The Prevalence and Distribution of Osteopathic Chief Residents in Emergency Medicine
Emma Wandro, Sahar Rammaha, Kevin McGurk

TL;DR
This study examines how often osteopathic doctors become chief residents in emergency medicine programs and finds they are overrepresented in leadership roles.
Contribution
The study quantifies the overrepresentation of D.O.s in chief resident roles relative to their overall presence in emergency medicine residencies.
Findings
29.4% of chief residents were D.O.s despite comprising only 25.4% of all residents.
D.O. chief residents were more common in programs with higher proportions of D.O. trainees and osteopathic program directors.
82.1% to 87.8% of EM residencies reported data on chief residents and their medical degrees.
Abstract
Background The chief resident position fulfills important administrative and educational functions for emergency medicine (EM) residency programs and has been associated with advanced academic and career opportunities. This study seeks to determine the prevalence and distribution of Doctor of Osteopathic Medicine (D.O.) and allopathic Doctor of Medicine (M.D.) degrees among chief residents within EM residencies. Methodology EM residency program websites, affiliated social media accounts on X (formerly Twitter) and Instagram, and program coordinator surveys were used to collect data, including the number of current residents, chief residents, and the listed medical degrees for residents and program directors during the 2021-2022 and 2022-2023 academic years. A Pearson’s chi-square test was used to compare the number of residents, chief residents, and program directors by medical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
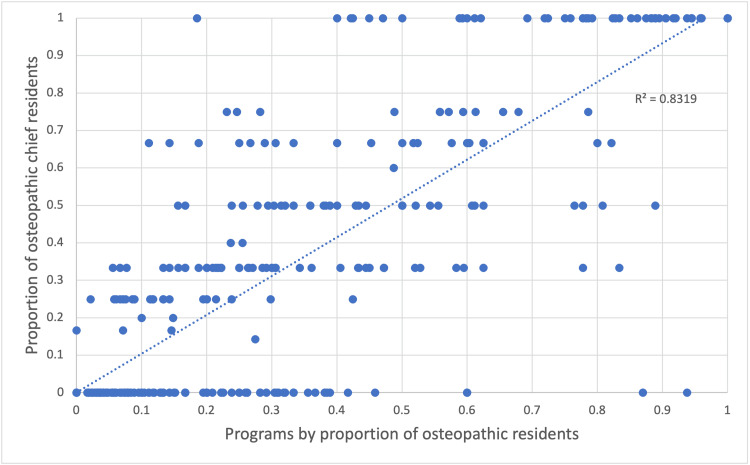 Figure 1
Figure 1| 2021–2022 | 2022–2023 | P-valuea | |
| Included programs | 188/229 (82.1%) | 201/229 (87.8%) | 0.0895 |
| Osteopathic residents | 1,776/7,051 (25.2%) | 1,900/7,436 (25.6%) | 0.6153 |
| Osteopathic chief residents | 182/593 (30.7%) | 180/637 (28.3%) | 0.3493 |
| Osteopathic program directors | 37/188 (19.7%) | 40/201 (19.9%) | 0.9567 |
| Programs without an osteopathic resident | 33/188 (17.6%) | 30/201 (14.9%) | 0.4820 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Diversity and Career in Medicine · Medical Education and Admissions
Introduction
The chief resident position fulfills important administrative and educational functions for emergency medicine (EM) residency programs [1-3]. Residents serving in this role often receive additional training and hone leadership and administrative skills that are beneficial to their career pursuits [2]. The position helps prepare trainees for future academic roles and is associated with an increased likelihood of a career in academic medicine [2,4]. Chief residents are typically selected based on multiple factors, including program director, faculty, and co-resident input. While prior studies have examined demographics, including gender and age among chief residents, little is known about the distribution between those with Doctor of Osteopathic Medicine (D.O.) and allopathic Doctor of Medicine (M.D.) degrees among this cohort [4-7]. Given the impact of the chief resident role on future academic and career prospects, a disparity between allopathic and osteopathic chiefs could contribute to broader representation issues within specialty leadership and academia. This study seeks to determine the prevalence and distribution of osteopathic chief residents within EM residencies.
