Recurrent Gastrointestinal Stromal Tumor With Chondroid Differentiation After Imatinib Therapy: An Unusual Case and Literature Review
Patricia Le, FNU Monika, Ahmed Sabri, Joyce Kovar, Nicholas Dietz

TL;DR
This paper reports a rare case of a gastrointestinal stromal tumor with chondroid features after imatinib treatment and compares it with similar cases in the literature.
Contribution
The novelty is the first documented case of recurrent GIST with chondroid differentiation at the primary site after imatinib therapy.
Findings
A 58-year-old patient had recurrent GIST with chondroid differentiation after two rounds of imatinib therapy.
The case highlights the possibility of chondroid differentiation in GIST post-imatinib therapy, which can mimic other malignancies like chondrosarcoma.
A mini-literature review compares this case with others to explore histomorphological and demographic patterns.
Abstract
Gastrointestinal stromal tumor (GIST) is the most common mesenchymal tumor in the gastrointestinal tract and is most commonly seen in the stomach. The standard treatment for patients with advanced GISTs include both surgical resection and imatinib therapy. There have been cases that document the alterations of patients' GIST histomorphology both with primary GIST prior to imatinib therapy and with recurrent GIST after imatinib therapy. However, there has been no documented case of a patient who has recurrent GIST with chondroid differentiation at the primary site after imatinib therapy. In this article, we report an incidental finding of a 58-year-old patient who had two treatments of imatinib therapy prior to surgical resection of her recurrent GIST in her stomach. We also explore through a mini-literature review the various cases of GIST with chondroid differentiation that have been…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
