Clinical Characteristics and Microorganisms Isolated in Community-Acquired Pneumonia in the COVID-19 Period
Meritxell Gavalda, Maria Isabel Fullana, Adrià Ferre, Rebecca Rowena Peña, Julen Armendariz, Orla Torrallardona, Aina Magraner, Alejandro Lorenzo, Carles García, Gemma Mut, Lluís Planas, Carla Iglesias, Pablo Fraile-Ribot, Maria Dolores Macia Romero, Melchor Riera

TL;DR
This study examines the causes and outcomes of community-acquired pneumonia during the COVID-19 pandemic and evaluates the effectiveness of molecular tests in identifying pathogens.
Contribution
The study provides insights into the clinical and microbiological characteristics of pneumonia during the pandemic and assesses a molecular diagnostic test's utility.
Findings
Streptococcus pneumoniae was the most common isolate in community-acquired pneumonia cases.
The molecular test (FilmArray) had a low positivity rate and mainly detected viral coinfections.
A high NEWS2 score, oncohematological disease, and chronic neurological conditions were linked to worse outcomes.
Abstract
Community-acquired pneumonia is a leading cause of mortality and hospital admissions. The aetiology remains unknown in 30–65% of the cases. Molecular tests are available for multiple pathogen detection and are under research to improve the causal diagnosis. We carried out a prospective study to describe the clinical characteristics and aetiology of community-acquired pneumonia during the COVID-19 pandemic and to assess the diagnostic effectivity of the microbiological tests, including a molecular test of respiratory pathogens (FilmArray™ bioMérieux). From the 1st of February 2021 until the 31st of March 2022, 225 patients were included. Failure in microorganism identification occurred in approximately 70% of patients. Streptococcus pneumoniae was the most common isolate. There were 5 cases of viral pneumonia. The tested FilmArray exhibited a low positivity rate of 7% and mainly aided…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
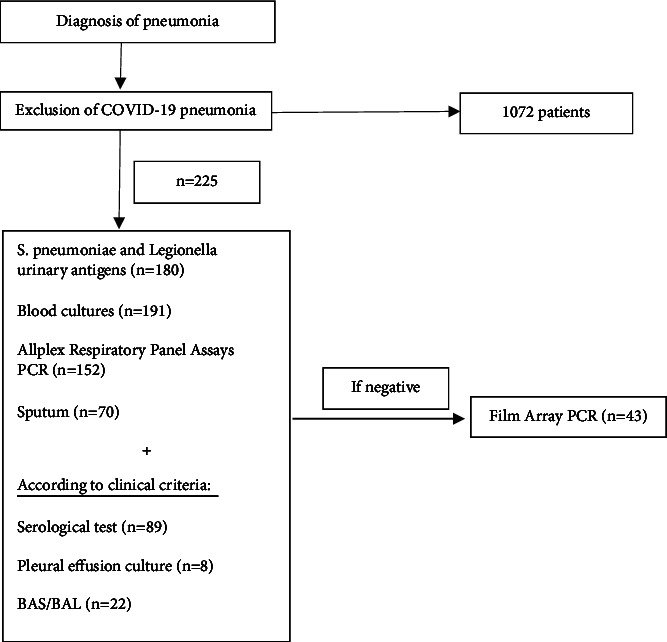 Figure 1
Figure 1- —Departments of Internal Medicine and Microbiology
- —CRUE-CSUC Gold
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Respiratory viral infections research · Nosocomial Infections in ICU
1. Introduction
Community-acquired pneumonia is a leading cause of hospital admissions and mortality. Its incidence in adults ranges between 3 and 20 cases per 1000 inhabitants per year [1]. Before the COVID-19 pandemic, it caused approximately 23,000 annual deaths in the European Union, corresponding to 6% of total mortality [2]. About 30–65% of the causes of pneumonia remain unknown [3, 4]. Finding the cause of pneumonia can be useful in various situations. It can help detect resistant pathogens, guide antibiotic therapy, recognise public health implications for certain pathogens like Legionella, adjust initial empirical therapy when it fails, and track changes in the epidemiology of pneumonia [5, 6].
Several studies have demonstrated the prognostic value of identifying the cause of pneumonia. For example, Uematsu et al. found that following microbiological testing guidelines (sputum, blood cultures, and urine antigen tests) on the first day of hospitalization was associated with lower mortality and shorter hospital stays [7]. Similarly, Costantini et al. demonstrated that performing guideline-recommended urinary antigen tests was associated with lower odds of in-hospital mortality and 30-day mortality [8]. Fullana Barceló et al. found that a delayed diagnosis of influenza infection was related to clinical complications [9]. However, some studies have failed to prove the prognostic value of microbiological testing [10–13], although these studies focused on a single microbiological test (sputum, urinary antigen, or blood culture) and not combined testing.
