Ticagrelor was associated with lower fracture risk than clopidogrel in the dual anti-platelet regimen among patients with acute coronary syndrome treated with percutaneous coronary intervention
D. T. W. Lui, C. H. Wong, A. Ip, A. K. Y. Ng

TL;DR
Ticagrelor, a blood thinner, was linked to a lower risk of fractures compared to clopidogrel in heart patients undergoing a specific treatment.
Contribution
This study shows ticagrelor reduces major osteoporotic fracture risk compared to clopidogrel in dual anti-platelet therapy.
Findings
Ticagrelor users had 0.34% annual fracture risk versus 0.56% for clopidogrel users.
Ticagrelor was associated with a 40% lower fracture risk (HR 0.60) compared to clopidogrel.
Lower fracture risk with ticagrelor was consistent across different body regions.
Abstract
Patients with coronary artery disease have increased fracture risks. P2Y12 inhibitors may impact fracture risks. We compared the fracture risks associated with ticagrelor and clopidogrel in dual anti-platelet therapy (DAPT). We identified all adults who underwent first-ever percutaneous coronary intervention (PCI) for acute coronary syndrome (ACS) between 2010 and 2017 from a territory-wide PCI registry in Hong Kong. Following 1:1 propensity-score matching for baseline characteristics, patients were followed up till event occurrence, death, or 30 June 2022. Outcomes of interest were major osteoporotic fractures (MOF) identified by validated ICD-9-CM codes. Cox proportional hazards regression was used to compute the hazard ratio (HR) for MOF associated with ticagrelor versus clopidogrel use. 3018 ticagrelor users and 3018 clopidogrel users were identified after propensity-score…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
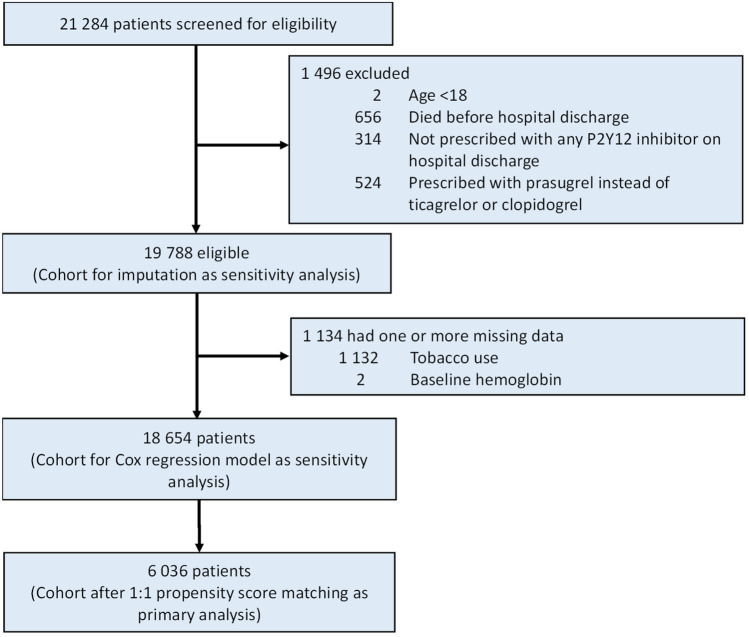 Figure 1
Figure 1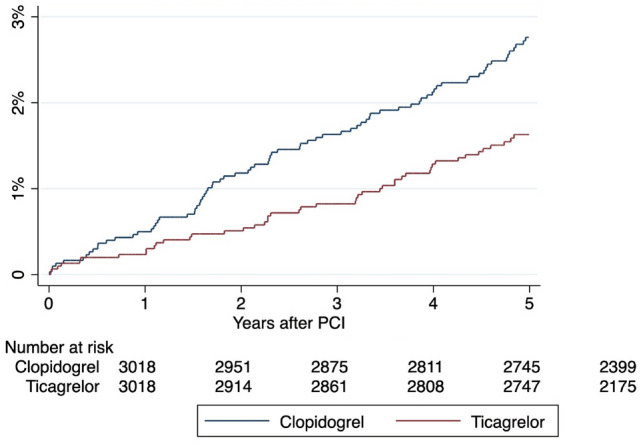 Figure 2
Figure 2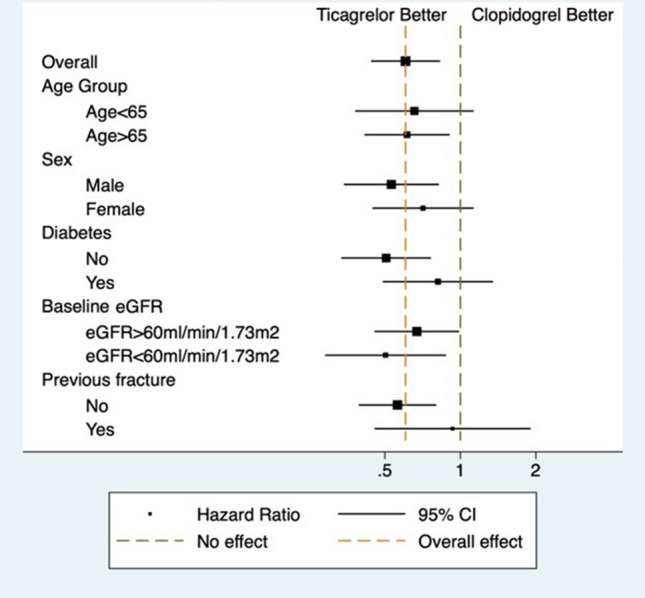 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntiplatelet Therapy and Cardiovascular Diseases · Lipoproteins and Cardiovascular Health · Acute Myocardial Infarction Research
Introduction