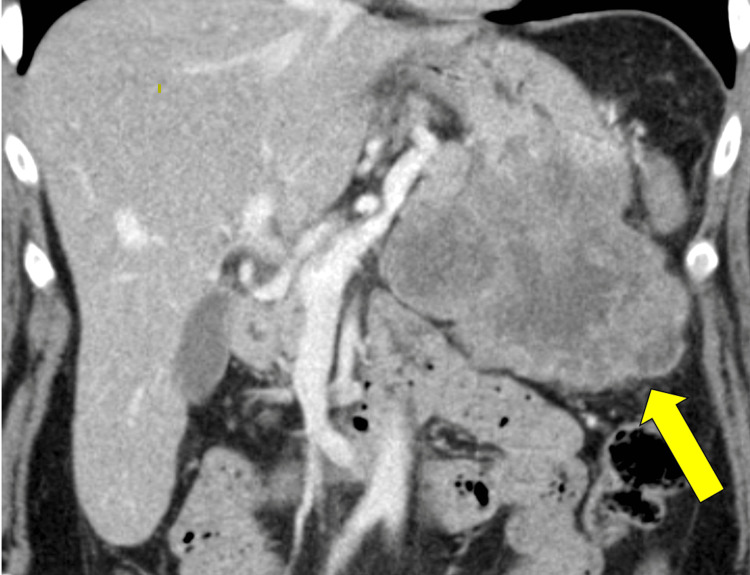 Figure 1
Figure 1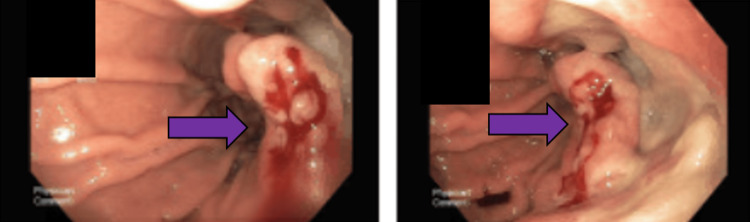 Figure 2
Figure 2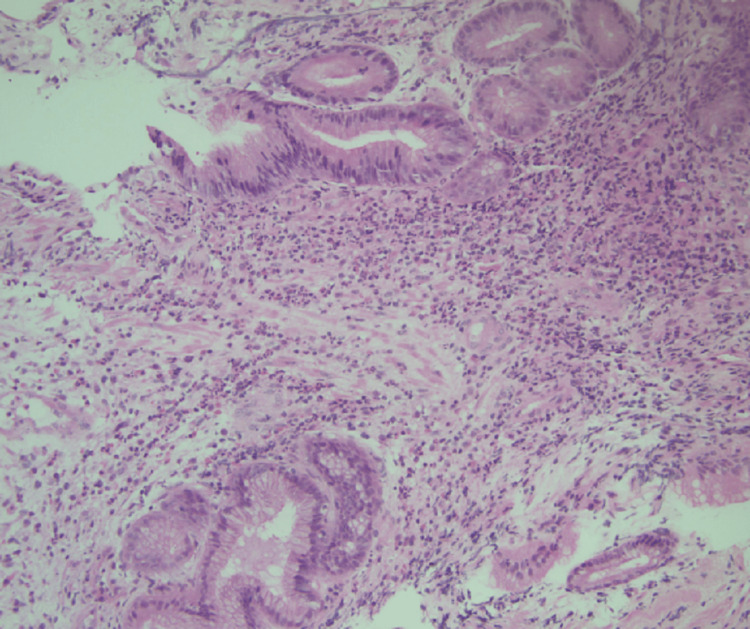 Figure 3
Figure 3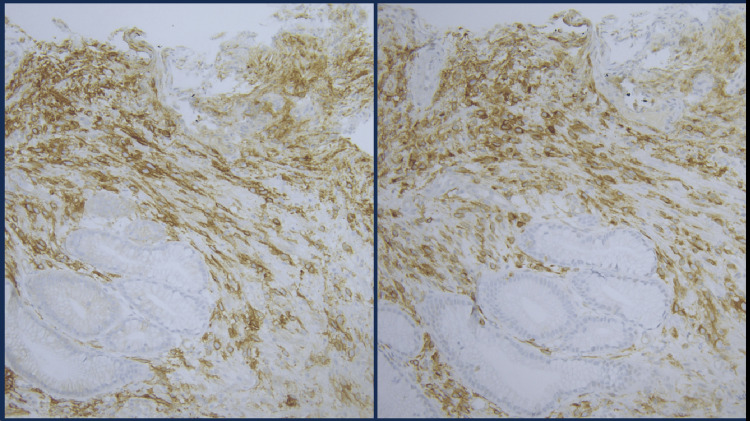 Figure 4
Figure 4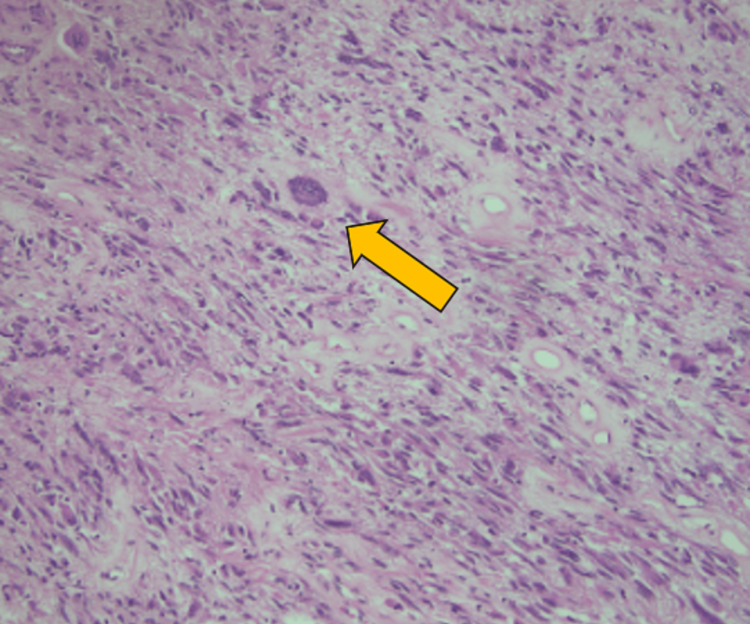 Figure 5
Figure 5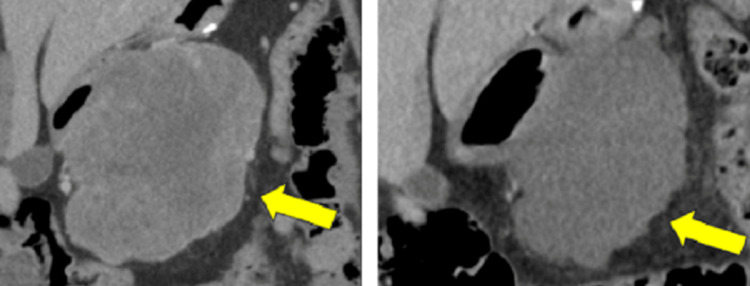 Figure 6
Figure 6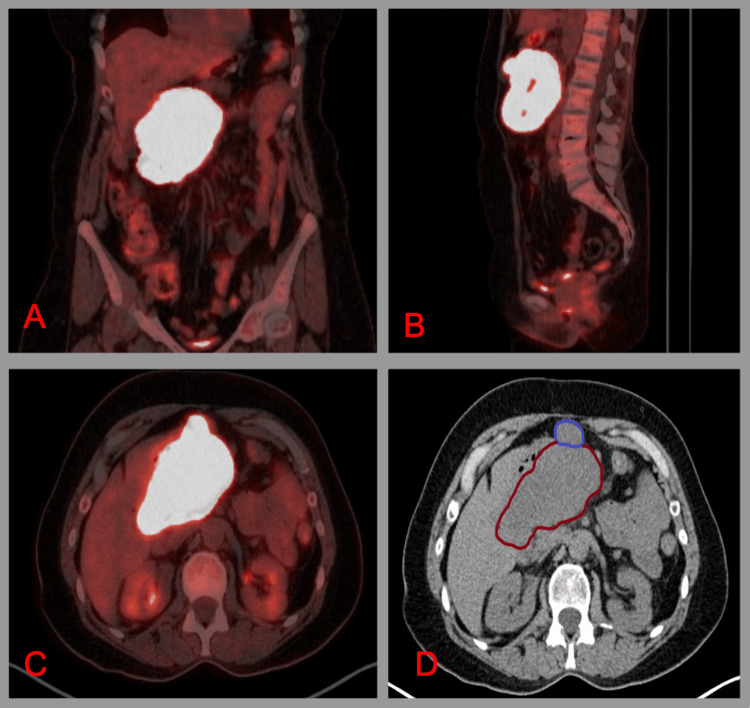 Figure 7
Figure 7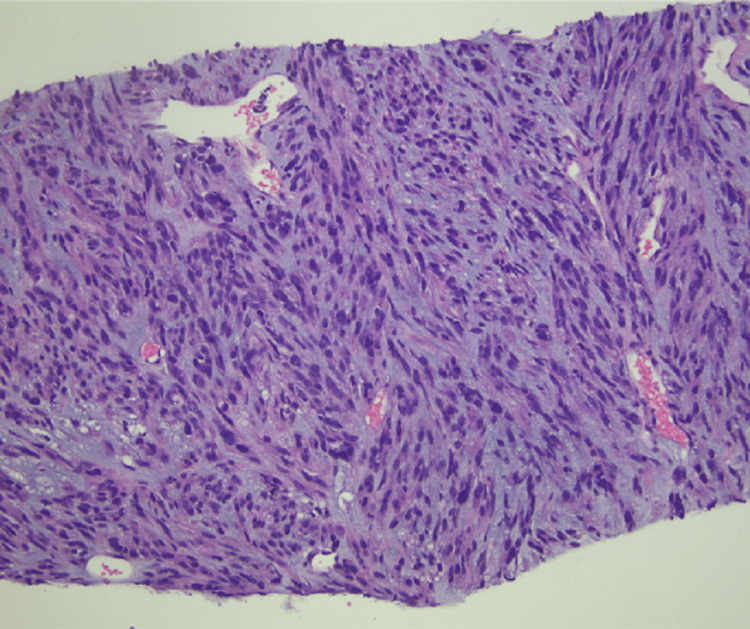 Figure 8
Figure 8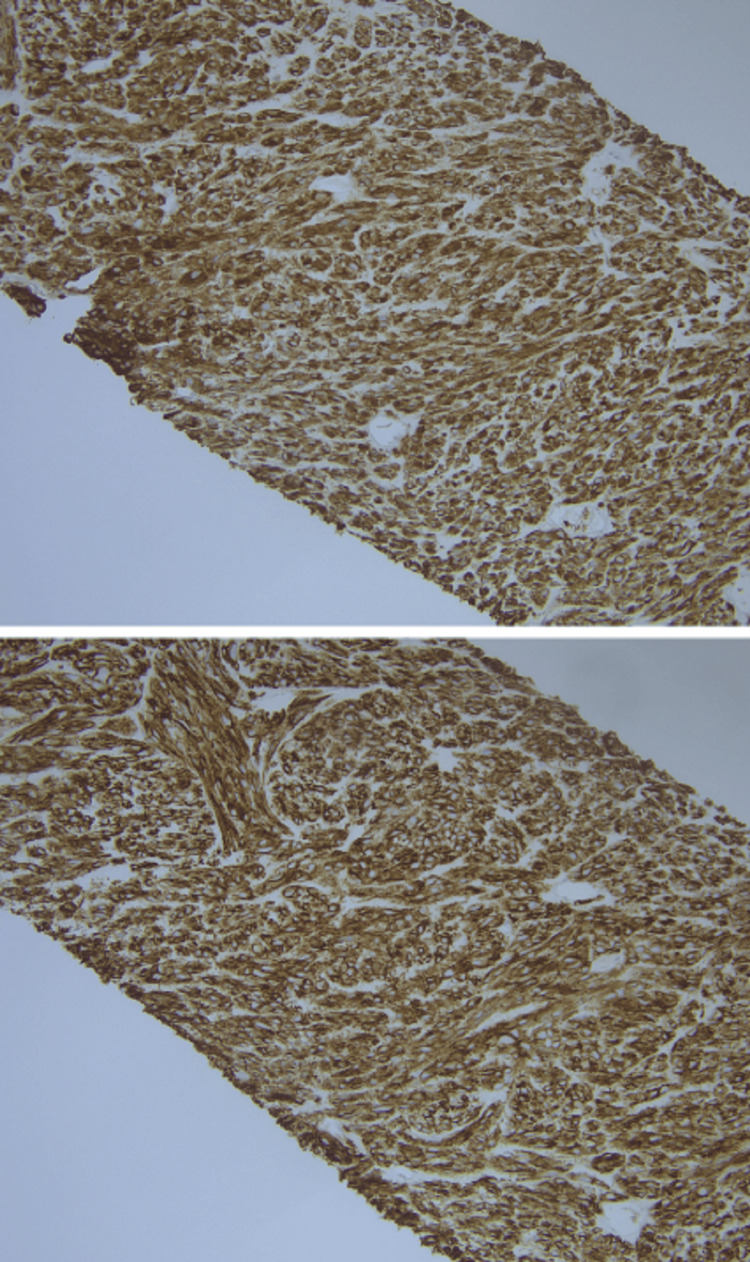 Figure 9
Figure 9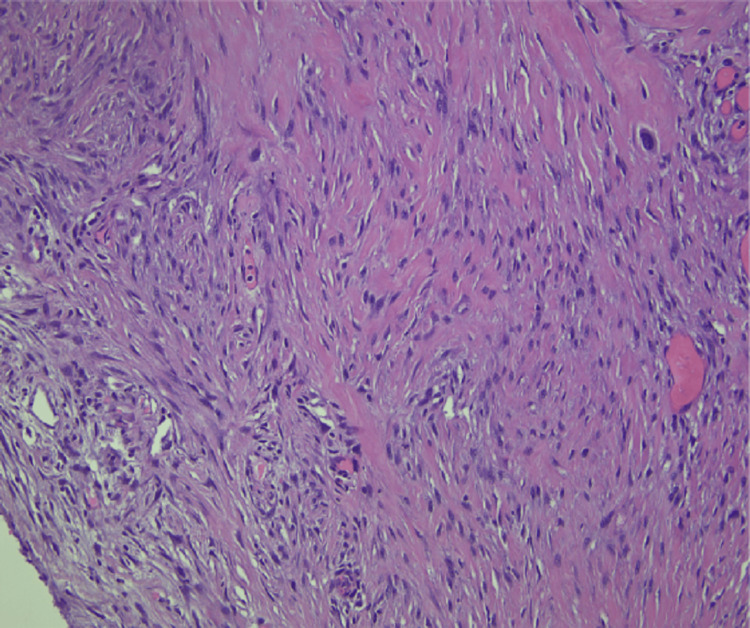 Figure 10
Figure 10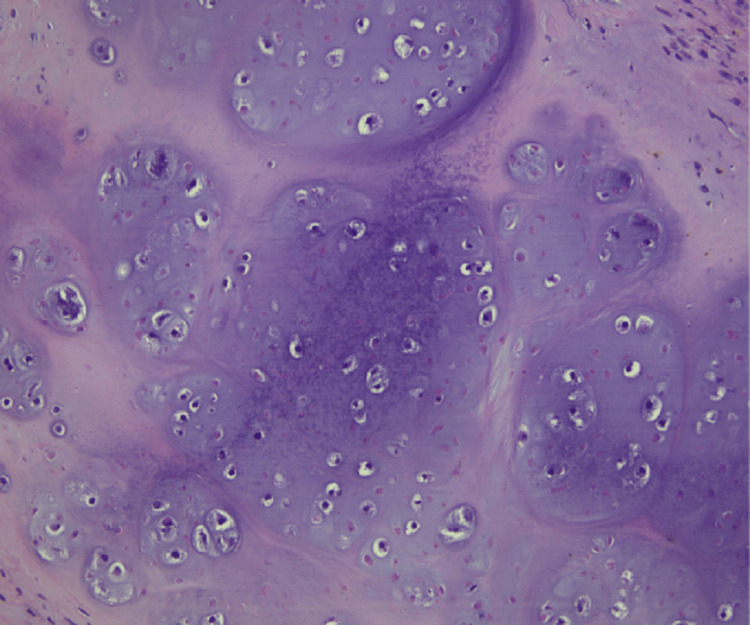 Figure 11
Figure 11| Year | Procedure/Specimen | Histomorphology | Immunohistochemistry/Molecular and Cytogenetics | Additional Findings |
| 2016 | Biopsy/Gastric Mass | Spindle cell type | Focally DOG1 (+), CD117 (+), Desmin (+), S100 (+), Cytokeratin AE1/AE3 (-), Low Molecular Weight Cytokeratin (-), High Molecular Weight Cytokeratin (-), CD34 (-), MelanA (-) | |
| 2016 | Partial Gastrectomy/Stomach Mass from Greater Curvature of Stomach | Spindle cell type with focal bizarre epithelioid cells and necrosis and mitotic rate of 23/50 HPF | No immunohistochemistry or molecular/cytogenetics was performed | Histologic grade G2, High Grade and Pathologic Stage pT4 |
| 2022 | Needle biopsy/Right mesenteric mass | Spindle cell type | DOG1 (+), CD117 (+) Ki-67 >30% with | |
