Off-label use of muscular VSD device for closure of a rare congenital portosystemic shunt
Hala Mounir Agha, Shady Mashoor, Mohamed Ghobashy, Antoine AbdelMassih, Hanya Gaber, Hanaa El-Karaksy

TL;DR
A 10-year-old patient with a rare congenital portosystemic shunt leading to pulmonary hypertension was successfully treated using a muscular VSD device.
Contribution
This case demonstrates the successful use of a muscular ventricular septal defect device for closure of a rare congenital portosystemic shunt.
Findings
A muscular VSD device was used to close a CPSS in a pediatric patient.
Pulmonary hypertension was reversed following the procedure.
CPSS is a reversible cause of pulmonary hypertension that can be treated via catheterization.
Abstract
Congenital portosystemic shunt (CPSS) is a vascular malformation in which portal blood drains toward the systemic circulation, leading to pulmonary hypertension. A 10-year-old patient was brought for evaluation because of dyspnea on exertion. Echocardiography revealed a pulmonary hypertension of 75 mmHg, and multi-slice CT angiography revealed the presence of a CPSS. Closure was finally implemented using a muscular ventricular septal defect device. Follow-up of the patient revealed a gradual decline in pulmonary hypertension. CPSS is an overlooked cause of reversible pulmonary hypertension (PH). Closure of such lesions and reversal pulmonary hypertension are possible via catheterization. The preferred device type depends largely on the intervening team. Plugs are the first choice for interventional radiologists, while ventricular and atrial septal occluder devices and duct occluders…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
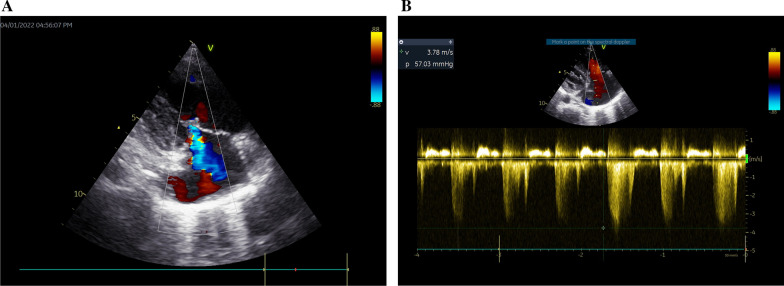 Figure 1
Figure 1 Figure 2
Figure 2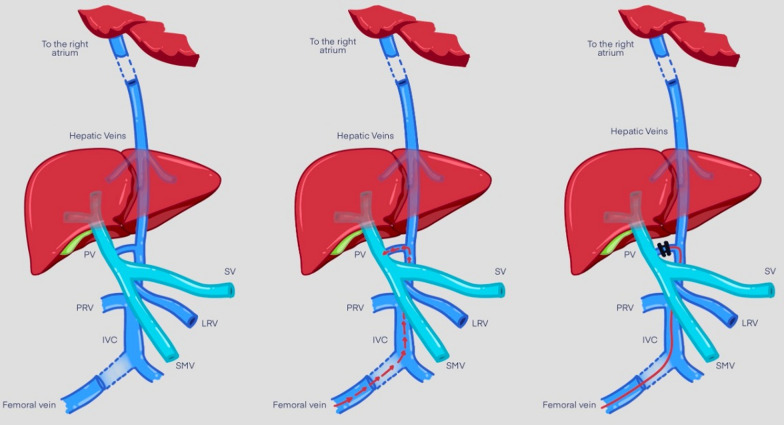 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments · Congenital Heart Disease Studies · Liver Disease and Transplantation
Background
Congenital portosystemic shunt (CPSS), also known as Abernethy malformation, is a rare vascular malformation in which portal blood drains into the systemic circulation, eluding the liver [1, 2].
According to the physiopathological theory, when vasoactive substances present in the intestinal circulation (e.g., serotonin, histamine, estrogen, glucagon) bypass the liver without being metabolized and pass through a CPSS, this results in pulmonary arterial hypertension (PAH) caused by the induction of long-lasting pulmonary vasoconstriction [3, 4].
CPSS has a wide spectrum of manifestations that can occur at any point in an individual's life, although asymptomatic cases that are incidentally detected on imaging are also common. In children, long-term portosystemic shunting leads to the most prominent manifestations such as hepatopulmonary syndrome, pulmonary hypertension, and hepatic encephalopathy. Even before birth, a disruption in fetal venous circulation caused by shunting may result in reduced liver perfusion and signs of intrauterine growth restriction, without the presence of hypoxia, maternal infections, and/or chromosomal abnormalities. Neonatal cholestasis and galactosemia are among the complications that may arise and should be distinguished from other congenital defects such as biliary atresia and metabolic disorders that may coexist [5, 6].
