Habitat-based radiomics analysis for evaluating immediate response in colorectal cancer lung metastases treated by radiofrequency ablation
Haozhe Huang, Hong Chen, Dezhong Zheng, Chao Chen, Ying Wang, Lichao Xu, Yaohui Wang, Xinhong He, Yuanyuan Yang, Wentao Li

TL;DR
This study develops a radiomics signature based on tumor habitats to predict treatment response in colorectal cancer lung metastases after radiofrequency ablation.
Contribution
A novel habitat-based radiomics signature is proposed, combining spatial tumor features to improve prediction accuracy.
Findings
The Habitat+Peri-5 signature achieved an AUC of 0.870 in the test set, outperforming clinical and intratumor models.
Combining habitat and peritumor radiomics features improved calibration and clinical utility for predicting treatment response.
80% of metastases achieved complete response after radiofrequency ablation.
Abstract
To create radiomics signatures based on habitat to assess the instant response in lung metastases of colorectal cancer (CRC) after radiofrequency ablation (RFA). Between August 2016 and June 2019, we retrospectively included 515 lung metastases in 233 CRC patients who received RFA (412 in the training group and 103 in the test group). Multivariable analysis was performed to identify independent risk factors for developing the clinical model. Tumor and ablation regions of interest (ROI) were split into three spatial habitats through K-means clustering and dilated with 5 mm and 10 mm thicknesses. Radiomics signatures of intratumor, peritumor, and habitat were developed using the features extracted from intraoperative CT data. The performance of these signatures was primarily evaluated using the area under the receiver operating characteristics curve (AUC) via the DeLong test, calibration…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
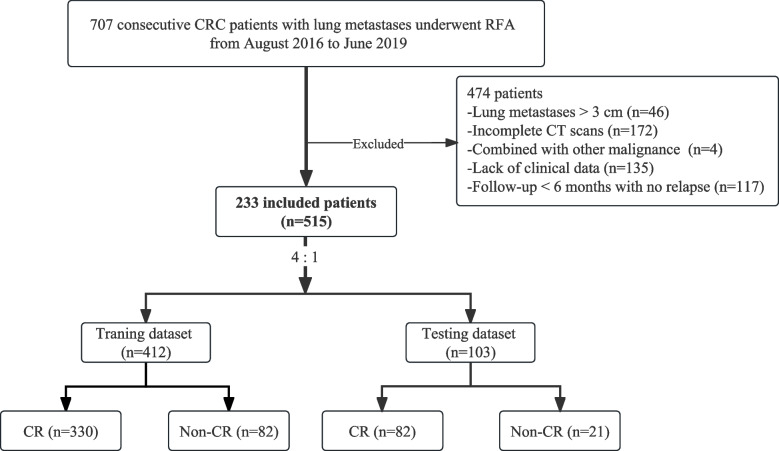 Figure 1
Figure 1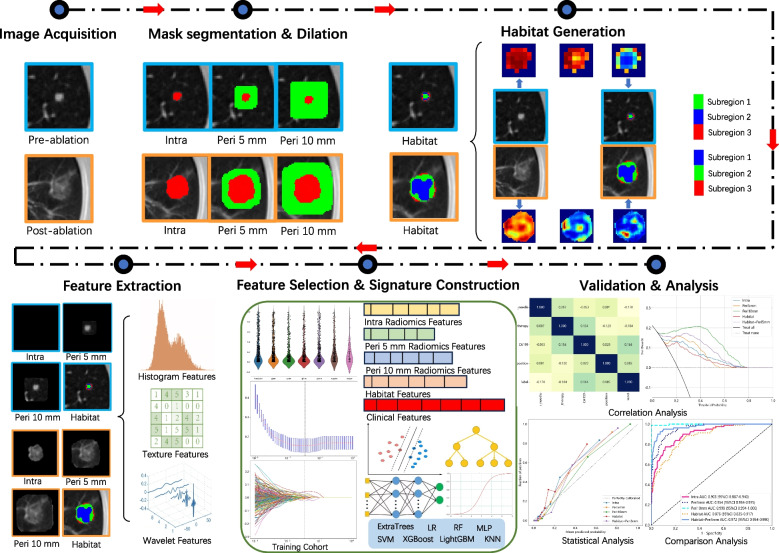 Figure 2
Figure 2 Figure 3
Figure 3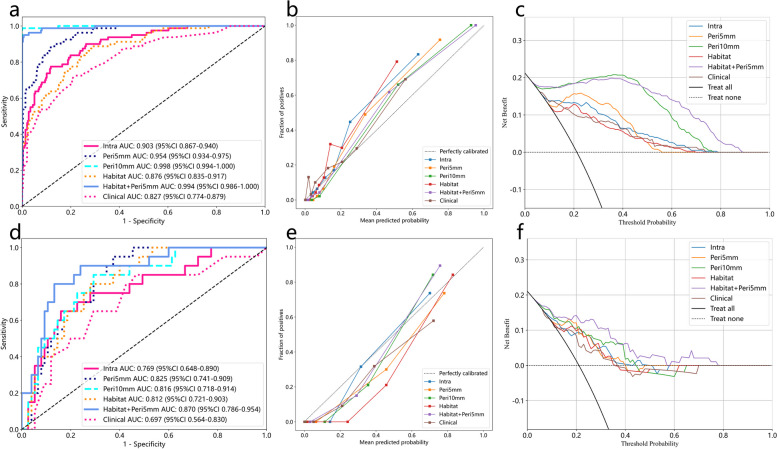 Figure 4