| 2023 | Partial gastrectomy/Stomach Mass from Greater Curvature of Stomach | Spindle cell type with focal chondroid differentiation | Spindle cells: DOG (+), CD117 (-) in neoplastic cells and (+) in background cells and chondroid regions: DOG (-), CD117 (-) | Histologic grade G2, High Grade and Pathologic Stage pT4 |
| Antibody | Clone |
| Anti CD117 | YR145 |
| Anti DOG1 | SP31 |
| Anti Desmin | DE-R-11 |
| Anti S100 | Polyclonal |
| Cytokeratin AE1/AE3 | PCK26 |
| Low Molecular Weight Cytokeratin | 34 βE11 |
| High Molecular Weight Cytokeratin | 34 βE12 |
| Anti CD34 | QBEnd/10 |
| Anti MelanA | A103 |
| Article | Primary Location/Size | Histomorphology | Immunohistochemistry/Molecular and Cytogenetics | Additional Findings | Age/Sex |
| Yu et al., 2019 [ | Lesser curvature of gastric antrum/2.5 x 1.8 x 1.5 cm | Epithelioid cells arranged as chondroid cells in submucosa with myxoid degeneration and hyalinization in background, mitotic count less than 5/50 HPF | Tumor cells: DOG1 (+), CD117 (+), CD34 (+), and INI1 (+), Ki-67 (+) at 2%, S100 (-), SMA (-), Cytokeratin (unspecified type) (-), Desmin (-), HMB45 (-), Synaptophysin (-), NSE (-), EMA (-), MelanA (-). Molecular: | Patient also had poorly differentiated adenocarcinoma of stomach along with the GIST with chondroid differentiation | 64/Male |
| Musaad et al., 2016 [ | Between upper left pole of kidney and posterior gastric fundus/Size unspecified | Cartilage lobules surrounded by spindle-shaped cells without mitotic figures | Spindle cells: CD117 (+), S100 (+). Cartilage cells: S100 (+), CD117 (-) | The lesion was cystic and multilocular. GIST presented with abscess. | 38/Female |
