Radiation therapy of breast cancer in the Nahe Breast Center: first results of an analysis in the context of health services research
Ralph Mücke, Gabor Heim, Robert Gosenheimer, Volker Schmitz, Christoph Schulz, Per Knoeß, Khashayar Fakhrian, Christina Harvey, Christiane Mücke, Gabriele Lochhas, Ute Metzmann, Matthias Bussmann, Markus Paschold

TL;DR
This paper reports on the effectiveness of radiation therapy for breast cancer at the Nahe Breast Center, showing low recurrence rates and good survival outcomes.
Contribution
The study provides new local recurrence and survival data from a specific breast cancer center's radiotherapy outcomes.
Findings
Local recurrence rate was 2.9% with a 97.1% 5-year recurrence-free survival.
Only 5.8% of patients developed distant metastasis, and 5.1% died from their tumors.
No severe radiogenic side effects (grade 3 or 4) were observed.
Abstract
The first evaluation of radiotherapy results in patients with breast cancer treated as part of a multimodal oncologic therapy in the Nahe Breast Center is presented. Analysis of the results was performed using an in-practice registry. From September 2016 to December 2017, 138 patients (median age 62.5 years; range 36–94 years) with breast cancer (right side, n = 67; left side, n = 71) received adjuvant radiation therapy. Of these, 103 patients received gyneco-oncologic care at the Nahe Breast Center, and 35 were referred from outside breast centers. The distribution into stages was as follows: stage I, n = 48; stage II, n = 68; stage III, n = 19; stage IV, n = 3. Neoadjuvant chemotherapy was given to 19 and adjuvant chemotherapy to 50 patients. Endocrine treatment was given to 120 patients. Both 3D conformal (n = 103) and intensity-modulated (n = 35) radiotherapy were performed with a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
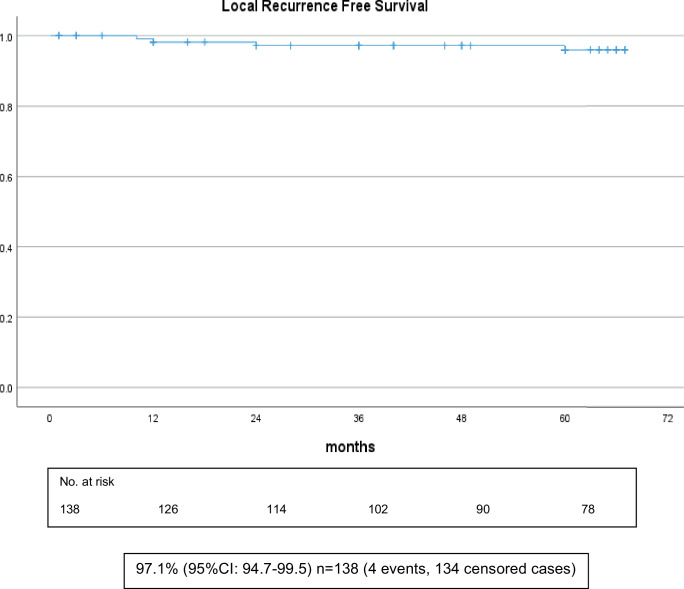 Figure 1
Figure 1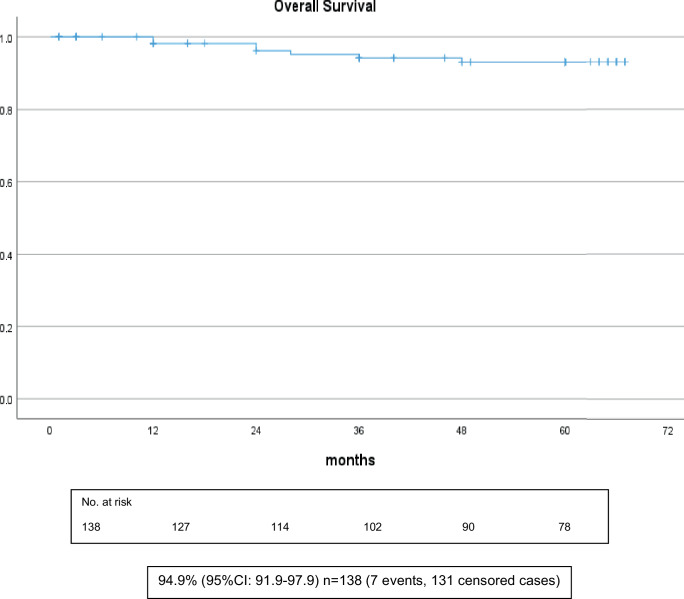 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Global Cancer Incidence and Screening · Cancer Risks and Factors
Introduction
This study is an initial evaluation of adjuvant radiation as part of the multimodal therapy of patients with breast cancer treated at the Nahe Breast Center in Bad Kreuznach. The study was performed to evaluate the quality of the treatment internally and to compare it with the results of national and international studies. The analysis is considered very important in identifying any deviations so they can be corrected if necessary. Data were collected using an internal practice registry in radiotherapy, which was kept in a disciplined manner over the years for all patients. Parameters such as type of surgery and systemic therapy were included. To ensure a sufficient follow-up period, only patients who received radiation from September 2016 to the end of 2017 were included in the analysis.