The 2019 IDSA guidelines recommend obtaining sputum cultures, blood cultures, and Legionella and Pneumococcal urinary antigen tests in cases of severe pneumonia. Additionally, they recommend obtaining sputum and blood cultures for inpatients empirically treated for MRSA or Pseudomonas aeruginosa [5]. However, this recommendation is based on low quality of evidence. For this reason and with the aim of enabling targeted therapies, the guidelines encourage new research to find rapid, cost-effective, sensitive, and specific diagnostic tests that identify the causative microorganism.
In recent years, molecular tests have become available for multiple pathogen detection. They are the preferred method for diagnosing some pathogens, such as viruses and Mycoplasma pneumoniae [14]. Molecular tests optimize antibiotic selection and allow for de-escalation and for the reduction of antibiotic and antifungal use in viral pneumonia [15]. These techniques have also proven to shift pneumonia aetiology, with a higher prevalence of viruses and atypical microorganisms [16–18].
This study has two main objectives. The first is to describe the clinical characteristics and aetiology of community-acquired pneumonia during the COVID-19 pandemic. The second is to assess the diagnostic effectivity of the microbiological tests, including a molecular test of respiratory pathogens (FilmArray™ bioMérieux) performed as a nasal swab.
2. Methods
This study has a prospective design: all patients admitted for community-acquired pneumonia (except COVID-19 cases) collected from the 1st of February 2021 until the 31st of March 2022. The protocol for respiratory infections in our hospital includes the following: blood cultures, sputum cultures (when possible), Legionella and Pneumococcal urinary antigen testing, and viral nasal swab (Allplex Respiratory Panel Assays PCR) in all patients. Allplex Respiratory Panel Assays PCR includes testing for FluA, FluA-H1, FluA-H1pdm09, FluA-H3, FluB, RSV-A, RSV-B; AdV, HEV, MPV, PIV-1, PIV-2, PIV-3, PIV-4, HBoV, human coronavirus 229E, NL63, OC43, and HRV. In the cases for which all tests were negative, we added our novel test: the respiratory pathogens FilmArray. This test includes identification for coronavirus 229E, coronavirus HKU1, coronavirus OC43, coronavirus NL63, metapneumovirus, rinovirus/enterovirus, influenza A, influenza A/H1, influenza A/H1-2009, influenza A/H3, influenza B, parainfluenza 1, parainfluenza 2, parainfluenza 3, parainfluenza 4, VRS, Bordetella pertussis, Chlamydophila pneumoniae, and Mycoplasma pneumoniae. Figure 1 represents the protocol that was followed.
According to clinical criteria, other microbiological tests were performed: Mycoplasma pneumoniae, Chlamydophila pneumoniae, Coxiella burnetti, Chlamydophila psittaci serological tests, bronchoalveolar lavage or aspirate, and culture of pleural effusion. Immunofluorescence is used for C. psittaci (IgM and IgG) and C. burnetti (IgM, IgG, and phases) while M. pneumoniae (IgM e IgG) are analysed by automated CLIA technique. For the serological tests, a confirmed diagnosis needed to meet the following criteria: (a) 2 serological tests 2–4 weeks apart confirming a 4-time elevation of IgG titers or (b) 2 serological tests 2–4 weeks apart with seroconversion (the first with positive IgM and negative IgG and the second with positive IgG). A possible diagnosis is given when the following criteria were met: (a) only 1 serological result available with a positive IgM and a negative IgG or (b) elevated IgG titles suggesting acute infection (ie IgG >1/1024 for Chlamydophila pneumoniae). Patients included in the study signed an informed consent form.
Data collection included age, sex, comorbidities, NEWS2 score at admission, infection markers in blood tests, microbiological tests performed, and clinical evolution during admission (ICU admission, death, and discharge). Categorical variables were expressed as numbers and percentages, and continuous variables as mean and standard deviation (SD) or median and percentiles p25 and p75 if a nonnormal distribution was found. Proportions for categorical variables were compared using the χ^2^ test. The independent group Mann–Whitney U test was used for the comparison of continuous variables. All statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) version 22.0 software (SPSS Inc.). Two-sided p values of less than 0.05 were considered statistically significant.
3. Results
In total, 225 patients were included in the study. Patients admitted for COVID-19 pneumonia (a total of 1072 during the study period) were excluded. Epidemiological data and comorbidities are presented in Table 1.
The median NEWS2 score on arrival at the emergency room was 4 points [2–6.5]. The blood test showed median leukocytes of 13,4000 [9,200–17,000] with C reactive protein values of 10.8 mg/dl [4.3–22.4] and procalcitonin of 0.4 ng/dl [0.1–1.6]. A wide majority of patients (168, 74.67%) had lobar pneumonia. However, 41 (18.22%) had a radiologically bilobar pneumonia, and 13 (5.78%) had a multilobar condensation or infiltrate.