| Brar et al., 2012 [ | Originated from greater curvature of stomach, adherent to diaphragm and liver, extended to pylorus /7012 grams | Chondroid matrix with discohesive epithelioid cells; other areas have more spindle-shaped cells with associated necrosis, hemorrhage, and high mitotic activity (65/50 HPF) | Tumor cells: CD117 (+), CD34 (+), CD 99(+), SMA (+), S100 (-). Molecular: Negative for | Gross appearance that is multinodular with areas of hemorrhage, necrosis, and cystic degeneration. There was a periumbilical mass that was part of the original tumor that was incarcerated in umbilical hernia and detached from original tumor | 84/female |
| Pulcini et al., 2009 [ | Fundus of stomach/7 x 5 cm | Spindle cell type with whorled pattern that surrounds area of chondroid differentiation | Spindle cells: CD117 (+), S100 (-), NSE (-), CK7(-), CK20(-), CD34 (-), MIB-1 (-), AML (-), AMS (-), chromogranin (-), alpha-1-antitrypsin (-), vimentin (-). Molecular: Negative for mutation in | MIB-1 index showed a low-grade GIST. Mutation for | 79/Female |
| Article | Primary Location/Size | Histomorphology | Immunohistochemistry/Molecular and Cytogenetics | Additional Findings | Age/Sex |
| Pulvers et al., 2020 [ | Stomach/130 mm | Primary GIST in stomach: Spindle cell morphology; Mitotic rate 18 per 5 mm2, Metastatic GIST to liver: Chondrocytes with mild cytologic atypia among scattered spindle cells in background of myxoid change and hyalinized stroma; cellular component is less than 5% of lesion. | Primary GIST in stomach: CD117 (+), DOG1 (+), subgroup of spindle cells desmin (+), Molecular for primary GIST: KIT exon 11 deletion variant c.1669_1674 deletion with p. (Trp557_Lys558del) variant. Metastatic