Osteoporosis is a global pandemic. It is clinically silent until complications occur, manifesting as fragility fractures [1]. Hip and vertebral fractures are the more devastating types of fragility fractures associated with significant morbidities and mortality [2]. Patients with coronary artery disease (CAD) may be at a higher risk of osteoporosis and fragility fractures, potentially mediated through the common pathophysiological mechanism of atherosclerosis [3, 4]. Furthermore, patients with acute coronary syndrome (ACS) tend to be older with multiple comorbidities, increasing the risk of major osteoporotic fractures (MOF). Impairment in activities of daily living after fractures can lead to significant morbidity, creating substantial functional limitations and reducing patients’ quality of life.
Dual anti-platelet therapy (DAPT), consisting of aspirin and a P2Y12 inhibitor, is the standard of care in patients with ACS following percutaneous coronary intervention (PCI) [5]. Inhibition of platelet aggregation by DAPT is deemed essential in reducing the risk of stent thrombosis and ischemic events such as stroke and peripheral artery disease [6]. Recently, novel agents, namely ticagrelor and prasugrel, have emerged as potent P2Y12 inhibitors with better antithrombotic effects than clopidogrel [7, 8]. Observational studies have demonstrated differences in fracture risks associated with different anti-platelet agents [9]. A cohort study by Jorgensen et al. showed that the risk of fracture was increased by approximately 50% among clopidogrel users compared to non-users [10]. Mechanistically, P2Y12 receptors are expressed not only in platelets but also in osteoblasts. Inhibition of P2Y12 receptors by clopidogrel could lower osteoblastic activity and differentiation, reducing new bone formation and thereby increasing fracture risk [11]. On the other hand, ticagrelor, in addition to P2Y12 inhibition, prevents cellular adenosine uptake by the equilibrative nucleoside transporter (ENT)-1, thereby increasing extracellular adenosine levels [12]. This may promote osteoblastic differentiation and bone formation. There are yet observational studies reporting fracture risks associated with ticagrelor use.
Given the higher fracture risks among patients with CAD [13], it is clinically relevant to evaluate whether clopidogrel or ticagrelor is associated with a better fracture risk profile. Based on the observations in the pre-clinical studies, we hypothesize that ticagrelor use is associated with a lower fracture risk than clopidogrel use. Here, we performed a retrospective cohort study comparing the risk of MOF among Chinese patients who underwent PCI and were subsequently treated with clopidogrel versus ticagrelor in the DAPT regimen.