Concerning the results of diagnostic tests: urinary antigen testing was performed in 180 of the patients (80%) and was positive in 20 (11.1%); 15 of the positives were for S. pneumoniae and the rest for L. pneumophila. Blood cultures were obtained in 191 patients (84.89%), and 13 (6.8%) were positive. Viral PCR was conducted in 152 patients (67.56%) and was positive in 23 instances (15.1%). Sputum cultures were obtained in 70 patients (31.11%), and 21 of them were positive (30%). Serological tests for atypical pneumonia were performed in 89 patients and were positive in 35 cases, but only 3 met the criteria for a confirmed diagnosis due to the absence of a second serological test. The FilmArray PCR was performed in 43 patients with 3 positive results. Pleural effusion analysis and culture were performed in 8 patients (3.56%) and yielded 2 (25%) positive results. Bronchial aspirate (BAS) or bronchoalveolar lavage (BAL) was obtained for 22 (9.78%) of the patients, and 9 were positive (40.91%).
Despite the above-described testing, no causal agent was identified in most patients (157, 69.77%). Of the patients for whom an aetiological diagnosis could be obtained, Streptococcus pneumoniae was the most common isolate [19] followed by Pseudomonas aeruginosa [7]. Aspiration pneumonia was suspected in 44 patients (19.56%) by the clinician (Table 2).
Concerning patient outcomes, 14 (6.2%) were admitted to the ICU, 11 of which required endotracheal intubation. 7 patients required high-flow nasal oxygen cannula at some point. The median admission time was 7 days [5–12], and the median antibiotic course was 9 days [7–12]. Mortality during admission was 12.4%.
We studied the differences between patients with pneumonia of known versus unknown aetiology. In the unknown aetiology group, there were more cases of bronchoaspiration, shorter antibiotic courses, a lower rate of ICU admissions, and shorter hospital admissions (Table 3).
We also searched for differences between patients who died during admission and those who did not. The patients who died during admission had a higher NEWS2 score, were older, had a higher Charlson score, had a higher prevalence of active oncohematological disease and chronic neurological disease, and had a higher rate of bronchoaspiration, a longer antibiotic course, and a greater need of high flow oxygen cannula (Table 4).
4. Discussion
Our study revealed several important findings. First, we observed a low rate of microorganism identification in our patient cohort despite our extensive diagnostic protocol (including FilmArray for respiratory pathogens). Failure in microorganism identification occurred in approximately 70% of patients. This finding is consistent with previous studies in the existing literature [3, 4]. Notably, we found that cases with unknown aetiology were more common in patients with shorter hospital admissions, which likely limited the ability to conduct comprehensive diagnostic tests.
Similar to the findings in other studies in North America, Europe, and Australia [19, 20], Streptococcus pneumoniae was the most frequently identified pathogen in our series. The second most frequent microorganism was Pseudomonas aeruginosa, typically associated with nosocomial pneumonia. The proportion of Pseudomonas aeruginosa cases identified was similar to that reported in other studies [21]. Klebsiella pneumoniae, E. coli, and other GNB, frequently isolated in patients with pneumonia in tropical areas, notably in Southeast Asian countries, are found in a small proportion of patients in our series and in other Western world series [22, 23].
Remarkably, there were very few cases of viral pneumonia during the study period, excluding those caused by COVID-19. The total number of viral pneumoniae amounted to only 5 cases, including 3 cases of metapneumovirus and 2 cases of respiratory syncytial virus. No instances of influenza-related pneumonia were observed during the study period, which was consistent with the flat curve of influenza incidence in the Balearic Islands [24]. We hypothesize that the widespread use of masks, adherence to social distancing measures, and a higher rate of influenza vaccination likely contributed to the reduction in viral pneumonia cases. In a prior study with a higher positive rate in aetiology, viral pneumonia was identified as a significant cause [25]. However, in our current series, the prevalence of viral pneumonia was notably low, attributed to the unique epidemiologic situation during the COVID-19 pandemic. This fact has probably contributed to a lower diagnosis in our study.
We found no significant association between microorganism identification and mortality. On the contrary, patients with an unknown aetiology had shorter courses of antibiotic treatment and hospital stays. This may suggest a greater ease in identifying the causative microorganism in more severe forms of the disease for reasons yet to be determined. Therefore, the possibility of isolating the causative microorganism could be used as a marker of disease severity, as noted in other studies [26].
In our study, bronchoalveolar aspirate or lavage was identified as the test with the highest predictive positive value (40%), especially in patients with severe pneumonia. It is also noteworthy that patients with shorter stays did not undergo serological testing, which may have limited the breadth of diagnostic possibilities. Consequently, patients with prolonged hospital stays and more severe pneumonia were subjected to a more extensive battery of tests, thereby increasing the likelihood of obtaining a comprehensive aetiological diagnosis.