Patients and methods
From September 2016 to December 2017, 138 patients (median age 62.5 years; range 36–94 years) with breast cancer (right side, n = 67; left side, n = 71) received adjuvant radiation therapy. Of these, 103 patients received gyneco-oncologic care at the Nahe Breast Center, and 35 were referred from outside breast centers. The distribution into stages was as follows: stage I, n = 48; stage II, n = 68; stage III, n = 19; stage IV, n = 3. Neoadjuvant chemotherapy was given to 19 and adjuvant chemotherapy to 50 patients. Endocrine treatment was given to 120 patients.
Radiation therapy was performed with a modern linear accelerator from Elekta (Stockholm, Sweden). All modern radiation techniques such as 3D conformal radiation (n = 103) and intensity-modulated radiation (IMRT; n = 35) were used. Radiation therapy target volumes and total doses were determined in each case according to the national S3 guideline, with each individual case discussed in an interdisciplinary tumor conference prior to the start of radiation. The median total radiation dose after breast-conserving surgery (n = 107) was 62 Gy (50–66), and after mastectomy (n = 31) it was 50 Gy (40–60).
The distribution of patient and radiation criteria is given in Tables 1 and 2.Table 1. Patient dataT‑stageT01/138(0.7%)T175/138(54.4%)T245/138(32.6%)T313/138(9.4%)T44/138(2.9%)N‑stageN091/138(65.9%)N131/138(22.5%)N212/138(8.7%)N34/138(2.9%)GradingG124/138(17.4%)G279/138(57.2%)G335/138(25.4%)Receptor statusER+/PR+120/138(87.0%)ER−/PR−18/138(13.0%)HER-2/neu statusNegative126/138(91.4%)Positive12/138(8.6%)Lymph node surgerySentinel Node98/138(71.0%)Axilla-Dissection40/138(29.0%)SurgeryBreast Conserving107/138(77.5%)Ablatio31/138(22.5%)Resection statusR0138/138(100.0%)T-stage tumor size, N-stage lymph node involvement, HER-2/neu status human epidermal growth factor receptor type 2Table 2Radiation dataFractionationHypofractionated4/138(2.9%)Normofractionated134/138(97.1%)RT technique3D103/138(74.6%)IMRT35/138(26.4%)BoostSimultaneous85/138(61.6%)Sequential17/138(12.3%)No Boost36/138(26.1%)RT of lymph nodesYes48/138(34.8%)No90/138(65.2%)IMRT intensity-modulated radiation therapy, 3D three-dimensional conformal radiation therapy, RT radiation therapy
Statistics
All data were stored and analyzed using the SPSS statistical package 29.0 (IBM. Corp., Armonk, NY, USA). Descriptive statistics were computed for continuous and categorical variables. The statistics computed included median and interquartile ranges of ordinal variables, means and standard deviations of continuous variables, and frequencies and relative frequencies of categorical factors. The period to death or recurrence or last follow-up was estimated with the Kaplan–Meier method. Differences between curves were assessed by the Mantel log-rank test for censored survival data. All p-values were from two-sided statistical tests, and values of p < 0.05 were considered statistically significant.
Results
With a median follow-up of 60 months (1–67), local recurrence occurred in 4/138 (2.9%) and distant metastasis in 8/138 (5.8%) patients; 7/138 (5.1%) patients died of their tumors during the follow-up period.
