Mycosis Fungoides: A Necessary Differential Diagnosis in Infectious Disease and Dermatology Settings
Claudio José dos Santos, Aryanna Kelly Pinheiro Souza, Thiago José Matos Rocha

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1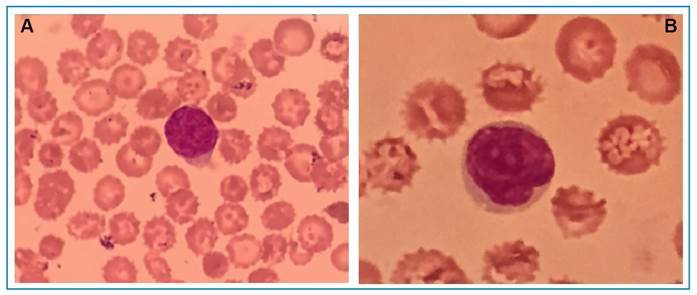 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Fungal Infections and Studies · Nail Diseases and Treatments
A 69-year-old male presented to the Infectious Disease Service with erythematous scaly lesions persisting for five years, which had evolved into diffuse exfoliative erythroderma and multiple disseminated scaly plaques in the three weeks preceding admission. Physical examination revealed infiltrated facial appearance, serous blistering, ulcerated lesions in the oral and genital mucosa, infiltrated plaques on the face and auricular pavilion, crusted scaly plaques on the anterior/posterior trunk and upper and lower limbs with lesion exulceration, intense pruritus, fever, arthralgia, and diffuse lymphadenopathy w(Figure 1). Laboratory findings at admission included LDH 672 U/L, PCR 152.91 mg/dL, 75,000 leukocytes/µL, atypical lymphocytes, and convoluted nucleus lymphomatous cells suggestive of Sézary cells (10-15% in peripheral blood smears) (Figure 2). The clinical course was unfavorable, with a worsening state after 10 days, preceding specific interventions.
FIGURE 1A AND 1B:Disseminated ulcerations and erythroderma on the chest, back, and cervical regions.
FIGURE 2A AND 2B: Sézary cells with convoluted nuclei in peripheral blood (Giemsa, x1000).
The challenging diagnosis of cutaneous T-cell lymphoma, particularly mycosis fungoides (MF), stems from nonspecific clinical-laboratory findings1. The annual incidence of T-cell cutaneous lymphoma is extremely low, at 0.77/100,000 individuals, with an estimated incidence of 0.41/100,000 for MF2.
In this case, the variable symptomatic manifestations did not indicate early MF. Extensive desquamative plaques and ulcerated/infected lesions were the reasons for admission, while the detection of Sézary allowed formulation of a diagnostic hypothesis.
MF significantly resembles various benign inflammatory skin conditions3. However, delayed diagnosis, as seen here, amplifies the likelihood of unfavorable outcomes4.
Thus, a cautious approach is warranted in infectious diseases and dermatology settings, considering MF as a differential diagnosis in presentations hinting at it.
ETHICS
The study was approved by the Institutional Ethics Committee (CAAE 33818720.6.0000.5011).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amorim GM Quintella DC Niemeyer-Corbellini JP Ferreira LC Ramos-e-Silva M Cuzzi T Validation of an algorithm based on clinical, histopathological and immunohistochemical data for the diagnosis of early-stage mycosis fungoides An Bras Dermatol 20209533263313231713210.1016/j.abd.2020.01.002PMC 8074686 · doi ↗ · pubmed ↗
- 2Lobato BADL Brito JAGSM Carneiro TX Xavier MB Diagnóstico tardio de micose fungoide: um relato de caso Rev Pan-Amaz Saude 202112 e 202100820
- 3Miyashiro D Sanches JA Mycosis fungoides and Sézary syndrome: clinical presentation, diagnosis, staging, and therapeutic management Front Oncol 202313114110811411083712451410.3389/fonc.2023.1141108 PMC 10140754 · doi ↗ · pubmed ↗
- 4Eklund Y Aronsson A Schmidtchen A Relander T Mycosis Fungoides: A Retrospective Study of 44 Swedish Cases Acta Derm Venereol 201696566967310.2340/00015555-233726778803 · doi ↗ · pubmed ↗