Figure 4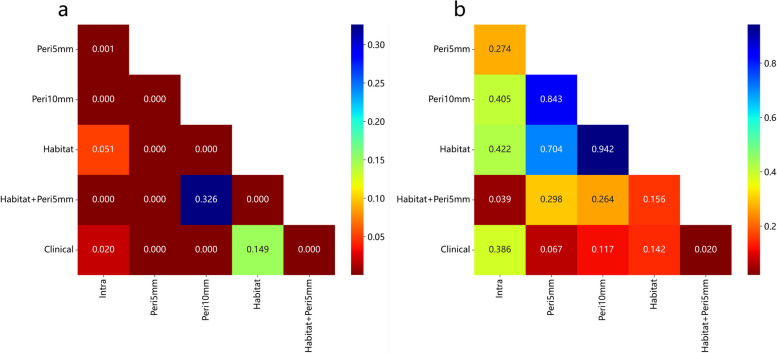 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEducational Technology in Learning · E-Learning and Knowledge Management · Educational theories and practices
Introduction
The lung ranks as the second most frequent location for metastases from colorectal cancer (CRC) [1]. Despite the importance of surgery, published reports indicate varying 5-year survival rates of 24 to 56% following surgical removal of CRC lung metastases [2]. European Society for Medical Oncology (ESMO) guidelines for metastatic CRC suggest considering local ablation alongside resection, based on factors like tumor size, number, location, lung tissue loss, comorbidity, and other relevant considerations [3].
Computed tomography (CT)-guided percutaneous radiofrequency ablation (RFA) stands as a viable choice for treating small lung metastases, especially those under 3 cm [4, 5]. However, due to the lack of histological evidence confirming complete ablation and a reported recurrence rate of 32.6% [6], assessing ablation outcomes after RFA remains challenging. The usual assessment of ground-glass opacity (GGO) [7], linked to residual tumor and recurrence [8], can be impacted by intraoperative intra-alveolar hemorrhage (IAH) or atelectasis [4, 9, 10]. The initial 3-month inflammatory response around the ablated lesion complicates early efficacy evaluation [11]. Hence, there’s a need to objectively define and evaluate the immediate ablation outcomes for CRC lung metastases.
In the context of personalized and precise treatments, radiomics can extract high-dimensional quantitative features from medical images. These features encompass data about tumor heterogeneity and the microenvironment [12, 13], enabling a more accurate assessment of traits and treatment response [14, 15]. Peritumoral features have been proposed to enhance radiomic models’ predictive abilities [16–19]. Unlike previous methods, a novel approach divides tumors into subregions known as habitats, containing voxels with similar attributes and consistent tumor biology [20]. This approach improved intratumoral heterogeneity quantification [21, 22].
