An Amyand Hernia With Concurrent Appendicitis Secondary to a Neuroendocrine Neoplasm: A Case Report
Jason Zouki, Anoj Dharmawardhane

TL;DR
A rare case of a 15-year-old with appendicitis in an inguinal hernia caused by a neuroendocrine tumor is reported, highlighting the importance of considering cancer in such diagnoses.
Contribution
This case report presents a rare combination of Amyand’s hernia, appendicitis, and a neuroendocrine tumor, emphasizing diagnostic and management considerations.
Findings
A neuroendocrine tumor was identified as the cause of appendicitis within an inguinal hernia in a 15-year-old male.
Curative treatment with caecectomy showed no residual malignancy after surgery.
The case highlights the need to consider underlying malignancy in atypical appendicitis presentations.
Abstract
Amyand’s hernia (AH) describes the rare instance of a vermiform appendix within an inguinal hernia. Primary appendiceal neoplasms are also rare with the majority of cases being found incidentally during routine histopathology. This case reports the management of a 15-year-old male, who presented to the emergency department with acute appendicitis located within an indirect right inguinal hernia, which was ultimately secondary to a neuroendocrine tumor (NET) with serosal involvement. Intraoperative findings included macroscopic appendicitis with no evidence of perforation. Histopathology returned as a neuroendocrine tumor (pT4) with involved proximal margin and curative treatment was undertaken with a caecectomy which returned no residual malignancy. Key considerations include management options of peritoneal spread within the inguinal canal and recommended management NET in the context…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
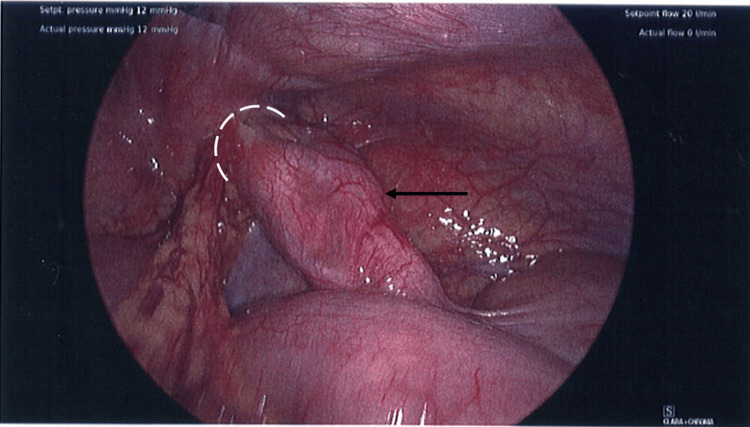 Figure 1
Figure 1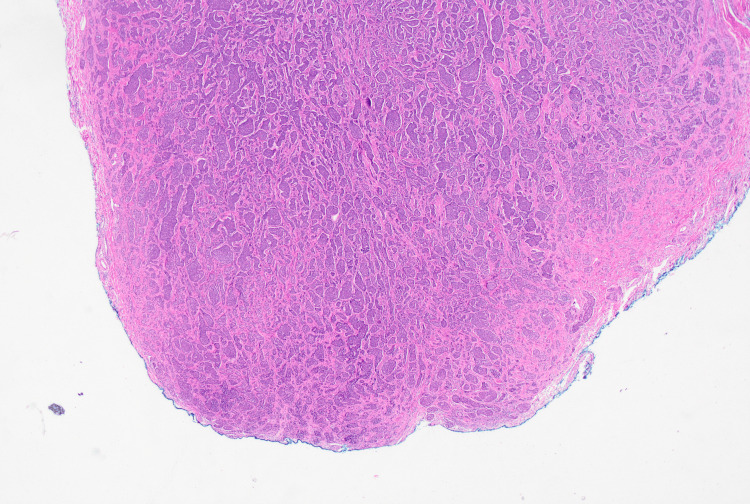 Figure 2
Figure 2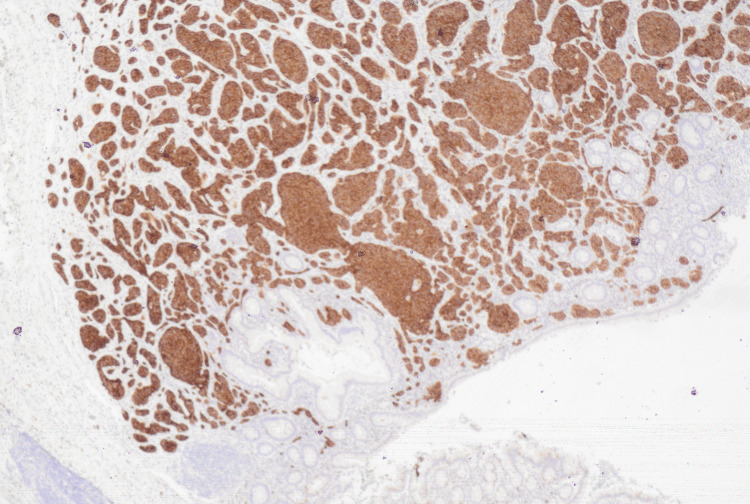 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Neuroendocrine Tumor Research Advances · Appendicitis Diagnosis and Management
Introduction
Amyand’s hernia (AH) describes the presence of the vermiform appendix in an inguinal hernia and accounts for 0.1% of all cases of appendicitis and 0.4% to 0.6% of all cases of inguinal hernias [1]. AH occur due to a patent processus vaginalis and are up to three times more common in the paediatric population, with the overwhelming majority identified in males or in females who are post-menopausal [2]. The underlying pathophysiology is not clearly understood, however the presence of a congenital fibrous band between the appendix and scrotum has been proposed as an underlying cause [2]. AH have a poor rate of pre-operative identification due to the varied clinical presentation and low detection rates on ultrasound [3]. The presence of macroscopic inflammation at the time of appendicectomy increases the rate of post-operative infection to around 5% and should be a key determinant of the type of hernia repair [2].
Primary appendiceal neoplasms are rare entities with diverse pathophysiology and a wide spectrum of mortality based on the tumour type and staging. Appendiceal malignancies are defined by the World Health Organisation (WHO) classification into epithelial (mucinous, non-mucinous adenocarcinoma, and signet ring cell tumors) and non-epithelial lesions (neuroendocrine tumours [NETs], lymphomas, and sarcomas) [4]. Appendiceal NETs account for 65% of appendiceal tumours, but are only found in 0.5% to 1% of all appendicectomies, the majority of which are incidental [5].