Local recurrence-free survival
The actuarial 5‑year local recurrence-free survival of all patients was 97.1% (Fig. 1).Fig. 1. Local recurrence-free survival of all patients (n = 138)
Overall survival
The actuarial 5‑year overall survival of all patients was 94.9% (Fig. 2). Further calculated survival data are shown in Tables 3 and 4.Fig. 2. Overall survival of all patients (n = 138)Table 3. Local recurrence-free survival data depending on endocrine therapy, chemotherapy, and gradingWith endocrine therapyn = 1201 event, 119 censored cases99.2% (95% CI: 97.8–100.6)p < 0.001Without endocrine therapyn = 183 events, 15 censored cases83.3% (95% CI: 69.8–96.8)Without chemotherapyn = 690 events, 69 censored cases100.0%^a^p < 0.001With adjuvant chemotherapyn = 501 event, 49 censored cases98.0% (95% CI: 94.7–101.3)With neoadjuvant chemotherapyn = 193 events, 16 censored cases84.2% (95% CI: 69.5–98.9)Grade 1n = 240 events, 24 censored cases100.0%^a^p < 0.001Grade 2n = 790 events, 79 censored cases100.0%^a^Grade 3n = 354 events, 31 censored cases88.6% (95% CI: 77.7–98.6)CI confidence intervals^a^No CI are calculated because all cases are censoredTable 4Overall survival data depending on endocrine therapy, chemotherapy, and gradingWith endocrine therapyn = 1205 events, 115 censored cases95.8% (95% CI: 92.8–98.8)p = 0.201Without endocrine therapyn = 182 events, 16 censored cases88.9% (95% CI: 77.7–100)Without chemotherapyn = 690 events, 69 censored cases100.0%^a^p = 0.019With adjuvant chemotherapyn = 505 events, 45 censored cases90.0% (95% CI: 84.2–95.8)With neoadjuvant chemotherapyn = 192 events, 17 censored cases89.5% (95% CI: 73.1–105.9)Grade 1n = 240 events, 24 censored cases100.0%^a^p < 0.039Grade 2n = 793 events, 76 censored cases96.2% (95% CI: 93.0–99.4)Grade 3n = 354 events, 31 censored cases88.6% (95% CI: 78.1–99.1)*CI *confidence intervals^a^No CI are calculated because all cases are censored
Toxicity data are shown in Tables 5 and 6.Table 5. Toxicity data at the end of radiotherapyRadiation dermatitisGrade 024/138(17.4%)Grade 1100/138(72.5%)Grade 214/138(10.1%)Grade 30/138(0%)Grade 40/138(0%)Breast painGrade 0125/138(90.6%)Grade 19/138(6.5%)Grade 24/138(2.9%)Grade 30/138(0%)Grade 40/138(0%)FatigueGrade 059/138(42.7%)Grade 171/138(51.5%)Grade 28/138(5.8%)Grade 30/138(0%)Grade 40/138(0%)PneumonitisGrade 0135/138(97.8%)Grade 13/138(2.2%)Grade 20/138(0%)Grade 30/138(0%)Grade 40/138(0%)Table 6. Toxicity data during follow-upFibrosisGrade 0113/138(81.9%)Grade 121/138(15.2%)Grade 24/138(2.9%)Grade 30/116(0%)Grade 40/116(0%)HyperpigmentationGrade 098/138(71.0%)Grade 134/138(24.6%)Grade 26/138(4.4%)Grade 30/138(0%)Grade 40/138(0%)Lymphedema breastGrade 0120/138(87.0%)Grade 112/138(8.7%)Grade 26/138(4.3%)Grade 30/138(0%)Grade 40/138(0%)Lymphedema armGrade 0128/138(92.7%)Grade 17/138(5.1%)Grade 23/138(2.2%)Grade 30/138(0%)Grade 40/138(0%)Lung fibrosisGrade 0135/138(97.8%)Grade 13/138(2.2%)Grade 20/138(0%)Grade 30/138(0%)Grade 40/138(0%)
Discussion
Our results of breast cancer irradiation in the context of multimodal therapy are in line with nationally and internationally published results. In particular, the 5‑year local recurrence rate for all patients in our study, determined absolutely (2.9%) and actuarially (97.1%), is excellent and demonstrates the usefulness of radiotherapy. It also shows the high professional and technical quality of all employees in our practice. The results confirm that postoperative radiation is the most important and effective measure to reduce the risk of local recurrence [1–12]. If we follow the current literature, this finding applies to all breast cancer subgroups. Thus, all women should be presented for radio-oncology after breast-conserving surgery, and predictive markers for decision-making cannot be relied on.
The currently published PRIME II trial also demonstrates these excellent local effects of radiation, although the authors recommend against radiation for women older than 65 years with hormone receptor positivity after breast-conserving surgery if they consistently take antiestrogenic medication for 5 years. In this study, the local recurrence rate of this group of patients after 10 years without radiation was 8.6%, and with radiation it was 1% [13].
Meta-analyses have even shown that local irradiation not only reduces the local recurrence rate but also reduces the rate of distant recurrences [1, 2].
With the use of state-of-the-art irradiation techniques, as we apply them in our center, both pronounced acute and late radiogenic side effects are very rare: no grade 3 and 4 toxicities occurred in our evaluation, and the pneumonitis rate is only 2.2% (Table 5).