To the best of our knowledge, no studies have aimed to develop habitat-based radiomics analysis to predict early RFA efficacy in CRC lung metastases. In this study, we employed a new radiomics approach to identify imaging biomarkers within intratumoral, peritumoral, and sub-regional zones. This enables assessing the immediate response to RFA in CRC lung metastases.
Methods
Patient selection and clinicopathological information
Due to the retrospective nature of this study, patient informed consent was waived. We included 233 consecutive CRC patients with lung metastases who underwent initial RFA between August 2016 and June 2019. Inclusion criteria were: (1) confirmed CRC through histology; (2) lung metastases treated with RFA, ≤ 3 cm in maximum diameter; (3) comprehensive medical records with clinical variables and CT data from procedure and follow-up; (4) technically successful ablation; (5) adequate normal organ function. Exclusion criteria were: (1) receiving other local treatments like radiotherapy or re-ablation; (2) inability to tolerate RFA; (3) concurrent malignant tumors or extrapulmonary metastasis. Patients with multiple nodules were included, analyzing each nodule individually [10, 23, 24]. A cohort of 515 lung metastases in 233 CRC patients who underwent RFA was enrolled and randomly divided into training and test cohorts at a 4:1 ratio (Fig. 1). Supplementary data 1 provided detailed RFA equipment and procedure information.Fig. 1. Flow diagram of the enrolment patients
The clinical variables including age, gender, serum tumor markers (carcinoembryonic antigen (CEA) and cancer antigen 19–9 (CA19–9)), lymphadenopathy at diagnosis, concomitant systemic treatment, and primary tumor location were collected within 1 week before RFA. Radiological data from intraoperative CT scans included pulmonary metastases size, location, proximity to vital structures like the heart or major blood vessels (> 3 mm in diameter), distance to the pleura or diaphragm (within 1 cm), electrode type, and complications such as IAH or pneumothorax.
CT examination protocol and local efficacy assessment
Pre- and immediate post-ablation CT scans were conducted using the United Imaging uCT 760 (United Imaging Medical Technology Inc.) and Philips Brilliance 64 slice (Philips Medical Systems Inc.) machines. Settings were: 200 mA, 120 kVp, 0.5 s/round, with 1 mm or 1.5 mm section thickness. The images were reconstructed using iterative reconstruction, and the resulting CT data was stored in the. DICOM format.
A contrast-enhanced chest CT was conducted as the baseline 1 month after ablation [25], followed by additional scans every 2 to 3 months. The treatment’s local efficacy was assessed by two experienced radiologists who were unaware of clinical data. Evaluation was grounded in chest-enhanced CT scans performed at least 6 months after RFA, adhering to the modified response evaluation criteria in solid tumors (mRECIST) criteria [11, 26]. Should there be differences in interpretation between the radiologists, consultation with a senior expert boasting over 20 years of experience was pursued. Complete response (CR) was determined by the presence of cavity, fibrosis, or nodule without enhancement. In contrast, the presence of irregular nodular, scattered, or eccentric patterns of peripheral enhancement within 1 cm of the ablation area in two consecutive CT scans denoted a non-complete response (non-CR).
Workflow of radiomics analysis
The radiomics analysis was executed through a series of steps: image segmentation, feature extraction, feature selection, signature construction, and evaluation (Fig. 2).Fig. 2. Workflow of radiomics analysis
Advanced image processing and mask segmentation
To enhance the robustness of medical image analysis, preprocessing techniques were applied. The CT images were uniformed to a common resolution of 1 mm × 1 mm × 1 mm by the B-spline interpolation algorithm, and then the window width was adjusted within the range of - 1200 Hu to 600 Hu and the intensity was scaled within the range of 0 ~ 255.