Methods
Study population and design
All patients who underwent first-ever PCI between 1 January 2010 and 31 December 2017 in any of all 14 public hospitals that performed PCI in Hong Kong were included in a territory-wide PCI registry [14]. Our current study is a retrospective cohort analysis of all adult patients (aged ≥ 18 years) who underwent PCI for ACS and survived beyond hospital discharge. Patients were excluded from the analysis if they were not prescribed ticagrelor or clopidogrel upon discharge. Patients’ baseline comorbidities, laboratory parameters and concomitant medications were retrieved from the PCI Registry and Clinical Data and Analysis Reporting System (CDARS) [14].
The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority (UW 20-176).
Definition of exposure
Patients were stratified according to the P2Y12 inhibitor (ticagrelor versus clopidogrel) prescribed upon hospital discharge. No further cross-over was allowed after the group assignment. Of note, the intravenous form of P2Y12 inhibitor was not available in our locality.
Definition of outcomes
The primary outcome was MOF, defined as any clinical vertebral, hip and upper limb fractures (i.e. proximal humerus and wrist fractures). MOF were identified using ICD-9 CM codes validated in the electronic health record system of the Hong Kong Hospital Authority [15]. The ICD-9 CM coding system was used throughout the follow-up period [16]. Clinical vertebral fractures were identified by 805.x; upper limb fractures by 812.x, 813.x and 814.x; and hip fractures by 820.x. The secondary outcomes were the individual components of the primary outcome.
Statistical analyses
The study cohort consisted of two comparison groups–‘ticagrelor’ and ‘clopidogrel’ groups—generated by 1:1 propensity-score-matching using a caliper of 0.2 times the standard deviation of the logit of the propensity score [17]. All analyses were performed with prespecified endpoints and statistical methods. We constructed a propensity score that predicted the likelihood of ticagrelor versus clopidogrel with variables selected a priori based on data in the published literature and biological plausibility: sex, age, ever tobacco use, diabetes, hypertension, cerebrovascular disease, chronic obstructive pulmonary disease, peripheral vascular disease, previous myocardial infarction (MI), previous heart failure, chronic kidney disease (CKD; defined as estimated glomerular filtration rate [eGFR] < 60 mL/min), anaemia before PCI (defined as haemoglobin < 13 g/dL for men and < 12 g/dL for women), obesity, previous fall event, previous MOF, inflammatory polyarthropathy, use of vitamin D or calcium supplements, use of bisphosphonates or other anti-osteoporosis medications (including raloxifene, denosumab, strontium and teriparatide), and use of proton pump inhibitors. Comparisons were performed using Chi-square tests for categorical variables and Student’s t test or Wilcoxon rank-sum tests for continuous variables. Kaplan–Meier survival curves were constructed for study groups. Cox proportional hazards regression was performed to evaluate the relationship between P2Y12 inhibitors and clinical outcomes as a time-to-first-event analysis from PCI date until death, loss to follow-up or study end date on 30 June 2022. Data management and statistical analyses were performed in Stata software, version 16 (StataCorp LP). Two-sided P values < 0.05 were considered statistically significant.
Sensitivity analyses
The following sensitivity analyses were performed. Firstly, we included all patients before propensity score matching and repeated the primary analysis using the Cox regression model, adjusting for the same set of covariates used to construct the propensity score. Secondly, we used multiple imputation with chained equations to address missing data and repeated the primary analysis on the entire cohort using the same Cox regression model.
Subgroup analyses
We examined any effect modification from subgroups on the relationship between P2Y12 inhibitor use and MOF by introducing interaction terms to the Cox regression model. The subgroups included age (≤ 65 vs > 65 years), sex, presence of diabetes and CKD at baseline, and history of fractures.
