176077310.1155/2011/142781 PMC 3132483 · doi ↗ · pubmed ↗
- 6A case of benign schwannoma of the transverse colon with granulation tissue Case Rep Gastroenterol Tsunoda C Kato H Sakamoto T 116120320092065197610.1159/000214837 PMC 2895187 · doi ↗ · pubmed ↗
- 7Cellular neurilemoma (schwannoma) of the descending colon mimicking carcinoma: report of a case Dis Colon Rectum Skopelitou AS Mylonakis EP Charchanti AV Kappas AM 11931196411998974950510.1007/BF 02239444 · doi ↗ · pubmed ↗
- 8Gastrointestinal: asymptomatic colonic schwannoma in an elderly woman; a rare case J Gastroenterol Hepatol Tanaka T Ishihara Y Takabayashi N Kobayashi R Hiramatsu T Kuriki K 13392620112177106110.1111/j.1440-1746.2011.06677.x · doi ↗ · pubmed ↗