Case presentation
Case description
A 10-year-old patient was brought for evaluation because of easy fatigability and dyspnea on exertion, with no clinically appreciable cyanosis. Patient anthropometric measurements showed mainly failure to thrive with a preserved stature centile; weight was 19 kg (< 5th percentile for age and sex), while stature was 125 cm (25th percentile for age and sex). Pulmonary hypertension was evident in the accentuated pulmonary component of the 2nd heart sound. Significant right atrial and ventricular dilatation were elicited by echocardiography, along with an estimated systolic pulmonary arterial pressure of 62–67 mmHg, obtained via tricuspid regurgitant jet (Fig. 1A–B). Left-to-right shunts and underlying cardiac abnormalities were not observed.Fig. 1A Tricuspid regurgitant jet. B Continuous wave Doppler gradient across the across the tricuspid regurgitant jet
Before concluding the diagnosis of primary pulmonary hypertension, multi-slice CT angiography was performed, which revealed the presence of CPSS.
Transcatheter closure of the portosystemic shunt was then attempted. For this purpose, a 6 Fr femoral vein, a 5 Fr Internal jugular vein access, and a 5 Fr femoral arterial access were prepared. Invasive hemodynamics were observed, which revealed elevated pulmonary vascular resistance. Inferior vena cava (IVC) injection revealed a previously identified fistulous malformation between it and the portal vein. It is conical in shape, with the largest diameter at the vena cava side (approximately 8 mm). The first attempt was performed using a Lifetech ductal occluder I DOI (8/6) device (Lifetech Scientific, Shenzhen, China) for shunt closure, but unfortunately, it was unstable in position and slipped into the IVC. A decision was made to close it using a Lifetech muscular mVSD device with a size of 8 mm (Lifetech Scientific, Shenzhen, China). A 4F Judkins Rt catheter under Terumo wire guidance in the IVC was used to cross the fistula to the portal vein. The Terumo wire was withdrawn and replaced by a stiff wire 0.035 × 260 cm to secure the position in the portal vein, which was then withdrawn and replaced by a multipurpose 5 Fr catheter to support the delivery system of the muscular device. The device was loaded onto a 7 Fr Lifetech delivery system, and the entire system was advanced along the guidewire and multipurpose catheter. Once part of the portal vein adjacent to the fistula was reached, the device was released progressively to seal the CPSS. Repeated injections revealed adequate closure of the fistula. (Figs. 2A–D and 3).Fig. 2A IVC angiogram showing CPSS. CPSS Congenital portosystemic shunt, IVC Inferior vena Cava, SMV Superior mesenteric vein. B Prolapsed ADO device. ADO Amplatzer duct occluder, CPSS Congenital portosystemic shunt, IVC Inferior vena Cava, PDA Patent ductus arteriosus, SMV Superior mesenteric vein. C Muscular Device placed across the fistula before deployment CPSS Congenital portosystemic shunt, IVC Inferior vena Cava, SMV Superior mesenteric vein. D Muscular Device placed across the fistula after deployment. IVC Inferior Vena Cava, mVSD Muscular ventricular septal defectFig. 3Diagram of the approach used for closure of the CPSS. Parts: Part 1 showing the fistula/Part 2: Shows the pathway used for closure, Part 3 shows the device across the fistula. IVC Inferior vena cava, LRV Left renal vein, PV Portal vein, SV Splenic vein, SMV Superior mesenteric vein.
Discussion of the case
Due to the increased levels of humoral substances in the lung tissue, chronic pulmonary vasoconstriction can occur in patients with CPSS. Our patient presented with difficulty breathing due to severe pulmonary hypertension, in addition to hyperammonemia due to concomitant liver dysfunction [4].
Kuo and colleagues performed the first endovascular closure of a portosystemic shunt in 2010. They used a three-stage approach due to associated portal vein hypoplasia. Subsequently, several studies have been published [7].
It is noticeable from the cases summarized in our table that interventional radiologists rely on vascular plugs in the closure of this malformation, whereas pediatric cardiologists perform most of their procedures using duct, atrial septal, and ventricular septal occluders. Vascular plugs are primarily used to treat extracardiac defects. Perhaps this is the reason why they are rarely used by interventional cardiologists and thus rarely available in pediatric cardiac catheter laboratories. This probably explains the bias in the devices used by different teams to close the same defect.
