ECG Changes Post-pericardiocentesis for Cardiac Tamponade Secondary to Non-small Cell Carcinoma of the Lung
Kyle Aldridge, Kevin E Guzman, Russell W Barry, Margaret A Franklin Christian, Felipe Ruiz, Ilya Fonarov, Damian Casadesus

TL;DR
A patient with lung cancer developed cardiac tamponade, and ECG changes resolved after pericardiocentesis.
Contribution
A case report showing ECG normalization after pericardiocentesis in a patient with lung cancer-related cardiac tamponade.
Findings
Electrical alternans on ECG resolved after draining pericardial effusion.
Biopsy confirmed poorly differentiated non-small cell lung adenocarcinoma.
Cardiac tamponade symptoms improved following pericardiocentesis.
Abstract
Electrical alternans on electrocardiograph (ECG) is an uncommon but nearly pathognomonic sign of cardiac tamponade. Here, we present a male quadragenarian who came to the emergency department complaining of low back and right upper abdominal pain. Work-up revealed a large pericardial effusion associated with electrical alternans on ECG and clinical findings of cardiac tamponade. Pericardiocentesis drained approximately 1 liter of hemorrhagic fluid with resolution of cardiac tamponade and normalization of the ECG. Further evaluation with right hilar lymph node biopsy confirmed a diagnosis of poorly differentiated non-small cell adenocarcinoma of the lung.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
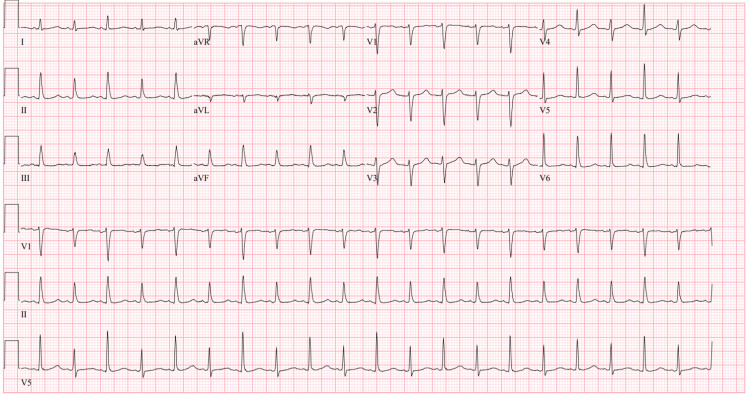 Figure 1
Figure 1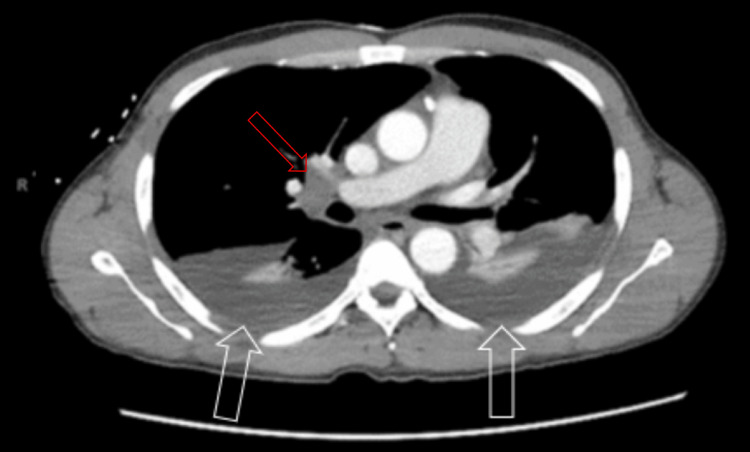 Figure 2
Figure 2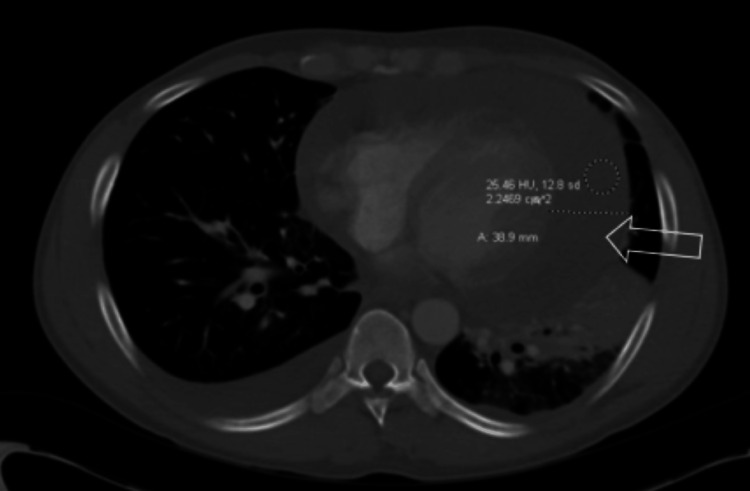 Figure 3
Figure 3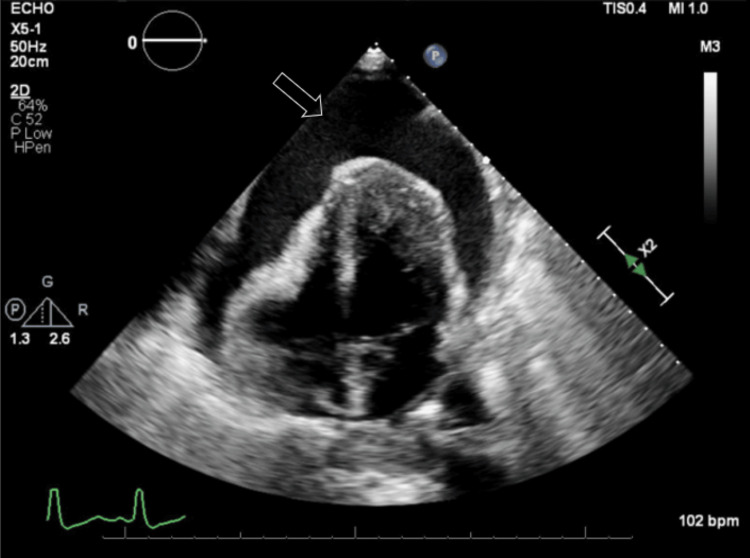 Figure 4
Figure 4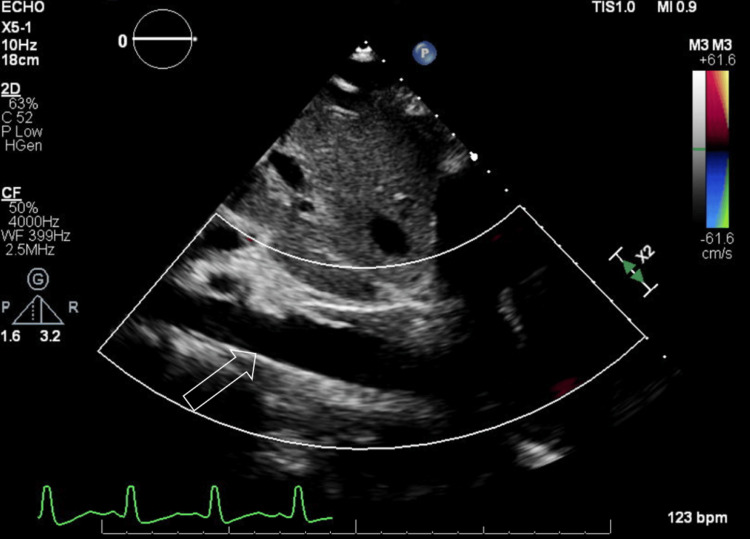 Figure 5
Figure 5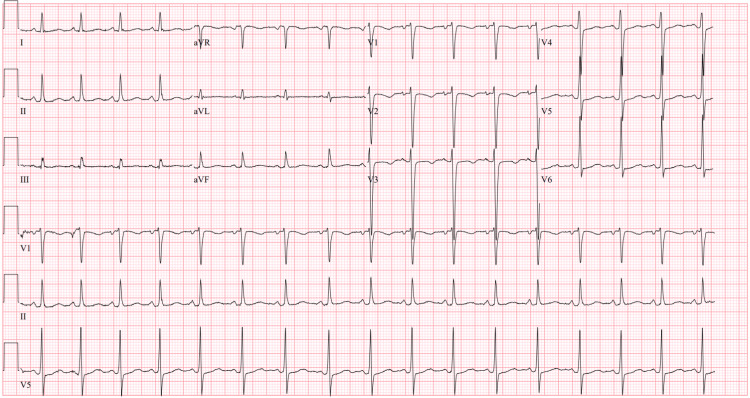 Figure 6
Figure 6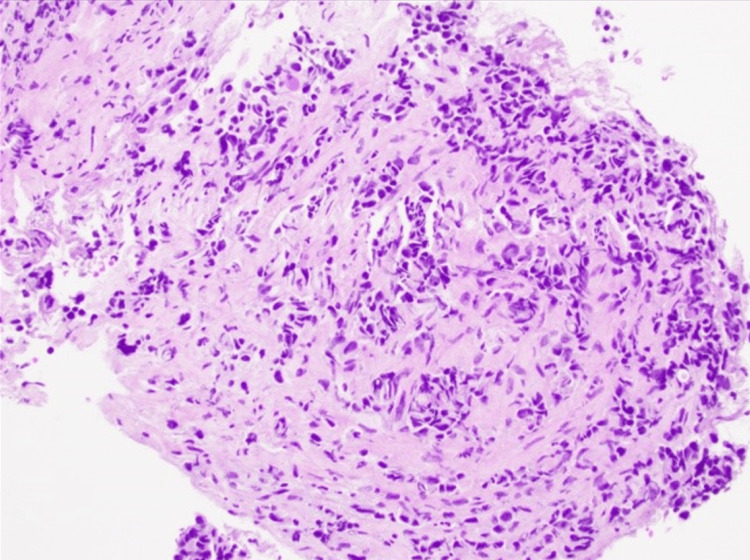 Figure 7
Figure 7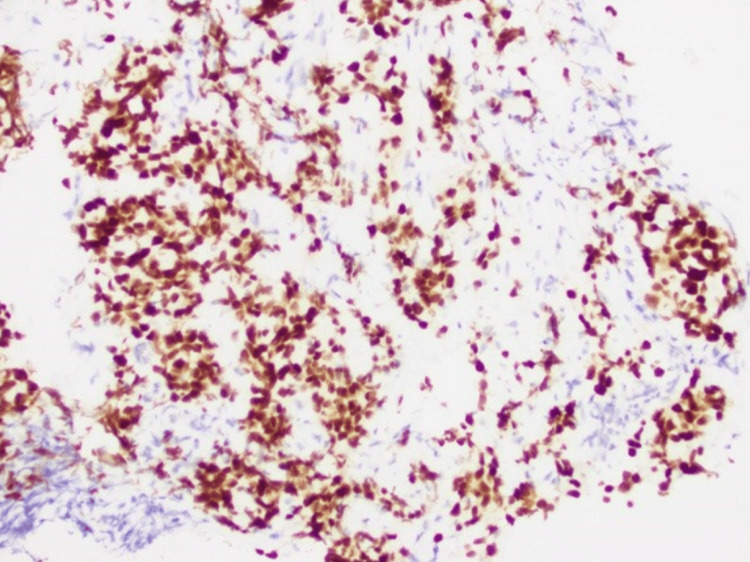 Figure 8
Figure 8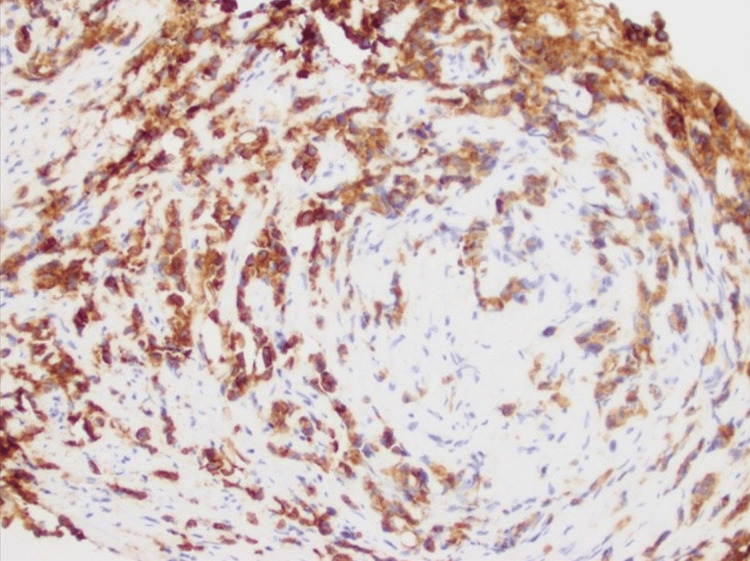 Figure 9
Figure 9| Investigation | Patient values | Reference values |
| BUN | 23 mg/dL | 6-24 mg/dL |
| Creatinine | 1.9 mg/dL | 0.7-1.3 mg/dL |
| CRP | 5.6 mg/dL | <0.3 mg/dL |
| Hemoglobin | 10.8 g/dL | 13.8-17.2 g/dL |
| Hematocrit | 33.7% | 41-50% |
| Platelets | 204 x 109/L | 150-450 x 109/L |
| Leukocytes | 10.3 x 109/L | 4.5-11 × 109/L |
| Troponin | <0.012 ng/mL | <0.04 ng/mL |
