Reversed halo sign in a patient with septic embolism
Louise Fátima Gomes-Almeida, Nathalia Christina Lopes Flores, Beatriz Rodrigues Bozza, Edson Marchiori

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
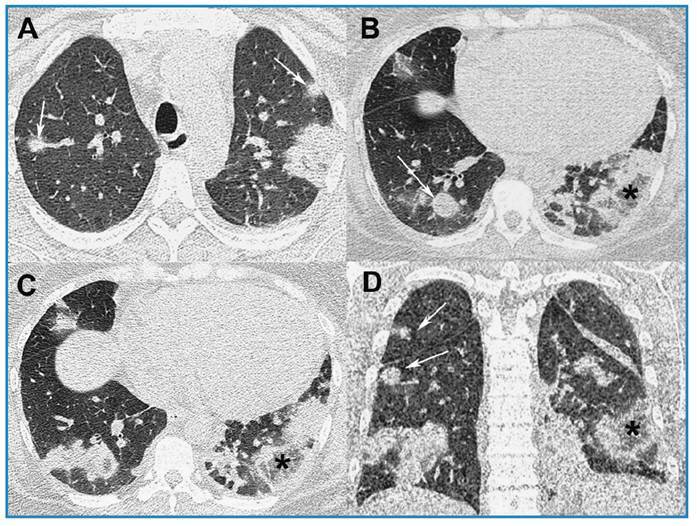 Figure 1
Figure 1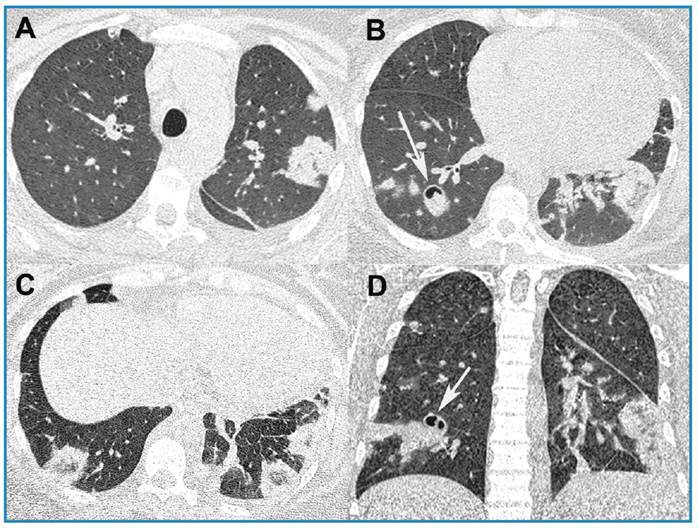 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLegionella and Acanthamoeba research · Infective Endocarditis Diagnosis and Management · Neutrophil, Myeloperoxidase and Oxidative Mechanisms
A 37-year-old woman with chronic renal failure and mitral insufficiency presented a 15-day history of fever, cough, and dyspnea after hemodialysis. On physical examination, she was eupneic on room air, with 97% O_2_ saturation, and was hemodynamically stable. Laboratory tests revealed leukocytosis (leukocyte count, 18,000/mm^3^), and elevated C-reactive protein (26.3 mg/L). Blood hemocultures were positive for methicillin-sensitive Staphylococcus aureus. Infection was observed around the hemodialysis catheter. Unenhanced chest computed tomography (CT) revealed multiple bilateral pulmonary nodules, areas of consolidation, and ground-glass attenuation, some forming reversed halo signs (RHSs; Figure 1). Septic pulmonary embolism (PE) was diagnosed, and antibiotic treatment was initiated, which improved the symptoms. CT examination after five days of treatment initiation revealed partial improvement in opacities, with cavitation of some nodules (Figure 2). The patient was discharged in a stable condition.
FIGURE 1:Chest computed tomography images with axial (A-C) and coronal (D) reconstruction showing multiple ill-defined nodules in both lungs (arrows) and areas of ground-glass opacities and consolidations, some forming reversed halo signs (asterisks).
FIGURE 2:Chest computed tomography images obtained five days after the first examination in the same planes. demonstrating partial resolution of lesions, some of which show cavitation (arrows).
CT findings in septic PE mostly include peripheral nodules with or without cavitation1. The RHS is a chest CT pattern defined as a focal, rounded area of ground-glass opacity surrounded by a complete or nearly complete ring of consolidation. This sign has been observed in several infectious and non-infectious diseases2 ^,^ 3, but rarely in cases of septic embolism. However, RHS was recently reported in more than half of intravenous drug users with septic emboli, several of which showed cavitation3. Septic PE should thus be considered in the differential diagnosis of patients presenting RHS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tufanoğlu FH Akyüz B Bekirçavuşoğlu S Septic embolism of the lung due to spondylodiscitis Rev Soc Bras Med Trop 202255 e 0662202110.1590/0037-8682-0662-202135416882 PMC 9009876 · doi ↗ · pubmed ↗
- 2Godoy MC Viswanathan C Marchiori E Truong MT Benveniste MF Rossi S The reversed halo sign: update and differential diagnosis Br J Radiol 20128510171226123510.1259/bjr/5453231622553298 PMC 3487053 · doi ↗ · pubmed ↗
- 3Almeida RR Marchiori E Flores EJ Frequency and Reliability of the Reversed Halo Sign in Patients With Septic Pulmonary Embolism Due to IV Substance Use Disorder AJR Am J Roentgenol 20202141596710.2214/AJR.19.2165931670590 · doi ↗ · pubmed ↗