GIST in liver: Spindle cells: Desmin (+), CD34 (-), CD117(-), and DOG1 (-), Molecular for metastatic GIST: KIT exon 11 deletion variant c.1669_1674 deletion with p. (Trp557_Lys558del) variant. | GIST metastasized to subcapsular region of liver measuring 28 mm; it was found 31 months after the initial resection of primary GIST. | 54/Female |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Neurofibromatosis and Schwannoma Cases
Introduction
Gastrointestinal stromal tumors (GISTs) are most frequently seen in the stomach (80%) and are the most common mesenchymal neoplasm in the gastrointestinal tract [1]. The most common histopathologic presentations of GIST include spindle cell type (70%), epithelioid cell type (20%), and mixed type (10%) [2,3]. The standard treatment of GIST includes surgical resection, and for more advanced tumors, either or both preoperative and postoperative imatinib therapy is administered [4].
There have been reports of changes in the histomorphologic features of GIST after imatinib therapy, both at the primary site and at the site of metastasis. Pauwels et al. described a case of a 46-year-old male patient with primary spindle-cell type GIST at the stomach that has metastasized to the liver. After imatinib therapy, there was a tubulopapillary and epithelioid growth pattern found in the liver [5]. There was another case described by Pulvers et al. of a 54-year-old female who had metastasized GIST to the liver and was found to have chondroid metaplasia in the liver at the site of the GIST post-imatinib therapy [6].