Results
A total of 21284 patients were considered for inclusion: 1496 (7.0%) were excluded—age younger than 18 years, died before hospital discharge, not prescribed with P2Y12 inhibitor on hospital discharge, prescribed with prasugrel (instead of ticagrelor or clopidogrel) on hospital discharge. Of the remaining 19788 patients analyzed, 1134 (5.7%) were excluded from the complete case analysis due to missing values in any of the variables used in the propensity score model (Fig. 1). A total of 3018 pairs of patients prescribed either ticagrelor or clopidogrel upon hospital discharge were generated by 1:1 propensity score matching. Baseline characteristics of all patients before and after propensity score matching are shown in Supplementary Table 1 and Table 1, respectively. Before matching, the two groups had significant differences in sex, age, diabetes, hypertension, cerebrovascular disease, previous MI, previous heart failure, CKD, anemia, obesity, and baseline medications. After matching, the two groups were well balanced in the baseline characteristics with standardized differences < 0.1 for all variables (Table 1). In the matched cohort, the mean age was 61.4 ± 11.4 years, with a male predominance (only 15.9% were women). The median follow-up was 6.5 years (IQR: 5.0–7.8).Fig. 1. Study flow diagramTable 1Baseline characteristics of the cohort after 1:1 propensity score matchingCharacteristicsTicagrelorClopidogrelP valueStandardized differenceN30183018Female471 (15.6%)488 (16.2%)0.550.015Age, mean (SD)61.4 (11.3)61.5 (11.6)0.660.011 Age > 651062 (35.2%)1125 (37.3%)0.0920.043Tobacco use1549 (51.3%)1533 (50.8%)0.68– 0.011Diabetes795 (26.3%)810 (26.8%)0.660.011Hypertension1480 (49.0%)1497 (49.6%)0.660.011Cerebrovascular disease162 (5.4%)161 (5.3%)0.95– 0.001Previous myocardial infarction143 (4.7%)162 (5.4%)0.260.029Previous heart failure100 (3.3%)110 (3.6%)0.480.018eGFR in ml/min, mean (SD)81.4 (23.0)79.6 (22.4)0.003– 0.076 eGFR below 60 ml/min492 (16.3%)496 (16.4%)0.890.004Hemoglobin in g/dL, mean (SD)13.8 (1.7)13.6 (1.7) < 0.001– 0.089 Anemia713 (23.6%)701 (23.2%)0.72– 0.009Obesity37 (1.2%)46 (1.5%)0.320.026Previous fall event260 (8.6%)296 (9.8%)0.110.041Previous major osteoporotic fracture122 (4.0%)142 (4.7%)0.210.032Polyarthropathy18 (0.6%)16 (0.5%)0.73– 0.009Medication received0.002 Calcium/vitamin D supplements75 (2.5%)76 (2.5%)0.930.015 Calcium supplements69 (2.3%)76 (2.5%)0.56– 0.015 Vitamin D supplements26 (0.9%)19 (0.6%)0.29– 0.027 Anti-osteoporosis agents7 (0.2%)7 (0.2%)1.00 < 0.001 Bisphosphonates5 (0.2%)5 (0.2%)1.00 < 0.001 Proton pump inhibitors2466 (81.7%)2493 (82.6%)0.360.023SD* standard deviation, eGFR estimated glomerular filtration rate*Anemia: Hemoglobin < 13 g/dL for men, < 12 g/dL for women
Primary outcomes
MOF occurred in 59 (2.0%) patients on ticagrelor and 119 (3.9%) patients on clopidogrel, corresponding to an annualized risk of 0.34% and 0.56%, respectively. The hazard ratio (HR) of MOF associated with ticagrelor use was 0.60 (95% CI, 0.44–0.83; P = 0.002) with reference to clopidogrel use (Table 2 and Fig. 2).Table 2. Annualized risks and hazard ratios of primary and secondary outcomes in the ticagrelor and clopidogrel groupsOutcomesTicagrelor (95% CI)Clopidogrel (95% CI)Hazard ratio (95% CI)P valuePrimary outcome Any major osteoporotic fracture0.34% (0.26–0.44%)0.56% (0.47–0.68%)0.60 (0.44–0.83)0.002Secondary outcomes Vertebral fracture0.06% (0.03–0.11%)0.10% (0.06–0.15%)0.61 (0.29–1.27)0.19 Hip fracture0.14% (0.10–0.21%)0.24% (0.19–0.32%)0.65 (0.40–1.06)0.087 Upper limb fracture0.15% (0.11–0.23%)0.28% (0.22–0.36%)0.53 (0.34–0.85)0.008Fig. 2Estimated probabilities of major osteoporotic fracture stratified by P2Y12 inhibitors
Secondary outcomes
The HR of fractures at individual sites was consistent with the main analysis. While the risk of upper limb fracture was lower in the ticagrelor group reaching statistical significance (HR, 0.53; 95% CI, 0.34–0.85, P = 0.008), the HR of clinical vertebral fractures (HR, 0.61; 95% CI, 0.29–1.27; P = 0.19) and hip fractures (HR, 0.65; 95% CI, 0.40–1.06; P = 0.087) suggested lower fracture risks in the ticagrelor group although not reaching statistical significance, possibly because of the lower event rates (Table 2 and Supplementary Figs. 1–3).