Materials and methods
We performed a retrospective observational study evaluating the number of osteopathic and allopathic residents, chief residents, and program directors in EM residencies across the United States. The Society for Academic Emergency Medicine program directory was used to compile a list of EM residencies accredited by the Accreditation Council for Graduate Medical Education for the 2021-2022 and 2022-2023 academic years. Programs that are no longer operational, new programs without a senior class of residents, and international programs were excluded from the study. Publicly available program websites and their affiliated social media accounts onX (formerly Twitter) and Instagram were used to collect data, including the number of current residents, chief residents, and the listed medical degrees for residents, chief residents, and program directors during the 2021-2022 and 2022-2023 academic years. When unlisted, program coordinators were surveyed for the same information.
After a brief training to standardize collection, data acquisition occurred between November 30, 2021, and December 31, 2021, and again over the same period for 2022. Dates were selected to follow the typical periods for chief selection (traditionally in the spring) and the summer transition of incoming and graduating residents. Reliability between the two observers was assessed on a 20-program sample using Cohen’s kappa. Linear regression analysis was used to assess the association between the proportion of D.O. residents within a program and the number of D.O. chief residents within a program. Subgroup analysis was then performed by separating programs by their proportion of D.O. residents into discrete quintiles (0-20%, 21-40%, 41-60%, 61-80%, and 81%-100%) and comparing the proportion of D.O. chiefs to D.O. residents by quintile.
Descriptive statistics and Pearson’s chi‐square test were performed using Excel (Microsoft Corporation, Redmond, WA, USA). Statistical significance was defined as p-values ≤0.05. This study was exempted from review by the Medical College of Wisconsin Institutional Review Board.
Results
Interobserver agreement was excellent with a kappa coefficient of 1.0. A total of 188/229 (82.1%) and 201/229 (87.8%) eligible EM residencies identified their current chief residents and the medical degrees of their trainees for the 2021-2022 and 2022-2023 academic years, respectively. Of the 14,487 EM residents included, 3,676 (25.4%) were osteopathic physicians. The median number of chief residents per program was three with a range from one to seven. Of the 1,230 chief residents identified, 362 (29.4%) were D.O.s.
A total of 37/188 (19.6%) and 40/201 (19.9%) of the included program directors for the 2021-2022 and 2022-2023 academic years, respectively, were osteopathic physicians. Among programs with M.D. program directors, 215/1,035 (20.8%) of chief residents and 2,188/12,371 (17.7%) of total residents were D.O.s. At programs with D.O. program directors, 147/195 (75.4%) of chief residents and 1,488/2,116 (70.3%) of total residents were osteopathic physicians.
The proportion of D.O. chief residents was higher than both the proportion of D.O. residents (29.4% vs. 25.4%, p = 0.002) and D.O. program directors (29.4% vs. 19.8%, p <0.001) in EM residencies.
The proportion of D.O. residents, chief residents, and program directors was similar between the 2021-2022 and 2022-2023 cohorts, as shown in Table 1.
Table 1: Trend in osteopathic residency leadership in emergency medicine 2021-2023.a: P-values from the chi-square test of independence. Statistical significance is defined by p-values ≤0.05.
<table><tbody><tr><td rowspan="1" colspan="1"> </td><td rowspan="1" colspan="1">2021–2022</td><td rowspan="1" colspan="1">2022–2023</td><td rowspan="1" colspan="1">P-value<sup>a</sup> </td></tr><tr><td rowspan="1" colspan="1">Included programs</td><td rowspan="1" colspan="1">188/229 (82.1%)</td><td rowspan="1" colspan="1">201/229 (87.8%)</td><td rowspan="1" colspan="1">0.0895</td></tr><tr><td rowspan="1" colspan="1">Osteopathic residents</td><td rowspan="1" colspan="1">1,776/7,051 (25.2%)</td><td rowspan="1" colspan="1">1,900/7,436 (25.6%)</td><td rowspan="1" colspan="1">0.6153</td></tr><tr><td rowspan="1" colspan="1">Osteopathic chief residents</td><td rowspan="1" colspan="1">182/593 (30.7%)</td><td rowspan="1" colspan="1">180/637 (28.3%)</td><td rowspan="1" colspan="1">0.3493</td></tr><tr><td rowspan="1" colspan="1">Osteopathic program directors</td><td rowspan="1" colspan="1">37/188 (19.7%)</td><td rowspan="1" colspan="1">40/201 (19.9%)</td><td rowspan="1" colspan="1">0.9567</td></tr><tr><td rowspan="1" colspan="1">Programs without an osteopathic resident</td><td rowspan="1" colspan="1">33/188 (17.6%)</td><td rowspan="1" colspan="1">30/201 (14.9%)</td><td rowspan="1" colspan="1">0.4820</td></tr></tbody></table>The proportion of osteopathic chief residents within a program largely mirrored the proportion of D.O. residents in those programs, as shown in Figure 1. Linear regression yielded a coefficient of determination, r^2^ = 0.83 (r = 0.91; p < 0.0001).