| BNP | 113 pg/mL | <100 pg/mL |
| AST | 4608 U/L | 8-33 U/L |
| ALT | 2134 U/L | 7-56 U/L |
| ALP | 105 U/L | 44-147 U/L |
| LDH | 5,299 U/L | 105-233 U/L |
| Total protein | 5.2 g/dL | 6.0-8.3 g/dL |
| Albumin | 2.6 g/dL | 3.4-5.4 g/dL |
| CPK | 479 mcg/L | 10-120 mcg/L |
| LDH | 5,299 U/L | 140-280 U/L |
| INR | 1.81 | <1.1 |
| Investigation | Patient values | Reference values |
| RBC | 2,049,527/mm3 | 0 |
| Nucleated cells | 8,318/mm3 | <200/mm3 |
| LDH | 5299 U/L | 141-2613 U/L |
| Glucose | 14 mg/dL | 80-134 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Takotsubo Cardiomyopathy and Associated Phenomena · Cardiac Structural Anomalies and Repair
Introduction
Cardiac tamponade is a life-threatening condition characterized by the abnormal accumulation of fluid in the pericardial space. It is common for patients to present in distress and they often complain of chest pain and dyspnea. Physical exam findings reflect the decreased filling capacity of the heart chambers, leading to tachycardia, hypotension, jugular venous distension, and pulsus paradoxus [1]. Findings on electrocardiograph (ECG) may include electrical alternans, low QRS voltage, P wave, and T wave changes [2]. Here, we showcase the resolution of electrical alternans on ECG after pericardial effusion drainage.
Case presentation
A male in his 40s with no significant past medical history presented to the emergency department complaining of lower back and right upper abdominal pain. He reported nausea and vomiting for four days preceding the visit, along with a cough. He denied any fever, weight loss, chest pain, or shortness of breath. He did not have any history of tobacco use but engages in social alcohol consumption and smokes marijuana weekly. While in the emergency room, he was afebrile and tachycardic at 121 beats per minute and had a blood pressure of 96/64 mmHg. A cardiopulmonary exam revealed distant heart sounds. The patient had 2+ pedal edema. Abdominal exam elicited tenderness in the right upper quadrant without rebound or guarding and a negative Murphy’s sign.
Pertinent laboratory data can be found in Table 1. Interferon-gamma release assay (IGRA) QuantiFERON Gold Plus I blood test was negative. Testing for COVID-19, influenza (A and B), and respiratory syncytial virus (RSV) were negative.