However, there has been no report of GIST with chondroid differentiation in a primary tumor site after imatinib therapy. This case highlights a unique presentation of GIST with chondroid differentiation after imatinib therapy. Furthermore, we provide a literature review of the documented cases of GIST with chondroid differentiation pre- and post-imatinib therapy to explore other possible ways cartilage is identified in GIST.
This case was previously presented as a meeting abstract at the 2023 American Society of Clinical Pathology Conference on October 18 and 19, 2023.
Case presentation
A 58-year-old female originally presented to the Emergency Department at Creighton University Medical Center-Bergan Mercy due to a syncopal episode and was incidentally found to have an 11 x 8.5 x 7 centimeters (cm) mass arising from the posterior wall and greater curvature of stomach on computed tomography scan (CT) of the abdomen (Figure 1).
CT Abdomen of Primary Gastrointestinal Stromal Tumor (GIST) in Posterior Wall and Greater Curvature of Stomach
Endoscopy was performed and gastroenterologists identified a large, fungating and ulcerated mass in the gastric body that was biopsied (Figure 2).
Mass in Gastric Body Found in Endoscopy Image
The initial biopsy of the gastric mass showed a spindle cell morphology and stained positively for DOG1 and CD117 (Figures 3, 4). The patient subsequently underwent a partial gastrectomy.
Hematoxylin and Eosin Stain of Needle Biopsy of Gastric Body Mass at 200x Magnification. Spindle cell Morphology is Identified in the Lamina Propria.
Immunohistochemical Stains DOG1 (Left) and CD117 (Right) of Needle Biopsy of Gastric Body Mass at 200x magnification. DOG1 and CD117 Both Highlight Spindle Cell Lesion.