Distribution of osteopathic chief residents 2021-2023.
When stratified into quintiles by the proportion of the residency comprising D.O.s, the percentage of osteopathic chief residents was marginally higher than the percentage of osteopathic residents in all but the highest quintile. More than half of all programs had resident rosters with fewer than 20% osteopathic residents. Among these programs, 483/8,325 (5.8%) of residents and 53/670 (7.9%) of chief residents were D.O.s. In both academic years studied, at least 30 programs included no osteopathic trainees. At residencies comprising 21-40% osteopathic residents, 726/2,517 (28.8%) of residents and 69/232 (29.7%) of chief residents were D.O.s. At programs with 41-60% osteopathic trainees, 819/1,632 (50.2%) of residents and 81/143 (56.6%) of chief residents were D.O.s. At those with 61-80% osteopathic trainees, 628/901 (69.7%) of residents and 63/80 (78.6%) of chief residents held osteopathic degrees. At programs with more than 80% D.O.s, 1,006/1,094 (92.0%) of residents and 94/103 (91.3%) of chief residents held osteopathic degrees.
Most programs excluded for missing data only failed to identify their chief residents. For 2022-2023, 21 of 28 programs with incomplete data listed the degrees of their trainees and program directors but not their chief residents. Collectively, D.O.s comprised a similar percentage of program directors (19.0% vs. 19.9%) and a modestly increased proportion of residents (33.2% vs. 25.6%) at the excluded versus included programs, respectively.
Discussion
The proportion of D.O.s serving in the role of chief resident is higher than the overall proportion of EM residents with osteopathic degrees. At residencies with D.O. program directors, trainees and chief residents are more likely to be osteopathic physicians. Unsurprisingly, residencies with a larger proportion of osteopathic residents have a larger proportion of osteopathic physicians as chief residents.
The results demonstrate that osteopathic residents are no less likely to be selected as chief residents than their allopathic peers. However, the distribution of osteopathic residents across programs is decidedly asymmetric and supports the notion that certain programs are D.O. friendly while others are not [8-11]. More than half of all EM trainees are educated in programs with <10% D.O.s, including at least 30 residencies with no osteopathic residents. D.O.s training in this cohort of programs were overrepresented in the chief role (7.9% of chief residents vs. 5.8% of residents overall). This suggests that for many D.O.s, a limiting factor may not be finding success within a program but rather matching into it. While the percentage of programs with no D.O. trainees decreased from 2021-2022 to 2022-2023, the change was nominal (17.6% to 14.9%, p = 0.482). As the national landscape changes and the overall popularity and competitiveness of the specialty evolves, so too may the prevalence of osteopathic physicians in residency positions and leadership roles. The striking decrease in EM applicants seen for the 2023 match cycle may compel programs with few or no D.O. residents to re-evaluate how they evaluate and rank these applicants [12].
While there are slight differences between osteopathic and allopathic EM resident U.S. Medical Licensing Examination (USMLE) Step 1 scores (mean of 228 and 233, respectively), this is unlikely to fully explain the degree of variable osteopathic representation across residencies [13,14]. Several other factors likely contribute, including applicant self-selection, access to appropriate mentorship, and availability of home EM rotations affiliated with applicants’ medical schools [9-11]. Prior studies have also indicated some programs do not match osteopathic applicants due to concerns about the quality of their medical education or how osteopathic trainees might impact the reputation of the program [9].