Sensitivity analyses
Both sensitivity analyses were consistent with the results of the main analysis. In the first sensitivity analysis, we analyzed the outcomes of all 18,654 patients with complete information before propensity score matching. After adjusting for potential confounders using the Cox regression model, the risk of any MOF was lower in the ticagrelor group (HR, 0.72; 95% CI, 0.55–0.94; P = 0.017). Similar results were obtained in the analysis of secondary outcomes: HR of fractures at individual fracture sites associated with ticagrelor use—clinical vertebral fracture (HR, 0.78; 95% CI, 0.42–1.46; P = 0.44), upper limb fracture (HR, 0.78; 95% CI, 0.52–1.18; P = 0.25) and hip fracture (HR, 0.64; 95% CI, 0.43–0.97; P = 0.033). In the second sensitivity analysis, we analyzed the outcomes of all 19,788 patients using multiple imputation with chained equations to address missing data. After adjusting for potential confounders using the Cox regression model, the HR of MOF associated with ticagrelor use was 0.73 (95% CI, 0.57–0.95; P = 0.019) with reference to clopidogrel use.
Subgroup analyses
In the subgroup analyses, we did not observe significant interaction in the relationship between P2Y12 inhibitors and MOF across different subgroups—age, sex, presence of diabetes, presence of CKD and history of fractures (Table 3 and Fig. 3).Table 3. Subgroup analysis examining differential effects of P2Y12 inhibitors on the risk of major osteoporotic fracturesSubgroupHazard ratio95% Confidence intervalP value for interactionAge group0.80 ≤ 65 years0.660.381.13 > 65 years0.610.410.91Sex0.34 Male0.530.340.82 Female0.710.451.13Diabetes0.18 No0.510.330.76 Yes0.810.491.35Baseline eGFR0.47 ≥ 60 mL/min0.670.450.99 < 60 mL/min0.500.290.88Previous fracture0.14 No0.560.390.80 Yes0.930.451.90Fig. 3Forest plot showing subgroup analyses of the risks of major osteoporotic fractures
Discussion
This is the first study in the literature addressing the impact of the choice of P2Y12 inhibitor in the DAPT regimen on the risk of MOF. Among patients undergoing PCI for ACS, ticagrelor use was associated with reduced risks of MOF compared with clopidogrel. From the perspective of bone health, ticagrelor may be the preferred agent in the DAPT regimen.