In a previous study, patients with unknown aetiology had worse outcomes [25]. However, this is most likely because most patients died before 48 hours of admission due to delayed or lack of ICU care therefore limiting the possibility of an ethology work-up.
Our study aimed to assess the performance of diagnostic tests, with sputum analysis and viral PCR emerging as the most useful ones. However, sputum analysis has limitations as it requires patient cooperation, leading to its successful processing in only 31% of cases. Moreover, most sputum samples were collected postantibiotic initiation due to challenges in obtaining them upon admission to the emergency room. On the other hand, viral PCR yielded positive results in 23 patients, primarily contributing to the identification of coinfections (Rhinovirus, Adenovirus, or Enterovirus). They were the primary cause of pneumonia in only 5 cases.
We also evaluated the performance of a molecular test for respiratory pathogens (FilmArray™ bioMérieux) conducted using a nasal swab. However, this test exhibited a low positivity rate of 7% among the tested patients and mainly aided in the diagnosis of coinfections (1 case of diagnostic respiratory syncytial virus and 2 cases of coinfection with rhinovirus/adenovirus). Nevertheless, further investigation is warranted to explore the potential of these novel techniques, as other studies have proven their ability to improve diagnosis and treatment outcomes [27]. There is improvement in the diagnosis rates in lower respiratory tract samples, but the beneficial effect on nasopharyngeal samples is uncertain due to possible contamination [28–31].
Our study had some limitations. Not all tests were performed on every patient, especially the molecular test for respiratory pathogens. In most cases, only one serological test was performed instead of two, which potentially might have underestimated the diagnosis of atypical pneumoniae. Additionally, we were unable to establish a correlation between the identification of aetiology and improved prognosis in community-acquired pneumonia, possibly due to sample size constraints.
In conclusion, we have observed a reduction in influenza and other viral pneumoniae during the COVID-19 pandemic. Despite our extensive diagnostic protocol, there is still a low rate of microorganism identification. Having a high NEWS2 score on arrival at the emergency department, an active oncohematological disease or chronic neurological conditions and a positive microbiological test result should serve as an alarm for clinicians, prompting them to provide enhanced attention to the patient. Furthermore, further research is needed to determine the role of molecular tests in the microbiological diagnosis of pneumonia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Falguera M. Ramírez M. F. Community-acquired pneumonia Revista Clínica Española 2015215845846710.1016/j.rceng.2015.08.00326186969 · doi ↗ · pubmed ↗
- 2Marshall D. C. Goodson R. J. Xu Y. Trends in mortality from pneumonia in the Europe union: a temporal analysis of the European detailed mortality database between 2001 and 2014 Respiratory Research 2018191 p. 8110.1186/s 12931-018-0781-42-s 2.0-85046420246 PMC 593599829728122 · doi ↗ · pubmed ↗
- 3Rothberg M. B. Community-acquired pneumonia Annals of Internal Medicine 20221754 ITC 496410.7326/aitc 20220419035404672 · doi ↗ · pubmed ↗
- 4Remington L. T. Sligl W. I. Community-acquired pneumonia Current Opinion in Pulmonary Medicine 201420321522410.1097/mcp.00000000000000522-s 2.0-8489757880724614242 · doi ↗ · pubmed ↗
- 5Metlay J. P. Waterer G. W. Long A. C. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American thoracic society and infectious diseases society of America American Journal of Respiratory and Critical Care Medicine 20192007 e 45e 6710.1164/rccm.201908-1581 st 2-s 2.0-8507277466931573350 PMC 6812437 · doi ↗ · pubmed ↗
- 6Engel M. F. van Manen L. Hoepelman A. I. M. Thijsen S. Oosterheert J. J. Diagnostic, therapeutic and economic consequences of a positive urinary antigen test for Legionella spp. in patients admitted with community-acquired pneumonia: a 7-year retrospective evaluation Journal of Clinical Pathology 201366979780210.1136/jclinpath-2012-2012092-s 2.0-8488285161623775436 · doi ↗ · pubmed ↗
- 7Uematsu H. Hashimoto H. Iwamoto T. Horiguchi H. Yasunaga H. Impact of guideline-concordant microbiological testing on outcomes of pneumonia International Journal for Quality in Health Care 201426110010710.1093/intqhc/mzt 0782-s 2.0-8489357591624257160 · doi ↗ · pubmed ↗
- 8Costantini E. Allara E. Patrucco F. Faggiano F. Hamid F. Balbo P. E. Adherence to guidelines for hospitalized community-acquired pneumonia over time and its impact on health outcomes and mortality Internal and Emergency Medicine 201611792994010.1007/s 11739-016-1445-32-s 2.0-8496434553927098057 · doi ↗ · pubmed ↗