Although the chief resident role has been associated with future academic medical careers, it is unclear whether this is as true for osteopathic trainees. While serving as chief resident may afford an individual more academic opportunities, a wide gap persists in traditional post-residency metrics for success in academic medicine between D.O.s and M.D.s. Though osteopathic physicians comprised 29.4% of chief residents in our study, they make up <1% of editorial positions for major medical journals, <3% of authors in major EM journals, and <3% of major EM research grant recipients [15-18]. The factors contributing to this gap, despite the proportional representation of D.O.s as chief residents, are unknown.
Limitations
This study relied upon publicly available data and/or program coordinator survey responses. As some residencies did not report all necessary information, a mean of 14.8% of programs were excluded from the analysis. While we do not believe this meaningfully changes the conclusions drawn, a fuller representation of EM programs may have altered some statistical considerations.
Our study compared M.D. and D.O. representation but could not make a distinction between graduates of U.S. medical schools and international medical graduates (IMGs) with M.D.s. IMGs face larger challenges matching and have lower mean USMLE scores than U.S. medical graduates. Residents with non-D.O. or -M.D. degrees (i.e., M.B.B.S.) were excluded from the analysis but make up an exceedingly small portion of current EM trainees nationwide [19]. We believe this is unlikely to have skewed results.
Conclusions
Osteopathic residents are asymmetrically distributed across EM residencies with program composition ranging from no D.O.s to 100% D.O. residents. Unsurprisingly, D.O.s are most likely to serve as chief residents at programs with a higher proportion of D.O. trainees and at programs with osteopathic program directors. However, the proportion of D.O. chief residents was higher than the proportion of D.O. residents within EM training programs. This was true even at programs with few D.O. residents, suggesting that for many D.O.s a limiting factor may not be finding success within a program but rather matching into it. Despite proportional over-representation in the chief resident role, D.O.s remain under-represented in other academic leadership roles and as recipients of grant funding. This disparity warrants further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chief resident skills: a study on resident perceptions of skill importance and confidence Spartan Med Res J Van Order T Wisniewski SJ 6466320183365513010.51894/001c.6466 PMC 7746022 · doi ↗ · pubmed ↗
- 2The chief resident role in emergency medicine residency programs West J Emerg Med Hafner JW Gardner JC Boston WS Aldag JC 120125112010 https://pubmed.ncbi.nlm.nih.gov/20823957/20823957 PMC 2908642 · pubmed ↗
- 3Qualities important in the selection of chief residents Cureus Turner J Litzau M Mugele J Pettit K Sarmiento EJ Humbert A 012202010.7759/cureus.7580 PMC 720535832391229 · doi ↗ · pubmed ↗
- 4Academic springboard: the chief resident position correlates with career path in emergency medicine AEM Educ Train Jordan J Hopson LR Clarke SO 05202110.1002/aet 2.10639 PMC 836474134435169 · doi ↗ · pubmed ↗
- 5Six years of gender equity in emergency medicine chief resident selection AEM Educ Train Farrell KJ Walker LE Battaglioli N Heaton HA Lohse C Sadosty AT 05202110.1002/aet 2.10595 PMC 803563233869983 · doi ↗ · pubmed ↗
- 6Diversity begets diversity: factors contributing to emergency medicine residency gender diversity AEM Educ Train Saak JC Mannix A Stilley J Sampson C 055202110.1002/aet 2.10676 PMC 848048934616976 · doi ↗ · pubmed ↗
- 7Emergency Medicine Gender in Resident Leadership Study (EM GIRLS): the gender distribution among chief residents AEM Educ Train Mannix A Parsons M Krzyzaniak SM Black LP Alvarez A Mody S Gottlieb M 262265420203270459610.1002/aet 2.10436 PMC 7369478 · doi ↗ · pubmed ↗
- 8Characteristics of ACGME residency programs that select osteopathic medical graduates J Grad Med Educ Beckman JJ Speicher MR 4354401220203287968310.4300/JGME-D-19-00597.1PMC 7450739 · doi ↗ · pubmed ↗