Case presentation
A 15-year-old male presented to the emergency department with 24 hours of migratory pain to the right iliac fossa, subjective fevers and anorexia consistent with a clinical diagnosis of acute appendicitis. He denied any associated bowel changes, weight loss, dysuria, testicular pain or new groin masses. The patient’s past medical history was limited to autism and his surgical history consisted of an open left inguinal herniotomy at the age of 10 for an indirect inguinal hernia. On review he was tachypneic to 24 in the context of pain, but afebrile with a heart rate of 80 beats per minute and regular. Abdominal examination revealed right iliac fossa tenderness with a positive Rovsing sign, but no hernia was detected. Initial investigations revealed a normal white cell count of 10.0 x 10^9/L with an elevated C-reactive protein of 55 mg/L. The remainder of the blood tests were unremarkable including a full blood count, liver function test, urea and electrolytes. The patient was diagnosed with appendicitis based on history and clinical findings and progressed to a laparoscopic appendicectomy with no pre-operative imaging.
Intraoperatively, an AH was found with macroscopic appendicitis within an indirect inguinal hernia (Figure 1), however no intra-abdominal free fluid or evidence of perforation was found. The previous hernia repair was intact and the decision was made to not proceed with a right inguinal hernia repair secondary to the presence of macroscopic inflammation and a risk of bacterial translocation with subsequent mesh infection.
Intraoperative picture showing macroscopic appendicitis with an Amyand herniaWhite semicircle: Indirect (right) inguinal herniaBlack arrow: Appendix with macroscopic inflammation
The patient was discharged the following morning with no concerns, however he presented one week later with loose stools and generalised abdominal pain. A computerized tomography (CT) scan failed to demonstrate any intra-abdominal collections or post-operative complications and he was managed with a course of oral antibiotics after a stool specimen confirmed the presence of Clostridium difficile. Appendiceal histology returned the following week, demonstrating ‘acute appendicitis with a well-differentiated neuroendocrine neoplasm in the proximal appendix and possible proximal margin involvement (Figure 2). The maximum tumour diameter is 11mm with invasion through the muscularis propria (Figure 3) into subserosa (pT4) and a Ki-67 index less than 1%’.
Haemotoxylin and Eosin stain of the appendix showing serosal involvement (pT4 staging)
Histopathology slide with chromogranin A-stained appendix showing neuroendocrine tumour in brown
A chromogranin A level returned normal and a DOTATATE Positron Emission Tomography (PET) scan revealed an avid right inguinal lymph node, however there were no features of nodal malignancy on the ultrasound scan and the scan was otherwise unremarkable. A multi-disciplinary team meeting was held with the surgical and oncological team regarding benefits of a caecectomy against a limited right hemicolectomy. The patient was followed up in the outpatient setting with his family, and he decided to proceed with a caecectomy which returned with no residual malignancy. A post-operatively colonoscopy one month after his caecectomy was unremarkable with nil lesions identified, and the patient underwent a clinical review at six months which was unremarkable. He was discharged from clinic with a curative prognosis and no further follow-up required.