Ticagrelor, a potent P2Y12 inhibitor, has superior efficacy over clopidogrel in treating CAD [18, 19]. In line with the results of the randomized controlled trials, our group has previously reported the superiority of potent P2Y12 inhibitors (predominantly ticagrelor) over clopidogrel in our current post-PCI cohort with a lower hazard of MI (including but not exclusively reinfarction) after PCI in the potent P2Y12 inhibitor group (adjusted HR 0.71; 95% CI 0.59–0.87; P < 0.001) [14]. Therefore, further evaluation of the fracture risk among patients receiving clopidogrel versus ticagrelor in the post-PCI cohort is essential. Patients with ACS undergoing PCI are at an increased risk of fracture per se. Previous observational studies have demonstrated an increased risk of osteoporosis and vertebral fracture following coronary events [3, 18]. Furthermore, given the role of aspirin in DAPT, proton pump inhibitors (PPI) are often co-prescribed with aspirin to reduce the risk of peptic ulcer disease [20]. PPI is a known risk factor for osteoporosis, increasing the risk of osteoporotic fractures [21, 22]. In our cohort, over 80% of the individuals were put on PPI. Overall, we observed an annualized fracture risk of 0.3–0.6%. Given the male preponderance and the relatively young age of the cohort (mean age of around 60 years), this level of fracture risk required attention.
Focusing on patients with ACS treated with first-ever PCI, our study demonstrated a higher risk of MOF with clopidogrel than ticagrelor, favouring using the latter agent in the post-PCI setting. While the association between clopidogrel use and fracture risk has been reported in prior studies [10], there is a lack of relevant studies on potent P2Y12 inhibitors such as ticagrelor. The nationwide cohort study by Jorgensen et al. showed that treatment with clopidogrel was associated with an increased risk of overall fractures and osteoporotic fractures, especially in patients with treatment duration longer than one year [10]. A dose-dependent relationship was also observed, where individuals on higher doses of clopidogrel had an increased risk of fractures [10]. Even though the latest study by Jorgensen et al. revealed no significant association between clopidogrel treatment and fracture risk in patients with stroke and transient ischemic attack [23], that might be explained by the fact that such patients were immobilized in bed for prolonged periods, which reduced the risk of falls and subsequent fractures [23].
The difference in the fracture risk between ticagrelor and clopidogrel users could be understood from the respective effects of the P2Y12 inhibitors on the bone in pre-clinical studies. Syberg et al. showed that clopidogrel delays osteoblast growth and reduces cell viability [24]. The resulting decrease in mature osteoblasts causes a decline in alkaline phosphatase activity and collagen production, inhibiting new bone formation. Furthermore, clopidogrel induces the precursor cells to preferentially differentiate into the adipocytic lineage instead of the osteoblastic lineage, creating a negative bone balance [24]. While P2Y12 receptors are expressed in both osteoblasts and osteoclasts, the effect of clopidogrel on the reduction of osteoclast activity and bone resorption is smaller in magnitude than that on the reduction of osteoblast differentiation and bone formation [24]. Hence, Syberg et al. postulated that prolonged exposure to clopidogrel could negatively impact bone health. On the other hand, the lower fracture risk observed with ticagrelor use could be ascribed to its ability to enhance bone formation via an adenosine-dependent mechanism. Mediero et al. demonstrated that in vivo, direct or indirect stimulation of adenosine A_2A_ receptor (A2AR) by specific agonists or by enhancing endogenous adenosine levels enhances new bone formation and regeneration [25]. Meanwhile, ticagrelor regulates osteoblast and osteoclast function by blocking adenosine uptake, increasing extracellular adenosine levels, thereby stimulating A2AR [12]. A2AR activation modulates the expression of semaphorins 4D (Sema4D) and 3A (Sema3A), which are important regulators of bone homeostasis [26]. Specifically, A2AR stimulation reduces the release of Sema4D by osteoclasts, inhibits Sema4D-mediated osteoclast activation and increases the secretion of Sema3A by osteoblasts [26]. This helps promote osteoblast differentiation and inhibit osteoclast activity, consequently increasing new bone formation.