Recently, numerous studies have demonstrated that the improved methods based on U-Net performed well in the segmentation of pulmonary nodules, which were trained on the Image Database Resource Initiative (IDRI) created by the US Institutes of Health based on the Lung Image Database Consortium (LIDC) [27–31]. We also have trained a 3D UNet model based on the open-source dataset to segment the target lesions and immediate ablation regions from pre- and postoperative CT images, with a Dice coefficient of 83.04% [32]. These masks were subsequently verified by two junior radiologists (HZH and HC, 8 years of specialized chest imaging) and the necessary adjustments have been made to guarantee accuracy and repeatability using the ITK-SNAP (version 3.8.0, http://www.itksnap.org). If they had disagreements, it would be determined in consultation with the senior expert (WTL, 30 years of specialized chest imaging).
Peritumoral region dilation
The regions of interest (ROI) were expanded using the mask padding toolkit provided by the Onekey AI platform. We evaluated the impact of different peritumoral sizes on model predictability by applying dilation intervals of 5 mm. Any ROIs extending beyond the lungs or overlapping with the heart, major blood vessels, or diaphragm were manually adjusted.
Habitat generation
Local features, including local entropy and energy values, were extracted from each voxel within VOI. These feature vectors represented diverse aspects of voxel properties. A 77-dimensional feature vector (Supplementary data 2) was generated for each block using a 3 × 3 × 3 non-overlapping moving window. The Calinski-Harabasz (CH) value selection method [33] was used to determine the optimal number of clusters. Subsequently, the K-means method was employed to cluster sub-regions for each sample.
Feature extraction and selection
Handcrafted features extracted using the Pyradiomics tool (version 3.0.1) were categorized into three groups: geometry, intensity, and texture (Supplementary data 2), following the guidelines of the imaging biomarker standardization initiative (IBSI). Unsupervised clustering yielded varying physical meanings for the habitat extracted from the subregions with identical centers. To mitigate this, mean feature values were computed.
Robustness was assessed through test-retest and inter-rater analyses, with the intraclass correlation coefficient (ICC) set at a threshold of ≥0.85. Nonetheless, ICC was not suitable for assessing the unsupervised habitat signature. All features were standardized using Z-scores to maintain a normal distribution, followed by a t-test to retain radiomic features with p-value < 0.05. Pearson’s correlation coefficient was computed to pinpoint highly consistent features with a coefficient > 0.9. The greedy recursive deletion strategy was then employed to filter out the highly redundant features. To curb overfitting, the minimum redundancy maximum relevance (mRMR) algorithm selected the top 8 features for each modality. The final features set was determined using the least absolute shrinkage and selection operator (LASSO) regression. LASSO adjusted parameter λ to assign zero regression coefficients to irrelevant features. Optimal λ value selection involved 10-fold cross-validation with minimum criteria, aiming for the lowest mean square error (MSE).
Signature construction
Several radiomics signatures were formulated based on distinct regions: intratumor and ablated area (Intra), intratumor with expanded tumor and ablated regions (5 mm and 10 mm, Peri-X), intratumor and ablated area subregions (Habitat), and intratumor combined with peritumoral regions. Additionally, the optimal peritumoral region was integrated with the tumor microenvironment habitat, termed Habitat + Peri-X. The Clinical signature was created from independent risk factors identified via multivariate logistic analysis. Commonly used machine learning models, including logistic regression (LR), support vector machine (SVM), K-nearest neighbor (KNN), random forest (RF), extremely randomized trees (ExtRa Trees), eXtreme gradient boosting (XGBoost), light gradient boosting machine (LightGBM), and multi-layer perceptron (MLP), were employed for model construction. Optimal hyperparameters for each model were determined using five-fold cross-validation and the Grid-search algorithm.
Performance evaluation
The performance of various signatures was verified using an independent test dataset, generating receiver operating characteristic (ROC) curves to calculate the corresponding area under the curve (AUC). The Delong test was used to compare predictive performance differences among the models [34]. Additionally, accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were computed. The Youden index determined the optimal cut-off value maximizing the sum of sensitivity and specificity [35]. Calibration curves were plotted to assess calibration accuracy, alongside the Hosmer-Lemeshow (HL) test [36] (A significant test statistic implies that the model does not calibrate perfectly.). Moreover, decision curve analysis (DCA) gauged the clinical utility of predictive signatures [37].