Table 1: Pertinent laboratory findingsBUN: blood urea nitrogen, CRP: C-reactive protein, BNP: B-type natriuretic peptide, AST: aspartate aminotransferase, ALT: alanine transaminase, ALP: alkaline phosphatase, LDH: lactic dehydrogenase, CPK: creatine phosphokinase, LDH: lactic dehydrogenase, INR: international normalized ratio
<table><tbody><tr><td rowspan="1" colspan="1">Investigation</td><td rowspan="1" colspan="1">Patient values</td><td rowspan="1" colspan="1">Reference values</td></tr><tr><td rowspan="1" colspan="1">BUN</td><td rowspan="1" colspan="1">23 mg/dL</td><td rowspan="1" colspan="1">6-24 mg/dL</td></tr><tr><td rowspan="1" colspan="1">Creatinine</td><td rowspan="1" colspan="1">1.9 mg/dL</td><td rowspan="1" colspan="1">0.7-1.3 mg/dL</td></tr><tr><td rowspan="1" colspan="1">CRP</td><td rowspan="1" colspan="1">5.6 mg/dL</td><td rowspan="1" colspan="1"><0.3 mg/dL</td></tr><tr><td rowspan="1" colspan="1">Hemoglobin</td><td rowspan="1" colspan="1">10.8 g/dL</td><td rowspan="1" colspan="1">13.8-17.2 g/dL</td></tr><tr><td rowspan="1" colspan="1">Hematocrit</td><td rowspan="1" colspan="1">33.7%</td><td rowspan="1" colspan="1">41-50%</td></tr><tr><td rowspan="1" colspan="1">Platelets</td><td rowspan="1" colspan="1">204 x 10<sup>9</sup>/L</td><td rowspan="1" colspan="1">150-450 x 10<sup>9</sup>/L</td></tr><tr><td rowspan="1" colspan="1">Leukocytes</td><td rowspan="1" colspan="1">10.3 x 10<sup>9</sup>/L</td><td rowspan="1" colspan="1">4.5-11 × 10<sup>9</sup>/L</td></tr><tr><td rowspan="1" colspan="1">Troponin</td><td rowspan="1" colspan="1"><0.012 ng/mL</td><td rowspan="1" colspan="1"><0.04 ng/mL</td></tr><tr><td rowspan="1" colspan="1">BNP</td><td rowspan="1" colspan="1">113 pg/mL</td><td rowspan="1" colspan="1"><100 pg/mL</td></tr><tr><td rowspan="1" colspan="1">AST</td><td rowspan="1" colspan="1">4608 U/L</td><td rowspan="1" colspan="1">8-33 U/L</td></tr><tr><td rowspan="1" colspan="1">ALT</td><td rowspan="1" colspan="1">2134 U/L</td><td rowspan="1" colspan="1">7-56 U/L</td></tr><tr><td rowspan="1" colspan="1">ALP</td><td rowspan="1" colspan="1">105 U/L</td><td rowspan="1" colspan="1">44-147 U/L</td></tr><tr><td rowspan="1" colspan="1">LDH</td><td rowspan="1" colspan="1">5,299 U/L</td><td rowspan="1" colspan="1">105-233 U/L</td></tr><tr><td rowspan="1" colspan="1">Total protein</td><td rowspan="1" colspan="1">5.2 g/dL</td><td rowspan="1" colspan="1">6.0-8.3 g/dL</td></tr><tr><td rowspan="1" colspan="1">Albumin</td><td rowspan="1" colspan="1">2.6 g/dL</td><td rowspan="1" colspan="1">3.4-5.4 g/dL</td></tr><tr><td rowspan="1" colspan="1">CPK</td><td rowspan="1" colspan="1">479 mcg/L</td><td rowspan="1" colspan="1">10-120 mcg/L</td></tr><tr><td rowspan="1" colspan="1">LDH</td><td rowspan="1" colspan="1">5,299 U/L</td><td rowspan="1" colspan="1">140-280 U/L</td></tr><tr><td rowspan="1" colspan="1">INR</td><td rowspan="1" colspan="1">1.81</td><td rowspan="1" colspan="1"><1.1</td></tr></tbody></table>The initial ECG (Figure 1) demonstrated sinus tachycardia with a shortened PR interval and variation in the amplitude of the R wave consistent with electrical alternans. Computerized tomography (CT) with contrast of the chest, abdomen, and pelvis revealed large bilateral pleural effusions (Figure 2), a large pericardial effusion (Figure 3), and hepatic congestion with a nutmeg appearance. In addition, there was enhancing prominent mediastinal lymphadenopathy and an enlarged right hilar lymph node concerning for a neoplastic process.