Grossly, her initial partial gastrectomy showed a bulging subserosal multilobular tan to reddish-gray mass measuring 13.0 x 9.5 x 6.4 cm. Cut surfaces ranged from solid tan fibrous to vaguely whorled and trabeculated. The pathology of the initial gastrectomy found high-grade spindle cell type GIST with focal bizarre epithelioid cells (Figure 5).
Hematoxylin and Eosin Stain of Section from Initial Partial Gastrectomy of Gastrointestinal Stromal Tumor (GIST) on 200x Magnification. Orange Arrow Points at Focal Bizarre Epithelioid Cell in a Background of High-Grade Spindle Cell Lesion.
The patient was subsequently treated with imatinib for three years. During her annual CT surveillance imaging two years after imatinib therapy, she was found to have a heterogeneous, centrally necrotic lobulated mass in the central abdomen that abuts the stomach measuring 11.8 x 11.7 x 6.7 cm, compatible with localized recurrence (Figure 6). Positron Emission Tomography-Computer Tomography also found a heterogeneously hypermetabolic mass from the body and greater curvature of the stomach with necrotic areas measuring 11.6 x 10.9 x 7.1 cm with dominant metabolic activity in the right inferior aspect of the mass (Figure 7). Additionally, there were hypermetabolic nodes anterior to the mass that were suspicious for metastasis.
CT Abdomen of Recurrent Gastrointestinal Stromal Tumor (GIST) Before (Left) and After (Right) Second Course of Imatinib Therapy
Positron Emission Tomography-Computed Tomography in Coronal (A), Sagittal (B), and Axial (C) Planes. Corresponding Computed Tomography of Abdomen with Red Outline Identifying Mesenteric Mass and Blue Outline Identifying Lymph Node (D).
The pathology from the biopsy of the right mesenteric mass showed spindle cell morphology on hematoxylin and eosin stain (Figure 8) and was positive for DOG1 and CD117 on immunohistochemistry (Figure 9). The patient subsequently underwent another partial gastrectomy. The mass measured 10.4 x 9.1 x 4.4 cm and had a heterogenous cut surface with tan-gray at the periphery and tan-yellow necrosis in the center. Additionally, the tumor appears to have invaded the adjacent adipose tissue.
Hematoxylin and Eosin Stain of Needle Biopsy of Right Mesenteric Mass on 200x Magnification. Tissue with Spindle Cell Morphology is Present.
Immunohistochemical Stains CD117 (Top) and DOG1 (Bottom) of Right Mesenteric Mass at 200x Magnification.
The tissue sections showed high grade spindle-cell morphology with chondroid differentiation (Figures 10, 11). After discovery of recurrent GIST, the patient was restarted on imatinib therapy. Table 1 outlines pertinent information in the pathology reports pertaining to our patient’s GIST diagnosis.
Hematoxylin and Eosin Stain of Partial Gastrectomy for Recurrent Gastrointestinal Stromal Tumor (GIST) at 200x Magnification. Tissue Section Shows Spindle-Cell Morphology.
Hematoxylin and Eosin Stain of Partial Gastrectomy for Recurrent Gastrointestinal Stromal Tumor (GIST) at 200x Magnification. Tissue Section Shows Chondroid Differentiation.
For processing of the tissue, the tissue was immersed in 10% formalin for fixation. The selected sections were then dehydrated, paraffin embedded, and cut into 4 μm sections for hematoxylin and eosin stain.
For immunohistochemical staining, the laboratory uses UltraView© or OptiView© detection kit with a known positive control. All antibodies except anti-CD117 were purchased from Ventana (Oro Valley, AZ, USA). Anti-CD117 was purchased from Cell Marque (Rocklin, CA, USA). The antibodies and their respective clones are shown in Table 2.
For molecular testing, the mesenteric mass biopsy specimen was sent out to NeoGenomics (Fort Myers, FL, USA) for testing of the PDGFRα and *c-KIT *mutation. Per the NeoGenomics report, molecular analysis for *c-KIT *mutation is accomplished when nucleic acid is isolated from formalin-fixed paraffin-embedded tissue. The mutations are tested with the Sanger sequencing bidirectional method and KIT exons 8, 9, 11, 13, and 17 were evaluated. PDGFRα hotspots in exons 12 and 18 were also evaluated using Sanger bidirectional sequencing.