Statistical analysis
Statistical analyses were performed using IBM SPSS (version 26.0). Continuous variables were presented as mean ± standard deviation (SD) and compared using the Man-Whitney U test. Categorical variables were expressed as counts with percentages and compared using the Chi-square or Fisher test. Variables with a P-value < 0.05 in univariate regression analysis were included in multivariable analysis. Variables with a P-value < 0.05 in multivariable analysis were considered independent predictors linked to immediate response. All statistical tests were two-sided with a significance level set at P < 0.05.
Results
Baseline characteristics
The training dataset consisted of 412 lesions (330 CR and 82 non-CR) selected via random division, while 103 lesions (82 CR and 21 non-CR) contributed the independent test dataset (Table 1). Table 1. Characteristics of patients and CRC lung metastasesCharacteristicsTraining datasetTest datasetP value(N_1_ vs N_2_)N_1_ = 412CR = 330Non-CR = 82N_2_ = 103CR = 82Non-CR = 21Age (years)^#^57.91 ± 10.4257.74 ± 10.3758.41 ± 10.6957.48 ± 10.8958.67 ± 10.8152.80 ± 9.850.59Gender0.68Male23418450614813Female1781463242348Tumor markersCEA (ng/ml)^#^14.89 ± 44.1212.48 ± 37.9127.13 ± 65.9213.49 ± 20.8011.50 ± 16.8020.84 ± 30.890.71CA19–9 (U/ml)^#^29.73 ± 56.7825.41 ± 48.3251.75 ± 88.3820.67 ± 30.6918.91 ± 29.8627.01 ± 32.950.29Lymphadenopathy at diagnosis0.03Yes28221864615011No13011218423210Concomitant systemic treatment0.10Yes27623145594712No136993744359Initial tumor location0.60Rectum27421658765719Sigmoid—left colon5850811101Transverse—right colon75601514131Caecum541220Nodule size (mm)^#^1.21 ± 0.661.12 ± 0.381.35 ± 0.421.27 ± 0.671.20 ± 0.481.38 ± 0.710.31Lung metastases location0.22RUL98871123194RML3932718162RLL7857211688LUL94791522193LLL103752824204Distance 10.28> 1 cm34027763796217< 1 cm72531924204Distance 20.08> 1 cm16113130493910< 1 cm25119952544311Electrode type1.00Expandable38031070947618Straight322012963Pneumothorax1.00Yes115932228226No29723760756015IAH0.01Yes108931540346No30423767634815CRC colorectal cancer, CEA carcinoembryonic antigen, CA19–9 cancer antigen 19–9, CR complete response, RUL right upper lobe, RML right middle lobe, RLL right lower lobe, LUL left upper lobe, LLL left lower lobe, Distance 1 the distance between the lesion and the great vessels or mediastinum, Distance 2 the distance between the lesion and the pleura or diaphragm, IAH intra-alveolar hemorrhage^#^ Mean ± SD
Establishment of clinical models
Univariate logistic regression analysis (Table 2) revealed significant factors for identifying ablated lesions: CEA, CA19–9, concomitant systemic treatment, lung metastases location, and electrode type (P < 0.05). Multivariate regression analysis indicated that CA19–9 (odds ratio [OR] = 1.002, P < 0.001), concomitant systemic treatment (OR = 0.916, P = 0.042), lung metastases location (OR = 1.032, P = 0.019), and electrode type (OR = 0.778, P = 0.004) were independent factors influencing ablation effect, forming the basis for clinical models construction. Table 2. Uni- and multivariate analysis of clinical and radiological characteristicsCharacteristicsUnivariate analysisMultivariate analysisOR (95%CI)P valueOR (95%CI)P valueAge1.001(0.998–1.004)0.628Gender1.047(0.975–1.123)0.285CEA1.001(1.001–1.002)0.0051.001(1.0–1.001)0.131CA 19–91.002(1.001–1.002)< 0.0011.002(1.001–1.002)**< 0.001#**Lymphadenopathy at diagnosis1.091(1.013–1.175)0.052Concomitant systemic treatment0.895(0.832–0.964)0.0130.916(0.853–0.983)**0.042#**Initial tumor location0.982(0.941–1.026)0.500Nodule size0.956(0.608–1.307)0.642Lung metastases location1.033(1.010–1.015)0.0201.032(1.009–1.005)**0.019#**Distance 11.092(0.995–1.198)0.119Distance 21.006(0.935–1.081)0.897Electrode type0.753(0.652–0.869)0.0010.778(0.675–0.897)**0.004#**Pneumothorax1.012(0.934–1.096)0.808IAH0.933(0.860–1.013)0.165OR odds ratio, 95%CI 95% confidence interval, CEA carcinoembryonic antigen, CA19–9 cancer antigen 19–9, Distance 1 the distance between the lesion and great vessels or mediastinum, Distance 2 the distance between the lesion and pleura or diaphragm, IAH intra-alveolar hemorrhage. The bold p values in the univariate (*) and multivariate analysis (#) mean < 0.05