Skin toxicity is comparable to currently published data. Pulmonary toxicity is slightly better, but only grade 1 symptomatic pneumonitis was reported in our study. Asymptomatic pneumonitis was not analyzed [14, 15].
A limitation of this study is the still very small number of patients, especially in the subgroups. We are very aware that this analysis is not a prospective randomized trial. The worse outcomes of patients with chemotherapy and with histological grade 3 disease indicate that these groups included patients with more risk factors. For example, only 4/24 patients (16.6%) with a grading of 1 but 33/35 patients (94.3%) with a grading of 3 received chemotherapy. Regarding nodal status, there were 31/91 patients (34.1%) with negative nodal status and 38/47 patients (80.9%) with positive nodal status who received chemotherapy. We will not further discuss the presented subgroups, such as those who did not receive endocrine treatment and did receive chemotherapy and patients with different grades of disease, but we wanted to show them. Nevertheless, we wanted to check the quality of our work for the first time after a follow-up of 5 years.
The results indicate high professional quality in the treatment of breast cancer at the Nahe Breast Center. Through regular training and quality improvement measures, everything is being done to maintain or even improve this high level of quality.
Conclusion
The results of radiotherapy for breast cancer at the Nahe Breast Center are comparable to published national and international results. In particular, the local recurrence rates in our study, determined absolutely and actuarially, are excellent and demonstrate the usefulness of radiotherapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clarke M Collins R Darby S Davies C Elphinstone P Evans V Godwin J Gray R Hicks C James S Mac Kinnon E Mc Gale P Mc Hugh T Peto R Taylor C Wang Y Early Breast Cancer Trialists’ Collaborative Group (EBCTCG)Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials Lancet 200536695032087210610.1016/S 0140-6736(05)67887-716360786 · doi ↗ · pubmed ↗
- 2Darby S Mc Gale P Correa C Taylor C Arriagada R Clarke M Cutter D Davies C Ewertz M Godwin J Gray R Pierce L Whelan T Wang Y Peto R Early Breast Cancer Trialists’ Collaborative Group (EBCTCG)Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials Lancet 201137898041707171610.1016/S 0140-6736(11)61629-222019144 PMC 3254252 · doi ↗ · pubmed ↗
- 3Pötter R Gnant M Kwasny W Tausch C Handl-Zeller L Pakisch B Taucher S Hammer J Luschin-Ebengreuth G Schmid M Sedlmayer F Stierer M Reiner G Kapp K Hofbauer F Rottenfusser APöstlberger S Haider K Draxler W Jakesz R Austrian Breast and Colorectal Cancer Study Group Lumpectomy plus tamoxifen or anastrozole with or without whole breast irradiation in women with favorable early breast cancer Int J Radiat Oncol Biol Phys 200768233434010.1016/j.ijrobp.2006.12.04517363187 · doi ↗ · pubmed ↗
- 4Hughes KS Schnaper LA Bellon JR Cirrincione CT Berry DA Mc Cormick B Muss HB Smith BL Hudis CA Winer EP Wood WC Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343 J Clin Oncol 201331192382238710.1200/JCO.2012.45.261523690420 PMC 3691356 · doi ↗ · pubmed ↗
- 5Kunkler IH Williams LJ Jack WJ Cameron DA Dixon JMPRIME II investigators Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME II): a randomised controlled trial Lancet Oncol 201516326627310.1016/S 1470-2045(14)71221-525637340 · doi ↗ · pubmed ↗
- 6Blamey RW Bates T Chetty U Duffy SW Ellis IO George D Mallon E Mitchell MJ Monypenny I Morgan DA Macmillan RD Patnick J Pinder SE Radiotherapy or tamoxifen after conserving surgery for breast cancers of excellent prognosis: British Association of Surgical Oncology (BASO) II trial Eur J Cancer 201349102294230210.1016/j.ejca.2013.02.03123523089 · doi ↗ · pubmed ↗
- 7Fyles AW Mc Cready DR Manchul LA Trudeau ME Merante P Pintilie M Weir LM Olivotto IA Tamoxifen with or without breast irradiation in women 50 years of age or older with early breast cancer N Engl J Med 20043511096397010.1056/NEJ Moa 04059515342804 · doi ↗ · pubmed ↗
- 8Kauer-Dorner DPötter R Resch A Handl-Zeller L Kirchheiner K Meyer-Schell KDörr W Partial breast irradiation for locally recurrent breast cancer within a second breast conserving treatment: alternative to mastectomy? Results from a prospective trial Radiother Oncol 201210219610110.1016/j.radonc.2011.07.02021907439 · doi ↗ · pubmed ↗