Secondary analyses revealed consistently lower HR of fractures over vertebrae, hip and upper limbs associated with ticagrelor use. However, the HR of fractures over vertebrae and hip did not reach statistical significance, which may be explained by the lower number of events at these two sites. In the study by Jorgensen et al., fracture risk over different sites (any fractures, hip, forearm and spine) was consistently higher in the clopidogrel-treated group compared to those not treated with clopidogrel [10]. This suggests that the differential effects of clopidogrel versus ticagrelor on the bone are probably systemic. Furthermore, subgroup analyses showed that the observed protective effects of ticagrelor over clopidogrel on fracture risk were consistent across various subgroups, denoting individuals with different fracture risk profiles—age, sex, presence of diabetes and CKD at baseline, and prior history of fractures. Our results suggested the favorable effects of ticagrelor over clopidogrel on bone health across patients with different baseline fracture risks.
There are several limitations in the present study. First, although we applied propensity score matching for various baseline characteristics, including the fracture risk profile of the clopidogrel and ticagrelor groups, the issue of unmeasured confounding and bias could not be entirely excluded given the observational nature of this cohort study. Secondly, bone mineral density measurement and bone turnover markers were not available. Nonetheless, bone mineral density was not the typical determinant of eligibility for various P2Y12 inhibitors. In addition, fracture events were the more important outcomes from patients’ perspective. Thirdly, treatment adherence could not be ascertained like all large-scale pharmacoepidemiologic studies using electronic health databases. Fourthly, as vertebral fractures were not systematically assessed by quantitative vertebral morphometry, we could only identify clinical, but not morphometric, vertebral fractures. Vertebral fractures are frequently asymptomatic [27], so morphometric vertebral fractures would go undetected. This could lead to an underestimation of the number of events of vertebral fractures. Finally, this study was performed among Chinese patients. The results may not be generalizable to patients of other ethnicities.
Conclusion
In this cohort of Chinese patients who underwent PCI for ACS, ticagrelor was associated with a lower risk of MOF than clopidogrel use. Our results support the use of ticagrelor in the DAPT regimen from the perspective of bone health.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 433 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rachner TD Khosla S Hofbauer LC Osteoporosis: now and the future Lancet 20113771276128710.1016/s 0140-6736(10)62349-521450337 PMC 3555696 · doi ↗ · pubmed ↗
- 2Johnell O Kanis JA An estimate of the worldwide prevalence and disability associated with osteoporotic fractures Osteoporos Int 2006171726173310.1007/s 00198-006-0172-416983459 · doi ↗ · pubmed ↗
- 3Syu DK Hsu SH Yeh PC Kuo YF Huang YC Jiang CC The association between coronary artery disease and osteoporosis: a population-based longitudinal study in Taiwan Arch Osteoporos 2022179110.1007/s 11657-022-01128-335804272 PMC 9270282 · doi ↗ · pubmed ↗
- 4Laroche MPécourneau V Blain H Breuil V Chapurlat R Cortet B Osteoporosis and ischemic cardiovascular disease Joint Bone Spine 20178442743210.1016/j.jbspin.2016.09.02227838246 · doi ↗ · pubmed ↗
- 5Cuisset T Verheugt FWA Mauri L Update on antithrombotic therapy after percutaneous coronary revascularisation Lancet 201739081082010.1016/s 0140-6736(17)31936-028831996 · doi ↗ · pubmed ↗
- 6Valgimigli M Bueno H Byrne RA Collet JP Costa F Jeppsson A 2017 ESC focused update on dual anti-platelet therapy in coronary artery disease developed in collaboration with EACTS: the task force for dual anti-platelet therapy in coronary artery disease of the European society of cardiology (ESC) and of the European association for cardio-thoracic surgery (EACTS)Eur Heart J 20183921326010.1093/eurheartj/ehx 41928886622 · doi ↗ · pubmed ↗
- 7Wiviott SD Braunwald E Mc Cabe CH Montalescot G Ruzyllo W Gottlieb S Prasugrel versus clopidogrel in patients with acute coronary syndromes N Engl J Med 20073572001201510.1056/NEJ Moa 070648217982182 · doi ↗ · pubmed ↗
- 8Wallentin L Becker RC Budaj A Cannon CP Emanuelsson H Held C Ticagrelor versus clopidogrel in patients with acute coronary syndromes N Engl J Med 20093611045105710.1056/NEJ Moa 090432719717846 · doi ↗ · pubmed ↗