Sub-region cluster and feature selection
Optimal CH value emerged when tumors were clustered into three sub-regions in the entire cohort (Fig. 3). To enhance the feature set, features from both pre- and post-ablation images were fused, resulting in 3668 features. Features were extracted via Pyradiomics (http://pyradiomics.readthedocs.io).Fig. 3. Calinski–Harabasz score plot. The red dotted line represented the optimal value beyond which the scores started to decrease in the radiomics features from CT images before (black line) and after (green line) ablation
Radiomics features with non-zero coefficients were selected using the LASSO method with the best lambda (Supplementary data 3). For habitat-based radiomics signature, lambda of 0.0095 yielded the best, selecting 71 features. These comprised 20 habitat features (8 pre- and 12 post-RFA) and 51 peritumoral features (29 pre- and 22 post-RFA).
Performance and comparison of signatures
Based on the analysis of prediction performance (Supplementary data 3), the Intra radiomics signature employed RF, the Peri-X radiomics signature utilized LightGBM, the Habitat radiomics signature was developed using ExtRa Trees, while the Habitat+Peri-5 radiomics and clinical signatures were constructed with XGBoost.
Summary of predictive performance for clinical and radiomics signatures was presented in Table 3 and Fig. 4. The clinical signature achieved AUC values of 0.827 (training) and 0.697 (test), hinting at potentially limited generalizability to unseen data. The Peri-5 signature outperformed Peri-10 in test AUC, prompting its combination with the Habitat signature. The Habitat+Peri-5 signature excelled in both training (AUC 0.972) and test (AUC 0.846) sets (Fig. 4 a and d). Moreover, calibration curves of the Habitat + Peri-5 signature exhibited robust concurrence between observed and projected probabilities (Fig. 4 b and e). The HL test yielded insignificant deviations (training cohort: P = 0.212; test cohort: P = 0.283), signifying conformity. DCA portrayed the enhanced clinical benefit of the fusion signature over other signatures (Fig. 4 c and f). Table 3. Performance comparison of all signaturesSignatureACCAUC95%CISensitivitySpecificityPPVNPVYoudenCohortClinical0.7770.8270.774–0.8790.7130.7950.4830.9110.278TrainingIntra0.8590.9030.867–0.9400.7750.8820.6390.9360.252TrainingPeri-50.8830.9540.934–0.9750.8870.8820.6700.9670.236TrainingPeri-100.9970.9980.995–1.0000.9881.0001.0000.9970.375TrainingHabitat0.7480.8760.835–0.9170.8870.7100.4520.9590.201TrainingHabitat+Peri-50.9840.9940.986–1.0000.9500.9930.9740.9870.366TrainingClinical0.6000.6970.564–0.8300.8500.5410.3270.9300.193TestIntra0.8000.7690.648–0.8900.6500.8510.5200.9000.238TestPeri-50.6950.8250.741–0.9090.9500.6350.4040.9790.189TestPeri-100.7370.8160.718–0.9140.8500.7160.4360.9460.179TestHabitat0.7370.8120.721–0.9030.8000.7300.4320.9310.212Test**Habitat + Peri-50.8530.8700.786–0.9540.8000.8670.6150.9420.274**TestACC accuracy, AUC the area under the curve, 95%CI 95% confidence interval, PPV positive predictive value, NPV negative predictive value. The bold values mean the best performance of the signature integrating habitat and radiomics features of peritumoral 5 mmFig. 4The receiver operating characteristic (ROC) curves, calibration curves, and decision curve analysis (DCA) of all signatures in the training cohort (a, b, c), and test cohort (d, e, f)
Discussion
This study systematically explored the tumor microenvironment through a comprehensive evaluation of intra- and peritumoral regions in pre- and post-ablation CT scans. As a result, we devised predictive signatures for early ablation efficacy in CRC lung metastases treated with RFA, leveraging sub-regional radiomics features. These signatures provided effective tools for tailoring treatment strategies in CRC patients with lung metastases.