Electrical alternans on initial ECG
Bilateral pleural effusions (white arrows) with prominent right hilar lymph node (red arrow) visualized on CT
Large pericardial effusion visualized on CT
An echocardiogram reported a left ventricular ejection fraction of 55-60%. There was a large pericardial effusion (Figure 4), and the inferior vena cava was dilated and lacked inspiratory variation (Figure 5), indicating cardiac tamponade.
Large pericardial effusion visualized on echocardiography
Dilated inferior vena cava visualized on echocardiography
A pericardiocentesis was immediately performed. Approximately 1 liter of hemorrhagic fluid was removed. Cell counts of the pericardial aspirate can be found in Table 2. Malignant cells were found on cytological analysis of the fluid.
Table 2: Pericardial fluid analysisRBC: red blood cell, LDH: lactate dehydrogenase
<table><tbody><tr><td rowspan="1" colspan="1">Investigation </td><td rowspan="1" colspan="1">Patient values </td><td rowspan="1" colspan="1">Reference values</td></tr><tr><td rowspan="1" colspan="1">RBC</td><td rowspan="1" colspan="1">2,049,527/mm<sup>3</sup> </td><td rowspan="1" colspan="1">0</td></tr><tr><td rowspan="1" colspan="1">Nucleated cells</td><td rowspan="1" colspan="1">8,318/mm<sup>3</sup> </td><td rowspan="1" colspan="1"><200/mm<sup>3</sup> </td></tr><tr><td rowspan="1" colspan="1">LDH</td><td rowspan="1" colspan="1">5299 U/L</td><td rowspan="1" colspan="1">141-2613 U/L</td></tr><tr><td rowspan="1" colspan="1">Glucose</td><td rowspan="1" colspan="1">14 mg/dL</td><td rowspan="1" colspan="1">80-134 mg/dL</td></tr></tbody></table>An ECG obtained following the procedure showed sinus tachycardia and resolution of the electrical alternans (Figure 6).
Repeat ECG obtained after pericardial fluid drainage without R wave amplitude variation
The patient was placed on colchicine and furosemide as adjuvant therapies.
A CT of the chest with contrast two days after admission revealed prominent mediastinal lymphadenopathy and an enlarged, enhancing left supraclavicular lymph node. In addition, several small pulmonary nodules in the right lung were identified. The investigation continued with a biopsy of the right hilar lymph node. Pathological findings indicated poorly differentiated infiltrative non-small cell carcinoma (Figure 7) with immunohistochemistry staining, suggesting a pulmonary origin (Figures 8, 9).
Hematoxylin and eosin-stained tissue section shows a poorly differentiated infiltrative non-small cell carcinoma (H&E; 200x)
Keratin 7-positive immunohistochemistry staining favors pulmonary origin adenocarcinoma (IHC; 200x)
Thyroid transcription factor 1-positive immunohistochemistry staining favors pulmonary origin adenocarcinoma (IHC; 200x)
Our patient’s symptoms progressively improved over the next few days. The aspartate aminotransferase (AST) and alanine aminotransferase (ALT) improved to 82 U/L and 265 U/L, respectively.
Oncology was consulted and made recommendations for treatment. The patient declined further intervention and decided to pursue outpatient palliative care. He was discharged from the hospital in stable condition.
Discussion
Electrical alternans is an ECG finding often associated with large pericardial effusions [3]. The sign is defined as an alternating height of electrical complexes arising from the same pacemaking site. Any ECG wave can show this change, but it is most often observed with the QRS complex [1]. A mechanism that contributes to this finding is the pendular motion of the heart throughout the cardiac cycle from accumulated pericardial fluid [4]. Although electrical alternans is typically associated with pericardial effusion, it has also been observed in other pathologies, such as immediately preceding ventricular fibrillation and during catecholaminergic states [5]. If the finding is associated with pericardial effusion, it can disappear following adequate drainage [6].
Large pericardial effusions result in cardiac tamponade in about 25% of cases [7]. A weakened apical pulse, distant heart sounds, pulsus paradoxus, and narrow pulse pressure mark the syndrome. Cardiac tamponade results in a life-threatening state of reduced venous return and impaired diastolic functioning. The ensuing shock can be fatal [7].