Discussion
We performed a review of existing literature and identified five patients reported to have GIST with chondroid differentiation. Four patients had GIST with chondroid differentiation prior to imatinib therapy and one patient had GIST with chondroid differentiation after imatinib therapy. The patient with GIST post-imatinib therapy was found to have GIST with chondroid differentiation at the site of metastasis. The patients’ mean age was 64 and ranged from 38 to 79 years old. Four of five patients were female, including the only patient who had chondroid differentiation in metastatic GIST post-imatinib therapy. Table 3 and Table 4 summarize the demographics and pertinent pathology findings for the cases we identified for patients before and after imatinib therapy, respectively.
GISTs vary in risk of malignancy based on anatomic site, mitotic rate, and size [11,12]. Our patient had high histologic grade both in the primary GIST and recurrent GIST. Furthermore, the size of the tumor and mitotic index of our patient put the patient in a high risk for malignancy stratification [13].
There are multiple reported cases of histomorphologic alterations after imatinib therapy that do not include chondroid differentiation. Pauwels et al. report a case of a 46-year-old male patient with a primary GIST in the stomach with spindle-shaped morphology that subsequently metastasized to various parts of the intra-abdominal region. Hematoxylin and eosin-stained tissue sections showed large epithelioid cells that resemble carcinomatous, melanoma-like and histiocytic proliferation in the duodenum after imatinib therapy [5]. Karakas et al. also reported a case with a 69-year-old male who had spindle and epithelioid type GIST. After imatinib therapy, his GIST was dedifferentiated and had anaplastic features with high mitotic activity and nuclear atypia [14].
GISTs have a wide variety of histomorphologic presentations both before and after imatinib therapy, though few have presented with chondroid differentiation. This article identified four documented incidences of patients with GIST with chondroid differentiation prior to imatinib therapy and one case of GIST with chondroid differentiation after imatinib therapy. The chondroid differentiation after imatinib therapy occurred at the site of metastasis. Therefore, our case of GIST is the first reported case to have chondroid differentiation at the primary recurrence site after imatinib therapy.
Conclusions
Our case and literature review highlight the importance of identifying the various histomorphologic changes that GIST can undergo before and after imatinib therapy. The case also illustrates the diagnostic challenges pathologists may encounter in evaluating patients with recurrent GIST post-imatinib therapy. Furthermore, this case report and literature review reflects how processes such as chondroid differentiation should be considered for these patients alongside histomorphologic mimickers such as chondrosarcoma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and management of gastrointestinal stromal tumors: an up-to-date literature review J Cancer Res Ther El-Menyar A Mekkodathil A Al-Thani H 8899001320172923794910.4103/0973-1482.177499 · doi ↗ · pubmed ↗
- 2The standard diagnosis, treatment, and follow-up of gastrointestinal stromal tumors based on guidelines Gastric Cancer Nishida T Blay JY Hirota S Kitagawa Y Kang YK 3141920162627636610.1007/s 10120-015-0526-8PMC 4688306 · doi ↗ · pubmed ↗
- 3Current clinical management of gastrointestinal stromal tumor World J Gastroenterol Akahoshi K Oya M Koga T Shiratsuchi Y 280628172420183001847610.3748/wjg.v 24.i 26.2806 PMC 6048423 · doi ↗ · pubmed ↗
- 4Gastrointestinal stromal cancer Stat Pearls [Internet] Burch J Ahmad I Treasure Island Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 554541/32119428 · pubmed ↗
- 5Changing phenotype of gastrointestinal stromal tumours under imatinib mesylate treatment: a potential diagnostic pitfall Histopathology Pauwels P Debiec-Rychter M Stul M De Wever I Van Oosterom AT Sciot R 41474720051598232210.1111/j.1365-2559.2005.02179.x · doi ↗ · pubmed ↗
- 6Decoding a mysterious morphology with molecular pathology: chondroid metaplasia in a metastatic gastrointestinal stromal tumour after imatinib therapy Pathology Pulvers J Guminski A Chou A Gill AJ Ahadi M 3963985220203211139710.1016/j.pathol.2019.12.007 · doi ↗ · pubmed ↗
- 7Chondroid gastrointestinal stromal tumor in the stomach with early adenocarcinoma Int J Clin Exp Pathol Yu G Yang P Ran W 16421648122019 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 6947111/31933982 PMC 6947111 · pubmed ↗
- 8Gastric GIST with chondroid differentiation presented with gastric abscess - a case report and literature review Arab J Gastroenterol Musaad AM Arabi NA Hussein T 56591720162657647310.1016/j.ajg.2015.07.001 · doi ↗ · pubmed ↗