Radiomics analysis enables the extraction and characterization of a broad range of information reflecting underlying biological diversity in a cost-effective manner [12]. A radiomics signature, composed of multiple features, serves as a robust prognostic biomarker that could complement clinical data [38]. The overestimation of the completely necrotic region as GGO on CT [39] indicates the need to ablate peritumoral lung parenchyma within 5 to 10 mm for complete ablation [9, 40]. Previous studies have highlighted the utility of combining intra- and peritumoral radiomics features for improved treatment response prediction [16, 19]. These findings underscore the importance of peritumoral features [16–18, 41]. Therefore, our study aimed to explore the predictive performance of peritumoral radiomics features by assessing the impact of peritumoral region sizes. The results demonstrated that the radiomics signature derived from a 5 mm dilated distance outside both the tumor and ablated area yielded the highest prediction performance compared to the intra- and peritumoral 10 mm regions. This signature exhibited high AUC values and low over-fitting, emphasizing the significance of peritumoral features in radiomics and the influence of peritumoral size on prediction performance.
The sub-region cluster analysis conducted in this study highlighted the importance of sub-region analysis in capturing CRC lung metastases’ tumor heterogeneity. By optimizing the number of clusters, we identified three spatially distinct habitats through K-means clustering. These habitats within the ablation area represented various characteristics: the inner region possibly indicated necrotic areas, the middle region potentially signified effusion areas, and the edge region likely represented congested areas. These findings were consistent with the histopathological results, demonstrating an inner-to-outer transition [39]. As anticipated, the habitat signature, derived from radiomics features within these unique subregions, contributed valuable information in assessing early effects after RFA. Furthermore, by combining habitat and peritumoral signatures, we achieved higher AUC values (training cohort: 0.972, test cohort: 0.870). This outcome validated the superiority of the Habitat+Peri-5 signature over the Intra radiomics signature (P = 0.039, Fig. 5).Fig. 5. The results of the DeLong test in the training cohort (a), and test cohort (b)
Furthermore, multivariate regression analyses identified several clinical variables, including CA19–9 levels, lung metastases location, concomitant systemic treatment, and electrode type. Notably, lung metastases location, particularly in the lower lobes, emerged as an independent risk factor, possibly due to the influence of respiratory movements on accurate probe positioning. Conversely, concomitant systemic treatment and the use of expandable electrodes were protective factors against treatment failure, evident from OR values below 1. Importantly, the Habitat + Peri-5 signature demonstrated a significantly improved AUC value (P = 0.020, Fig. 5) compared to the clinical model (training cohort: 0.827, test cohort: 0.697), underscoring enhanced precision and clinical utility, as supported by the HL test and DCA results.