Discussion
Appendicitis is a common surgical presentation commonly managed via laparoscopic appendicectomy. The presence of an inflamed appendix within an inguinal hernia is rare and accounts for only 0.1% of appendicectomies. Neoplasms of the appendix are also rare entities and are found in less than 2% of all appendicectomies [6], with only 0.3% - 0.9% diagnosed as a NET. Losanoff and Basson have proposed a classification for surgical management of AH, however the varied approaches are heavily reliant on pre-operative identification of AH, which is considered difficult to diagnose [7].
The management of a NET is well described, and dependent on the size of the neoplasm as well as the presence of high-risk features, including mesoappendiceal involvement, location at the base of the appendix, Ki-67 >2%, angioinvasion, neuroinvasion or involved surgical margins [8]. Given the involved margin and proximal location at the base of the appendix, definitive treatment with a right hemicolectomy, or yearly cross-sectional imaging with CT or Magnetic Resonance Imaging (MRI) is suggested. Of note, the patient was initially staged as pT4NxMx (Histopathology slide 4), requiring consideration of peritoneal carcinomatosis, which has been reported as commonly as 10% to 33% of NET [9]. In the presence of a well-differentiated malignancy, with a Ki-67% <1% and a reassuring CT/PET, the decision was made to manage the inguinal canal expectantly. Interestingly, despite a high rate of nodal involvement around 47% in NET between 1-2cm, Rossi and Patel report a 0% recurrence rate if the primary lesion is <2cm [10]. Definitively, a caecectomy was planned with curative intent to resect the involved margin and avoid the likely unnecessary morbidity of a right hemicolectomy.
Furthermore, the patient underwent a colonoscopy post-operatively to exclude synchronous lesions, which are present in up to 22% of patients with a NET [10], however this was unremarkable with no lesions identified.
Conclusions
Appendicitis is a common surgical presentation which may is typically managed via laparoscopic resection. Understanding of the varied ways in which it may present and the best proposed management outcomes it critical. Occasionally it may present as part of a secondary condition, such as AH and a differential diagnosis in the underlying cause must always include malignancy. Furthermore, an understanding of proposed surgical managements as reported by Losanoff and Basson may help with preoperatively planning during these rare cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amyand's hernia: a review Am J Surg Michalinos A Moris D Vernadakis S 98999520720142428014810.1016/j.amjsurg.2013.07.043 · doi ↗ · pubmed ↗
- 2Amyand's hernia in premature twins Hernia Baldassarre E Centonze A Mazzei A Rubino R 2292301320091879178010.1007/s 10029-008-0427-4 · doi ↗ · pubmed ↗
- 3Amyand's hernia: a review Med Sci Monit Ivanschuk G Cesmebasi A Sorenson EP Blaak C Loukas M Tubbs SR 1401462020142447337110.12659/MSM.889873 PMC 3915004 · doi ↗ · pubmed ↗
- 4Management of incidentally discovered appendiceal neuroendocrine tumors after an appendicectomy World J Gastroenterol Muñoz de Nova JL Hernando J Sampedro Núñez M 13041314282022 http://10.3748/wjg.v 28.i 13.13043564554410.3748/wjg.v 28.i 13.1304 PMC 9099182 · doi ↗ · pubmed ↗
- 5The 2019 WHO classification of tumours of the digestive system Histopathology Nagtegaal ID Odze RD Klimstra D 1821887620203143351510.1111/his.13975 PMC 7003895 · doi ↗ · pubmed ↗
- 6Risk of appendiceal cancer in patients undergoing appendectomy for appendicitis in the era of increasing nonoperative management J Surg Oncol Lu P Mc Carty JC Fields AC 45245912020193127082410.1002/jso.25608 · doi ↗ · pubmed ↗
- 7Amyand hernia: a classification to improve management Hernia Losanoff JE Basson MD 3253261220081821463710.1007/s 10029-008-0331-y · doi ↗ · pubmed ↗
- 8Appendiceal neuroendocrine neoplasms: diagnosis and management Endocr Relat Cancer Alexandraki KI Kaltsas GA Grozinsky-Glasberg S Chatzellis E Grossman AB 04123201610.1530/ERC-15-031026483424 · doi ↗ · pubmed ↗