Table 1 shows reports where the endovascular approach was used for CPSS closure [7–13].Table 1. Examples of endovascular approach to congenital portosystemic shuntsYearType of publication/number of patientsAuthorService provided byPresenting manifestationAgeSize of the shuntType of occluding device2010Case report/1Kuo et alInterventional radiologyProgressive cyanosis11 years14 mmGraded closure using covered stents to allow growth of portal veins followed by complete closure by vascular plug2012Case report/1Passalacqua et alInterventional RadiologyProgressive cyanosis3 years10 mmVascular plug 10 mm2013Case Series/4Bruckheimer et alPediatric cardiologyFour patients all presenting with hepatic encephalopathy2.5 years, 4 years, 8 and 10 yearsNot reportedGraded closure using covered stents followed by duct occluder2017Case report/1AlHarbi et alPediatric Cardiology and Interventional radiologyHepatic encephalopathy1 month-old4 mmDuct occluder 12 × 6 mm2017Case series/2Tomiyama et alPediatric RadiologyTwo patients presenting with Hepatic encephalopathy75 and 83 years oldNot reported22- and 14-mm vascular plugs, respectively2021Case report/1Facas et alInterventional RadiologyAsymptomatic: during routine screening of liver functions before isotretinoin therapy for acne15 years16 mm16 mm atrial septal occluder followed by 14 mm vascular plug2021Case report/1Shnayder et alInterventional RadiologyHepatic encephalopathy2 years14 mm18 mm patent foramen ovale device2022Case series/21Koneti et alPediatric cardiology11 with progressive cyanosis6 with pulmonary hypertension2 with hepatic encephalopathy2 with pulmonary hypertension and progressive cyanosis0.45 to 19 years7–16 mmTen with vascular plugsSix with muscular ventricular septal defect (VSD)deviceFour by septal occluderGraded closure using covered stents followed by Muscular VSDOne by duct occluder
A very important consideration to be taken into consideration, during and after closure, is the possible hypoplasia of intrahepatic pulmonary veins. This hypoplasia is either managed with staged repair or with close follow-up every 3–6 months for any signs of portal hypertension and serial ammonia measurements after shunt closure. Nevertheless, prolonged intrahepatic hypoxia can stimulate neoplastic activity and nodule formation; therefore, experts recommend annual abdominal ultrasound to detect any liver neoplasm [6].
Conclusions
When dealing with PAH patients, CPSS should be ruled out, despite its rarity, especially in the pediatric field. The damage caused by PAH can be reversed by transcatheter shunt closure. The endovascular approach has supervened classic surgical ligation, and off-label use of intracardiac devices is increasingly being implemented.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yi J-E Jung H-O Youn H-JA case of pulmonary arterial hypertension associated with congenital extrahepatic portocaval shunt J Korean Med Sci 20142960410.3346/jkms.2014.29.4.60424753712 PMC 3991808 · doi ↗ · pubmed ↗
- 2Ecochard-Dugelay E Lambert V Schleich J-M Portopulmonary hypertension in liver disease presenting in childhood J Pediatr Gastroenterol Nutr 20156134635410.1097/MPG.000000000000082125885880 · doi ↗ · pubmed ↗
- 3Simonneau G Gatzoulis MA Adatia I Updated clinical classification of pulmonary hypertension J Am Coll Cardiol 201362 D 34D 4110.1016/j.jacc.2013.10.02924355639 · doi ↗ · pubmed ↗
- 4Ivy DD Abman SH Barst RJ Pediatric pulmonary hypertension J Am Coll Cardiol 201362 D 117D 12610.1016/j.jacc.2013.10.02824355636 · doi ↗ · pubmed ↗
- 5Papamichail M Pizanias M Heaton N Congenital portosystemic venous shunt Eur J Pediatr 201817728529410.1007/s 00431-017-3058-x 29243189 PMC 5816775 · doi ↗ · pubmed ↗
- 6Xu S Zhang P Hu L Case report: clinical features of congenital portosystemic shunts in the neonatal period Front Pediatr 202110.3389/fped.2021.77879134926351 PMC 8674941 · doi ↗ · pubmed ↗
- 7Kuo MD Miller FJ Lavine JE Exploiting phenotypic plasticity for the treatment of hepatopulmonary shunting in abernethy malformation J Vasc Interv Radiol 20102191792210.1016/j.jvir.2010.01.03820399112 · doi ↗ · pubmed ↗
- 8Alharbi A Abdulrahman S Al Otaibi M Congenital extrahepatic portosystemic shunt embolization with the use of a duct occluder in a neonate with liver dysfunction and hyperammonemia J Vasc Interv Radiol 2017281291129310.1016/j.jvir.2017.05.01628841939 · doi ↗ · pubmed ↗