There are many etiologies of pericardial effusion. Pericarditis, autoimmune disease, and malignancy are frequent causes. Malignant involvement of the pericardium is common, but the treatment of the malignancy itself is another possible culprit [8].
The diagnosis of cardiac tamponade requires a high degree of clinical suspicion. ECG can be a vital tool in diagnosis. Signs indicating cardiac tamponade include low QRS voltage, PR segment depression, sinus tachycardia, and electrical alternans. An echocardiogram could report a swinging heart, right atrial systolic collapse, right ventricular free wall diastolic collapse, enlarged and non-pulsatile inferior vena cava, and the presence of fluid in the pericardial space. Advanced imaging techniques are occasionally used. A CT or MRI may show deformed cardiac chambers and distention of the vena cava [9].
Cardiac tamponade requires immediate drainage to avoid life-threatening complications. Ultrasound-guided pericardiocentesis is an effective procedure to alleviate this condition. Fluid removal should be less than 1 liter to avoid right ventricular dilation that can result in profound hypotension. Other possible treatment options include subxiphoid surgical drainage, pericardial window technique, and left anterior minithoracotomy [10]. There is evidence that pericardiocentesis followed by continuous negative pressure drainage via a pigtail catheter can result in better patient outcomes [11].
The optimal management of malignant pericardial effusion is debated. The creation of a pericardial window is frequently used to prevent effusion recurrence. Despite this definitive procedure, the prognosis is extremely poor in the postoperative period. Most patients with malignant effusion experience only three months of survival [12]. Adjuvant therapy to prevent effusion recurrence includes systemic or intrapericardial antineoplastics or anti-inflammatory medications. Colchicine was used in our patient. This drug is highly beneficial in inflammatory pericardial effusion but has shown limited success in malignant effusion [13].
Conclusions
Electrical alternans is a unique ECG finding often associated with large pericardial effusions. Our patient presented in cardiac tamponade with electrical alternans on ECG. After adequate pericardial fluid drainage, the sign resolved. Further evaluation resulted in a diagnosis of lung adenocarcinoma. Our patient decided to pursue palliative care in the outpatient setting after inpatient stabilization. Pericardial effusion resulting in cardiac tamponade has many etiologies. Although optimal chronic care of malignant pericardial effusion is debated, acute treatment requires drainage of pericardial fluid to avoid life-threatening complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Total electrical alternans in a patient with malignant pericardial tamponade BMJ Case Rep Verlaan D Veltman JD Grady B 2018201810.1136/bcr-2018-224771 PMC 605810430030246 · doi ↗ · pubmed ↗
- 2Electrocardiographic changes in pericardial effusion Chest Meyers DG Bagin RG Levene JF 142214261041993822279910.1378/chest.104.5.1422 · doi ↗ · pubmed ↗
- 3Electrical alternans: a sign, not a diagnosis South Med J Goyal M Woods KM Atwood JE 48548910620132391214610.1097/SMJ.0b 013e 3182 a 1456 c · doi ↗ · pubmed ↗
- 4The swinging heart: cardiac alternans and right ventricular collapse in classic tamponade Can J Cardiol Olearczyk BM Chongkrairatanakul T Menzies DJ 2402520091934035210.1016/s 0828-282x(09)70080-7PMC 2706766 · doi ↗ · pubmed ↗
- 5Electrical alternans and vulnerability to ventricular arrhythmias N Engl J Med Rosenbaum DS Jackson LE Smith JM Garan H Ruskin JN Cohen RJ 2352413301994827208410.1056/NEJM 199401273300402 · doi ↗ · pubmed ↗
- 6Mechanism of electrical alternans in patients with pericardial effusion Cathet Cardiovasc Diagn Rinkenberger RL Polumbo RA Bolton MR Dunn M 63704197864777510.1002/ccd.1810040109 · doi ↗ · pubmed ↗
- 7Cardiac tamponade revisited: a postmortem look at a cautionary case Tex Heart Inst J Ariyarajah V Spodick DH 347351342007 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 1995065/17948086 PMC 1995065 · pubmed ↗
- 8Neoplastic cardiac tamponade Intern Med Osawa T Tajiri K 244724486220233664252510.2169/internalmedicine.1294-22PMC 10518545 · doi ↗ · pubmed ↗