A study by Markich et al. [10] examined clinical, radiological, technical, and radiomics features examined before and after RFA to evaluate local control in 48 CRC patients with 119 lung metastases. However, their reliance on CT scans taken 48 hours post-ablation hindered real-time procedure assessment, delaying timely interventions. To address this limitation, our recent study [42] integrated relative radiomics features from pre- and immediate post-RFA CT scans with clinical and radiological variables from 479 lung metastases in 198 CRC patients. This aimed to establish a novel multimodal data fusion model for evaluating immediate RFA efficacy. Liu et al. [43] explored intratumor density heterogeneity changes following microwave ablation (MWA) of pulmonary tumors, utilizing radiomics-based CT features for prognostic value in predicting treatment response. Additionally, Zhu et al. [44] developed intra- and peritumoral radiomics models based on post-operative CT images to predict early MWA efficacy in malignant lung tumors, validating the predictive ability. However, neither study explored the optimal peritumoral region nor assessed the impact of peritumoral region sizes. Also, the inclusion of primary and metastatic lung tumors in both studies raised concerns about disease heterogeneity.
This study bears several limitations that warrant acknowledgment. Firstly, it was a single-center retrospective study with a limited sample size. Therefore, a more extensive, multi-center prospective study is essential to validate the generalizability of our signature and ascertain its utility in clinical settings. Secondly, the spatially distinct habitats identified through K-means clustering could not be pathologically confirmed due to technical challenges and ethical considerations. However, pursuing such a correlation might entail unnecessary surgeries.
Conclusion
In summary, this study introduces a pioneering signature that combines habitat and peritumoral radiomics to access immediate response and predict outcomes of RFA in CRC patients with lung metastases. The habitat-based radiomics signature holds the potential for advancing precision medicine and shaping treatment strategies.
Supplementary Information
Supplementary material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mitry E Guiu B Cosconea S Jooste V Faivre J Bouvier AM Epidemiology, management and prognosis of colorectal cancer with lung metastases: a 30-year population-based study Gut.2010591383138810.1136/gut.2010.21155720732912 · doi ↗ · pubmed ↗
- 2Pfannschmidt J Dienemann H Hoffmann H Surgical resection of pulmonary metastases from colorectal cancer: a systematic review of published series Ann Thorac Surg.20078432433810.1016/j.athoracsur.2007.02.09317588454 · doi ↗ · pubmed ↗
- 3Cervantes A Adam R RosellóS Arnold D Normanno N Taïeb J Metastatic colorectal cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up Ann oncol: offic j Europ Soc Med Oncol ESMO.202334103210.1016/j.annonc.2022.10.00336307056 · doi ↗ · pubmed ↗
- 4de Baère T Aupérin A Deschamps F Chevallier P Gaubert Y Boige V Radiofrequency ablation is a valid treatment option for lung metastases: experience in 566 patients with 1037 metastases Ann Oncol.20152698799110.1093/annonc/mdv 03725688058 PMC 4405279 · doi ↗ · pubmed ↗
- 5Ibrahim T Tselikas L Yazbeck C Kattan J Systemic versus local therapies for colorectal Cancer pulmonary metastasis: what to choose and when?J Gastrointest Cancer.20164722323110.1007/s 12029-016-9818-427080402 · doi ↗ · pubmed ↗
- 6Hiyoshi Y Miyamoto Y Kiyozumi Y Sawayama H Eto K Nagai YCT-guided percutaneous radiofrequency ablation for lung metastases from colorectal cancer Int J Clin Oncol.20192428829510.1007/s 10147-018-1357-530328530 · doi ↗ · pubmed ↗
- 7Abtin FG, Eradat J, Gutierrez AJ, Lee C, Fishbein MC, Suh RD. Radiofrequency ablation of lung tumors: imaging features of the postablation zone. Radiographics. 2012;32:947–69. 10.1148/rg.324105181.10.1148/rg.324105181 PMC 339388322786987 · doi ↗ · pubmed ↗
- 8de Baère T Palussière J Aupérin A Hakime A Abdel-Rehim M Kind M Midterm local efficacy and survival after radiofrequency ablation of lung tumors with minimum follow-up of 1 year: prospective evaluation Radiol.200624058759610.1148/radiol.240205080716864679 · doi ↗ · pubmed ↗